
Abstract
Although the Virchow's triad on thrombosis includes reduced blood flow as a factor, there has been relatively little data on the importance of total cerebral blood flow on the risk of subsequent stroke. In the current study, we investigate whether total cerebral blood flow helps predict stroke recurrence. Extracranial arterial blood flow volume estimated by color velocity imaging quantification ultrasound (CVIQ) is an index of cerebral blood flow measurement. We performed a cohort study of 210 consecutive acute stroke patients. Patients were studied with transcranial Doppler and duplex ultrasound for intra- and extracranial large artery disease within 3 days of symptom onset. The association between the risk of recurrent stroke and CVIQ was analyzed with Cox proportional hazards model. Thirty-nine patients (17.7%) developed an ischemic stroke during a mean follow-up of 47.5 months. The mean extracranial blood flow volume was significantly lower for patients who had a recurrent stroke than those without (594.4 ± 130.3 versus 683.8 ± 176.9mL/min; P = 0.003). In a Cox proportional hazards model adjusting for potential confounding variables, extracranial blood flow volume (hazard ratio (HR) for lowest tertile, 4.1; 95% confidence interval (CI), 1.5 to 11.0) along with male sex (HR, 2.5; 95% CI, 1.3 to 5.1), diabetes (HR, 2.5; 95% CI, 1.2 to 5.0) and large artery stenosis (HR, 2.2; 95% CI, 1.1 to 4.4) were independent predictors for stroke recurrence. Our data indicated that patient with low amount of blood flow to the brain is at risk of recurrent stroke.
Introduction
Stroke recurrence is an important public health concern (Sacco et al, 1997). Despite the use of antithrombotic agent and control of risk factors, recurrent stroke remains common (Hardie et al, 2004). Stroke is a heterogeneous disease with a variety of pathophysiological mechanisms. Possible mechanisms for cerebral infarctions include hypoperfusion, artery-to-artery embolism or a combination of these two factors. Hypoperfusion to the brain can be regional or total, mainly because of reduced blood flow caused by obstruction of extracranial and intracranial large and small arteries. Although the Virchow's triad on thrombosis includes reduced blood flow as a factor, there has been relative little data on the importance of total cerebral blood flow on the risk of subsequent stroke.
Available data strongly link hypoperfusion with the occurrence of ischemic stroke. Severity of stenosis is a well-known major risk factor of stroke in patients with symptomatic or asymptomatic carotid artery disease (Hennerici et al, 1987; MRC European Carotid Surgery Trial: interim results for symptomatic patients with severe (70 to 99%) or with mild (0 to 29%) carotid stenosis. European Carotid Surgery Trialists' Collaborative Group, 1991; Norris and Zhu 1992; North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis 1991). Recent studies reported a significant ipsilateral cerebral perfusion deficit in patients with moderate to severe cartiod artery stenosis (Moftakhar et al, 2005; Trivedi et al, 2005). Moreover, degree of stenosis was found to be a strong predictor of the presence of perfusion abnormality (Moftakhar et al, 2005). Methods for measurement of cerebral perfusion include xenon CT, Single Photon Emission Computed Tomography (SPECT), and Positron Emission Tomography (PET) and MRI perfusion. Such techniques often require a contrast agent and are relatively expensive. Another study reported that among 100 patients continuously monitoring middle cerebral artery (MCA) blood flow velocities as a reflection of brain perfusion during heart surgery, the reduction in baseline blood flow velocities was 17% for patients who had no neurological deficits and 43% for those who had stroke (Barbut and Caplan, 1997). However, this technique is well known to suffer significant failure as a result of an impenetrable temporal acoustic window (Gomez et al, 1993; Itoh et al, 1993).
Extracranial arterial blood flow volume estimated by color velocity imaging quantification (CVIQ) ultrasound is a new and noninvasive technique that can reveal total blood flow to the head and neck region, which is an index of total brain perfusion (Ho et al, 2002a; Ho and Metreweli, 2000). In this study, we sought to determine whether extracranial arterial blood flow volume as measured by CVIQ could be predictive for further ischemic stroke in acute stroke patients.
