
Introduction
Brain microdialysis during aneurysm surgery was introduced by Landolt et al
1
and has been described more recently by Kett-White et al
2
. Both studies concluded that intraoperative monitoring could detect focal ischaemia in vivo; however, availability of metabolic information about disturbed homeostasis was delayed by least 30 minutes, because of sampling and analysis times. We therefore believe that for results of intraoperative microdialysis to influence patient management and hence outcome, we require:
rapid online analysis of metabolites in a continuous flow of dialysate. a shortened ‘event-to-detection’ time.
Methods
We conducted a prospective study, LREC-approved, on patients requiring surgery for ruptured middle cerebral artery (MCA, n=7) or posterior communicating aneurysms (n=1). Microdialysis catheters (CMA 70) were inserted into cortex at risk of ischaemia after opening the dura. The dialysate fed continuously (via 1 m of fine tubing) into a flow-injection assay for glucose and lactate, each sampled at 30-sec intervals 3 . Outcome was ranked at discharge.
Results
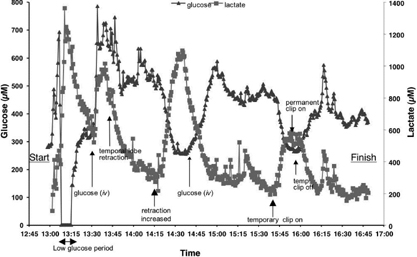
The figure 1 shown is an example of a procedure to clip a left MCA aneurysm, with arrowed annotated events. Note that this patient experienced a period of low dialysate glucose (<150 microM) for 12 minutes, and was given 2 boluses of iv glucose during the course of the procedure, resulting in rapid but non-sustainable rises. Time between events and detection: range 8 – 20 min (mode value 9 min). Temporal lobe retraction (n=7): lactate +71 %, glucose −25%. Glucose bolus infusion (n=4): +587% (peak at 16 min). Temporary proximal clip (n=6): mean clip time: 8.1 min; lactate + 72%; glucose change −24%. Periods of low glucose: 7 under 150 microM, 3 undetectable. In 6 patients outcome quality correlated inversely with duration of glycopaenia (dialysate glucose <150 microM, Spearman's Ranked: r2=0.94, p < 0.05).
Conclusions
The method robustly detects changes after 9 minutes (limited by surgical site-to-sensor transit), and thereby the ischaemic events associated with temporary clipping and lobe retraction. This enables the possibility of real-time feed-back and prompt changes in management (surgical or anaesthetic). The adverse effect of intraoperative glucose depletion on outcome after aneurysm surgery resembles findings in head injury 4 .