
Introduction
In animal studies waves of peri-infarct depolarisations (PIDs) propagate from the penumbra region around focal brain lesions into intact brain regions, where they show the characteristics of cortical spreading depression (CSD) 1 . Recurrent PIDs are associated with increases in final infarct volume 2 . Clinical neuroprotection studies using NMDA-receptor antagonists that block CSD and PID have been disappointing. To select patients that may benefit from this treatment, it seems important to detect CSDs and PIDs reliably in man. We reported transient depressions of electrocorticographic activity (ECoG) spreading with a speed similar to experimental CSD, in 5/14 brain injured patients 3 . We have now improved the technique to enable detection of cortical depolarisations: The COSBID study (www.cosbid.org).
Methods
ECoG was recorded for up to 120 hours from twelve acutely brain-injured human patients by six platinum electrodes placed near foci of damaged cortical tissue. The ECoG was high pass filtered at 0.02 Hz to enable recording of slow potential changes (SPC) of 2–3 minute duration to prove that ECoG depressions were identical to CSD, and to be able to record PIDs in otherwise electrically silent cortical tissue.
Results
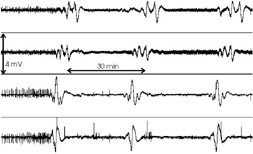
Six patients displayed a total of 49 spontaneous episodes of spreading depression of the ECoG. ECoG depressions were invariably accompanied by stereotyped SPCs (Figure 1), and spread across the cortex at 3,3 (1,0-10) mm/min (median (range)). The amplitude of the SPCs was 0,1-4,0 mV. In 5/6 patients the ECoG recovered spontaneously. In one patient we recorded recurrent SPCs, but without recovery of the initial ECoG activity (Figure 1). This may represent the first direct recording of PIDs in acute human brain injury. CSD was recorded in 4/5 patients with traumatic brain injury, and in 2/7 patients with spontaneous cerebral haemorrhages or SAH.
Conclusion
The spreading ECoG depressions recorded in patients are identical to CSDs recorded in animal experiments. We furthermore provide direct electrophysiological evidence for the existence of PIDs and hence a penumbra in the human brain. We hypothesise that CSDs and PIDs might contribute to the tissue damage in acute brain disorders.