Materials and methods
We performed a prospective cohort study of mild to moderately severe ischemic stroke patients admitted to the Prince of Wales Hospital in Hong Kong, a regional general hospital with accident and emergency service. Patients with acute ischemic stroke admitted to our department from January 1, 1998 to December 31, 2000 were studied. Patients were included in the study if the following criteria were fulfilled: rapidly developing signs of focal neurological deficit that lasted > 24 h; diagnosis confirmed by a CT scan of the head that excluded bleeding or other alternative diagnosis. All patients underwent a 12-lead electrocardiogram examination. Echocardiography was performed only if there was clinical suspicion of cardiac abnormality such as endocarditis and severe valvular disease. Patients with cardioembolic stroke according to the the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) criteria (Madden et al, 1995) were excluded. Because of the need to be examined at the ultrasonology laboratory, we also excluded patients who required constant bedside monitoring or unable to physically comply with examination because of severe stroke and multiple co-morbidities.
Stroke subtype was classified, without knowing the results of neuroimaging investigations, as total anterior circulation infarct (TACI), partial anterior circulation infarct (PACI), posterior circulation infarct (POCI), or lacunar infarct (LACI) according to a published criteria by Oxfordshire Community Stroke Project (OSCP) (Bamford et al, 1991). The OCSP classification was performed prospectively by a neurologist within 24 h after admission, who reviewed the details of the neurological deficits for each patient. Patients were determined to be with TACI if there were a combination of (i) higher cerebral dysfunction, (ii) homonymous visual field defect and (iii) ipsilateral motor/sensory deficit of at least two areas of the face, arm and leg. Patients with PACI were determined because they presented with only two of the three components of TACI, or with higher cerebral dysfunction alone. POCI was determined if there were sign of posterior circulation dysfunction including ipsilateral cranial nerve palsy with contralateral motor/ sensory deficit, bilateral motor/sensory deficit, disorder of conjugate eye movement, cerebellar dysfunction without ipsilateral long-tract deficit, or isolated homonymous visual field defect. LACI was determined if there was a pure motor or sensory stroke, sensori-motor stroke, or ataxic hemiparesis.
Baseline Characteristics
Baseline demographic, clinical details, and medical history were recorded. Detailed information on risk factors has been reported previously (Wong, 1999). Assessment of stroke severity was performed by certified clinicians using the National Institutes of Health Stroke Scale (NIHSS) after admission. We also noted the use of antithrombotics at the time of discharge from acute hospital or at any time during follow-up.
Ultrasound Examination
All enrolled patients were examined by transcranial Doppler (TCD) and extracranial duplex ultrasound investigation within 3 days of neurological symptom onset. The intracranial large arteries and extracranial carotid arteries were investigated, including bilateral middle cerebral arteries, anterior cerebral arteries, posterior cerebral arteries from temporal window, siphon segments of internal carotid artery from orbital window, vertebrobasilar arteries from suboccipital approach, and extracranial internal carotid arteries. TCD examination was conducted by use of a standardized protocol based on a principle published previously (Ho et al, 2002a) and we diagnosed intracranial large artery occlusive disease as previously reported (Babikian and Wechsler 1993; Wong, 1999; Wong et al, 2000). In addition, a duplex color Doppler examination of the carotid arteries was also performed. We recorded any stenosis greater than 50% diameter reduction as estimated either by peak systolic velocity ratio greater than 1.5 (a ratio of the peak systolic velocity at the internal carotid artery stenosis to that at the ipsilateral common carotid artery) or by direct measurement of the stenosis on the static image if the true and residual lumen could be clearly depicted. Patient was classified as having relevant large artery disease if there was evidence of arterial stenosis which could explain its neurological deficits.
We adopted standardized CVIQ technique in the measurement of extracranial blood flow volume. The examination was performed with a 7.5 MHz liner transducer of Philips SD800 ultrasound unit (Best, Netherlands), which has a standard feature of Duplex Doppler imaging as well as a software for blood flow volume measurement by using CVIQ technique. The technical details have been described previously (Ho et al, 2002b). Extracranial blood flow volume was defined as the sum of the blood flow volume in both common carotid arteries and vertebral arteries.
Recording of Stroke Recurrence
The specified outcomes were the occurrence of further ischemic stroke. Stroke recurrence was defined as either a new neurological deficit with a confirmed new infarct relevant to clinical symptom on brain CT scan or a deterioration of the previous deficit not considered to be because of edema, hemorrhagic transformation, or intercurrent illness. Only recurrences 21 days after the index stroke or, if earlier, clearly in another vascular terrioity were included. Each recurrent stroke was reviewed by a physician unaware of the results of the ultrasound study.
Follow-up
Patients were followed up in our outpatient clinic every 6 months. These visits were supplemented by monthly follow-up telephone calls to the patient. The follow-up period was defined as the time from admission because of the index stroke until either a recurrent stroke, death, or the indexed date of September 30, 2004.
Statistical analyses
Baseline comparisons were made with the Student's t-test, the Mann—Whitney U-test or the χ2 test as appropriate. To evaluate the role of extracrainal cerebral blood flow volume as predictor of the risk of recurrent ischemic stroke, we divided the patients into three groups according to tertiles of extracranial blood flow volume of all the participants in our study (n = 210). Cox proportional hazards model was used to assess the risk of recurrent stroke, with the group of patients in the highest tertile considered the reference group. Besides extracranial blood flow volume, possible confounders including sex, age hypertension, diabetes mellitus, previous TIA or stroke, large artery stenosis, and history of antithrombotic treatment were included in the model.
All tests were two-sided, and P-values <0.05 were regarded as statistically significant. Statistical analysis was performed with SPSS for Windows (SPSS Inc.).
Results
Baseline Characteristics
During the period from January 1998 to December 2000, 210 acute ischemic stroke patients were enrolled in our study. The mean age of the 210 patients was 69.4 ± 10.5 years (median, 70.0 years; range, 46 to 94); 52.4% were men and 47.6% were women. The risk factor profile is summarized in Table 1. Of the 210 patients in the study cohort, 101 (48.1%) of the patients had large artery disease, among which 34 (16.2%) patients had extracranial artery stenosis, 77 (36.1%) had intracranial stenosis, and 10 (4.8%) patients had tandem lesions. Volumes of extracranial blood flow ranged from 306.0 to 1296.9 mL/min (mean ± s.d., 667.2 ± 172.5 mL/min; median, 658.1 mL/min) and were normally distributed.
Baseline characteristics of study participants
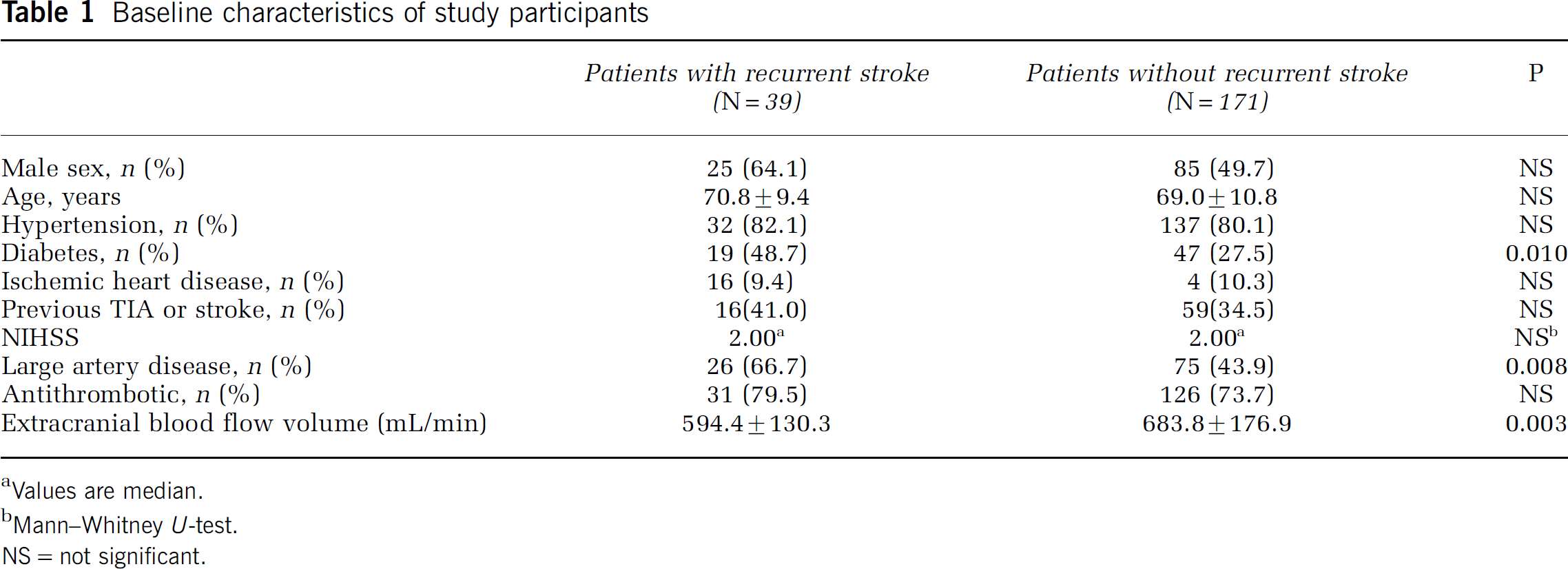
Values are median.
Mann—Whitney U-test.
NS = not significant.
Patients were followed for a mean time of 47.5 ± 20.1 months. No patient was lost to follow up. Thirty-nine patients (17.7%) developed a recurrent ischemic stroke. The cumulative recurrence rate was 11.4% after 1 year and 21.1% after 4 years. Univariate analysis showed that diabetes mellitus, large artery disease, and lower mean extracranial blood flow volume were significant risk factors for recurrent stroke (Table 1). The mean extracranial blood flow volume was significantly lower for patients who had a recurrent stroke than those without (594.4 ± 130.3 versus 683.8 ± 176.9 mL/min; P = 0.003). Percentage of patient with and without stroke recurrence in different tertile levels were depicted in Figure 1. Our study found that patients with lower blood flow tertile had a higher risk of recurrent stroke (χ2 = 9.258; P = 0.01, Figure 1).
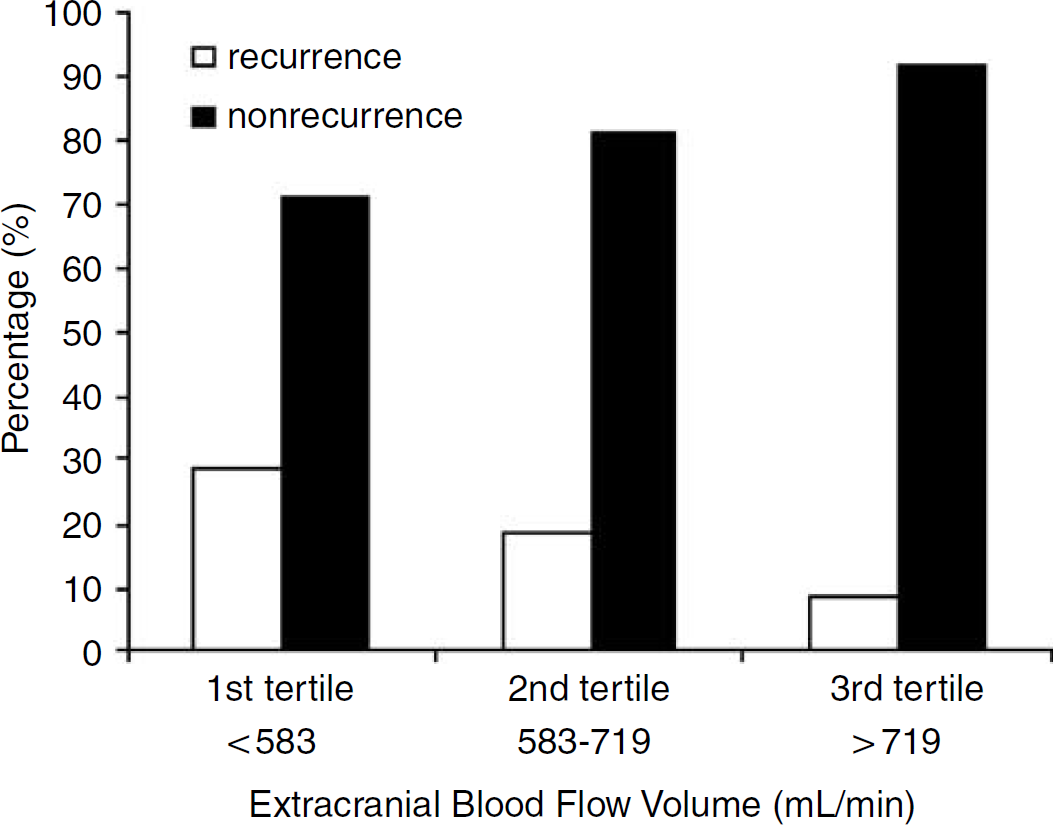
Percentage of patients with and without stroke recurrence by tertile levels.
Multivariate Analysis
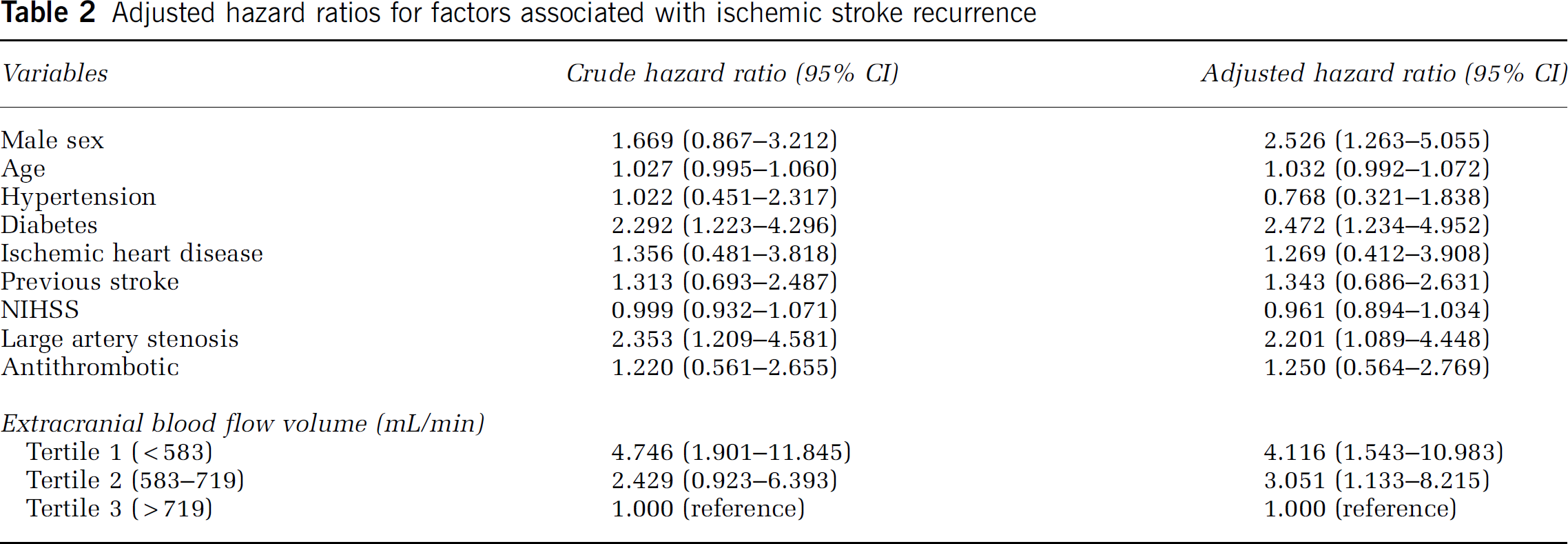
In a model including traditional risk factors and potential confounding variables, male sex, diabetes, large artery disease, and extracranial blood flow volume were the only factors that were independently associated with stroke recurrence (Table 2). In comparison with woman, man had a 2.5-fold greater risk of stroke recurrence (95% CI: 1.3 to 5.1; P = 0.009). Patients with diabetes had a 2.5-fold increased risk of recurrent stroke (95% CI: 1.2 to 5.0; P = 0.011). Large artery stenosis was also an independent risk factor (HR = 2.2; 95% CI: 1.1 to 4.4; P = 0.028). To assess whether there is an association between CVIQ and recurrent stroke, we stratified the blood flow volume by tertiles. Compared with patients in the highest tertile, the hazard ratio for recurrent ischemic stroke of those in the first tertile was 4.1 (95% CI, 1.5 to 11.0; P = 0.005), and for the second tertile, 3.1(95% CI, 1.1 to 8.2; P = 0.027) (Figure 2).
Adjusted hazard ratios for factors associated with ischemic stroke recurrence
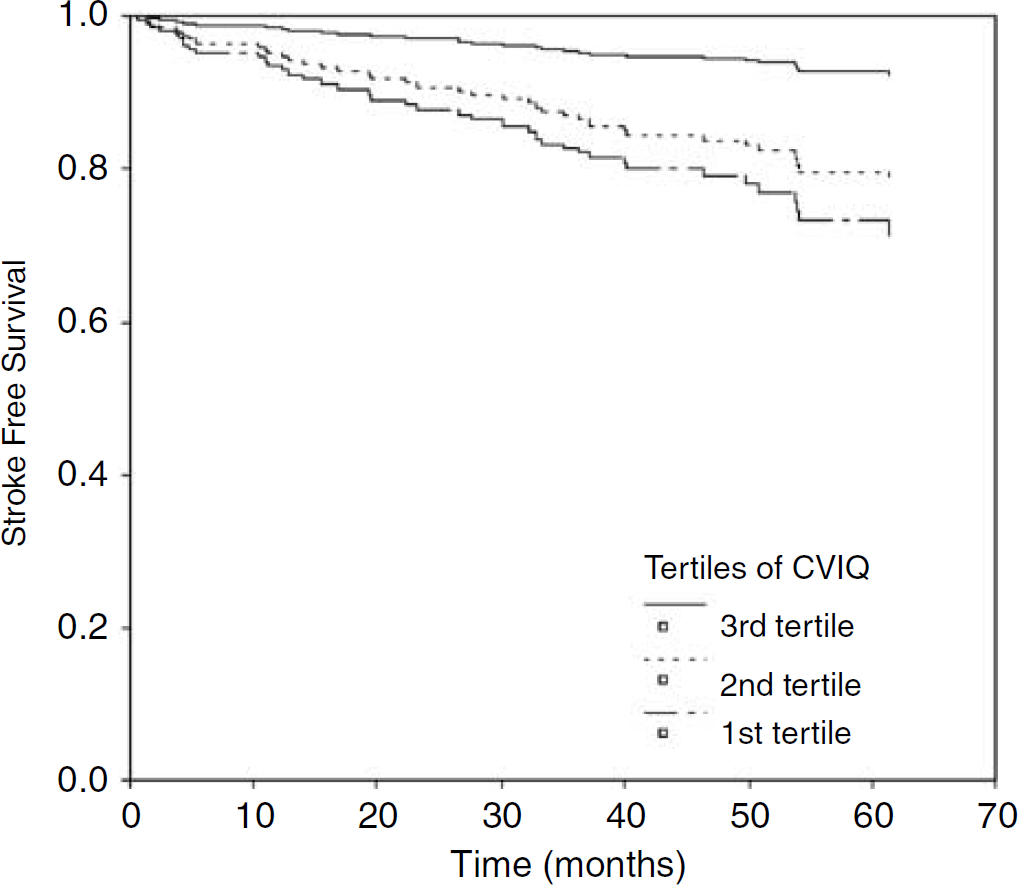
Recurrence of ischemic stroke in patients with different tertiles of extracranial blood flow volume.
Discussion
Our study found that the risk of recurrent ischemic stroke was highest in the first year (11.4%) after the index stroke event, and the cumulative risk rose to 21.1% after 4 years, which was similar to the pattern of cumulative risk observed in other studies (Hardie et al, 2004; Lee et al, 2004). Clinical factors found to influence ischemic stroke recurrence in our study were male sex, diabetes, and large artery disease. Our data are in agreement with previous studies (Hillen et al, 2003; Lee et al, 2004; Wong and Li 2003). To the best of our knowledge, this is the first study to indicate a role for extracranial arterial blood flow volume measured on CVIQ as a predictor for recurrent stroke. Our results provide evidence that decreased blood flow was associated with higher risk of future ischemic stroke. Compared with those in the highest tertile, patients in the lower tertile had > 3-fold higher risk of recurrent stroke. Furthermore, the effect of decreased cerebral blood flow appears to be independent of traditional cerebrovascular risk factors.
CVIQ measurement added approximately 15 mins to the routine examination time of standard carotid duplex examination, which is a routine exam for acute stroke patients in clinical setting. Thus, it may provide a potential useful tool for clinical assessment and identifying the subgroup of patients with high risk of recurrence. In additional, one of our previous study screened stroke patients by TCD and found that the presence and the total number of occlusive arteries in the craninocervical circulation predict further vascular events in patients with intracranial large-artery occlusive disease (Wong et al, 2000). Lack of a good temporal window for insonation of the intracranial artery is a main flaw of the use of TCD in clinical practice. Because intracranial artery stenosis is the predominant vascular lesion found in Asian population, which is also demonstrated in our study cohort, thus, total cerebral blood flow volume measured by CVIQ may serve as an alternative prognostic risk factor.
Although not commercially readily available, CVIQ technique has been validated in our laboratory (Ho et al, 2002a, 2005a; Ho and Metreweli 2000). We opted to use the CVIQ technique instead of the more popular technique to measure blood flow volume (BFV) because it has been shown that CVIQ is more accurate than spectral Doppler technique in the determination of BFV in the carotid arteries, where the BFV is significantly overestimated by spectral Doppler technique (Ho and Metreweli, 2000). Moreover, it is comparable to magnetic resonance angiography with phase contrast flow quantification (Ho et al, 2002a). Our recent study also found that post-stroke extracranial arterial blood flow volume is an independent predictor of functional outcome (Ho et al, 2005b). However, this methodology has shortcomings. Errors may arise from the inaccurate estimation of flow velocity and diameter measurement caused by off-axis sampling, tortuous vessels, turbulent or non-axial flow, poor color setting, and great respiratory vessel movement, which is quite common in stroke patients (Ho et al, 2002a). Therefore, all the measurements in our study were performed by the same experienced vascular technologist (S Ho) with standardized techniques.
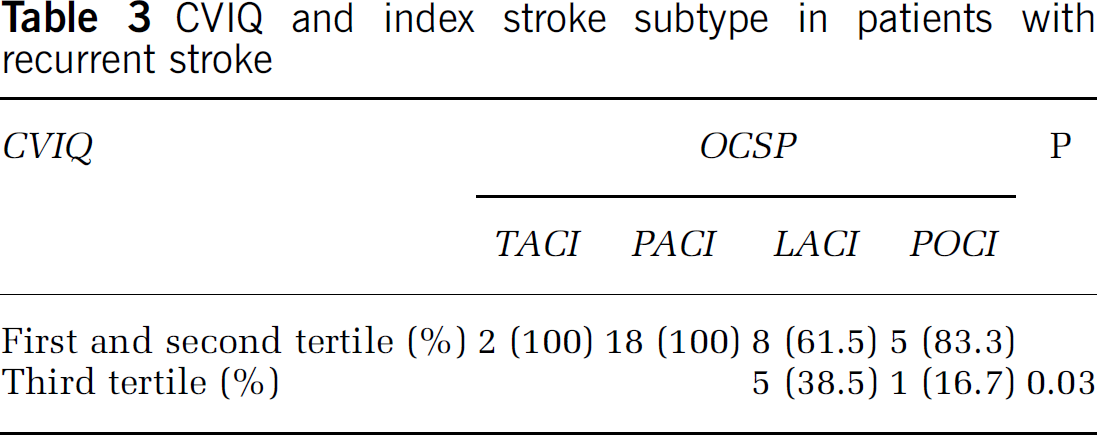
However, the exact mechanism underlying our finding is largely unknown. Brain perfusion is a dynamic process and a key determinant of subsequent brain ischemia. Arterial stenosis may cause hypoperfusion of the focal brain tissue; in additional, narrowing of the arterial lumen stimulate formation of thrombi, which further reduce brain perfusion. Conversely, decreased perfusion reduces the washout of emboli and microemboli that have entered the hypoperfused regions (Caplan and Hennerici, 1998). Therefore, a possible explanation for total cerebral blood flow volume to predict stroke recurrence is that except hypoperfusion caused by atherosclerosis, patients with poor brain perfusion has diminished the ability to clear thromboemboli that are generated, thus may lead to further ischemic stroke. We also measured total blood flow volume from control subjects aged 50 years or above with no history of neurological disease, hypertension, DM, smoking, heart disease, and extracranial plaque formation, the mean CVIQ value was 781.0 (95% CI: 726.5 to 835.5 mL/min) (data unpublished). Our data showed that patients with ischemic stroke had a much lower blood flow volume than controls and those who had a recurrent stroke had a further reduction in CVIQ, which indicated the important role of brain perfusion in the development of ischemic stroke. Furthermore, among 39 recurrent stroke cases, two patients were classified as TACIs (5.1%), 18 patients as PACIs (46.2%), 13 as LACIs (33.3%) and six as POCIs (15.4%) for the index stroke. We further looked at the association between CVIQ and index stroke subtype among those with recurrent stroke. Compared with those in the highest tertile, patients with a reduction in blood flow had a higher risk of recurrence in all subtypes (P = 0.03), especially for those with TACIs and PACIs (Table 3). The finding that low extracrainal blood flow volume was associated with all subtypes of ischemic stroke further suggests the role of hypoperfusion in the pathophysiology of ischemic stroke.
CVIQ and index stroke subtype in patients with recurrent stroke
There are two potential reasons that CBF is reduced in patient with acute stroke: restricted supply because of large vessel disease and reduced demand because of ischemic brain damage. The finding of a relation between whole brain blood flow volume and recurrent stroke could indicate a hemodynamic mechanism that would benefit from flow augmentation or it could just as easily indicate that brains with bigger infracted areas are at higher risk for subsequent stroke. Blood flow measurements alone cannot differentiate. In this study, we did not measure the stroke volume of individual stroke patient and were therefore not able to exclude the possibility that a difference in stroke volume could have contributed to our results. However, a significant difference is unlikely because NIHSS score, which has a correlation with acute magnetic resonance imaging (MRI) stroke volume (Fink et al, 2002), were comparable between the two groups on admission. On the other hand, although patients in the recurrent group in our study had more large artery disease and it was a known risk factor for stroke recurrence, spearman correlation coefficient did not show a close relationship between these two variables (r = 0.061, P = 0.384). Further multivariate analysis showed that conventional risk factors (i.e., diabetic, large artery disease) cannot fully explain all the subsequent ischemic strokes, which is also noted in other studies.
Under such circumstance, some studies tried to find other factors to predict stroke recurrence, that is, homodynamic status evaluated by cerebrovascular reactivity or oxygen extraction fraction or the development of good collateral circulation. Ogasawara et al (2002) reported that decreased cerebrovascular reactivity to acetazolamide determined quantitatively by 133Xe SPECT is an independent predictor of the 5-year risk of subsequent stroke in patient with large artery occlusive disease. Another study using PET scan found that symptomatic carotid occlusive patients with stage II hemodynamic failure (increased oxygen extraction) are at high risk for recurrent stroke (Grubb et al, 1998). Collateral capacity in patients with ICA occlusive disease measured via angiography was also useful in predicting the presence of infarction on CT scans in patients with TIAs (Norris, 1992). However, SPECT, PET scan, and angiography are relatively expensive and not freely available and thus not ideal for regular screening. Because CVIQ is invasive and easily available in our lab, it is ideal for screening and may serve as a complementary method in assessing hemodynamic status of stroke patients.
Our data suggest that the third arm of the Virchow's triad of thrombosis is also an important contributor for stroke. Current strategies for stroke prevention include plaque stabilization with statin and use of antithrombotic agents. Cerebral blood flow augmentation such as use of revascularization may be an important means to prevent stroke in patients who fail to respond to the usual medications.
In conclusion, we provided evidence in the present study for an association between lower volume of extracranial blood flow and risk of recurrent ischemic stroke, even taking into account of large artery disease. This inexpensive and noninvasive hemodynamic imaging parameter may become an innovative predictor for stroke recurrence or an effective screening method in future. However, because of the relatively small sample size of our study, our result should be interpreted cautiously and further studies are required to test its clinical value. It should also be noted that CVIQ measurement performed in the extracrainal arteries is a global index of cerebral perfusion rather than true CBF measurement. Further study comparing this methodology to PET scan, which is a standardized measurement of CBF, is needed to support the reliability of this new technique.