
Introduction
Magnetic resonance contrast agents (MRCA) can be intravenously (i. v.) administered by either bolus injection or continuous infusion. Two previous studies have employed these two input functions for comparison of resultant data, but came to different conclusions1, 2. In this study, a rat model of transient cerebral ischemia was used and the differences in MRCA arterial inputs, contrast enhancement, estimates of gadolinium-diethylenetriaminepentaacetic acid (Gd-DTPA) influx constants (Ki) and Gd-DTPA affected-proton distribution volumes (Vp) between the two methods were evaluated.
Methods
Unilateral cerebral ischemia was induced in halothane anesthetized male Wistar rats (275–295 g; n=12) by suture occlusion of the right middle cerebral artery. After 3 hr of occlusion, the suture was withdrawn to initiate reperfusion. At ∼2.5 hr post-reperfusion, Gd-DTPA-based contrast enhanced MR imaging was performed to localize extravascular enhancement and quantify Ki and Vp. For bolus injection, 0.02 mmol Gd-DTPA was injected through a femoral vein. For continuous infusion, a stepped-down procedure using a syringe pump was employed following published procedures 3 to quickly attain and maintain an elevated blood level of Gd-DTPA. Resultant arterial input functions from both were tracked with MRI using a T1-Look-Locker sequence by measuring changes in Gd-DTPA relaxation rates (ÄR1; R1=1/T1) in sagittal sinus as described previously 3 . Offline image processing was performed to localize enhancing areas and calculate Ki and Vp using Patlak plots 3 .
Results
The bolus injection produced a steep rise in Gd-DTPA levels in the sagittal sinus that decayed exponentially; the continuous infusion a steep rise that remained steady for the duration of the study (Figure 1). The continuous infusion schedule resulted in better visual enhancement and definition of the infarct than bolus injection (blinded observations), confirming a previous report 2 . For bolus injection and for continuous infusion, the values (mean ± SD) were 0.004 ± 0.001 and 0.006 ± 0.005 ml/g/min (Ki) and 0.06 ± 0.02 and 0.075 ± 0.04 ml/g (Vp), respectively (p>0.05).
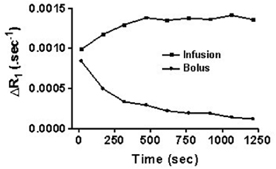
Representative sagittal sinus Gd-DTPA concentration over time after a bolus and constant infusion arterial input functions. Note the steep fall in levels in the farmer and the near steady state levels in the latter.
Conclusion
Bolus injections may not result in complete resolution of the infarct because: 1) rapid diffusion into the tissue of smaller contrast agents such as Gd-DTPA may not define the infarct boundaries; and 2) backflux of the MRCA can underestimate blood-to-brain transfer kinetics. A continuous infusion schedule may help overcome these deficits by maintaining a steady blood level and a unidirectional driving force from vasculature to tissue. Therefore, despite its perceived shortcomings 1 , a continuous infusion schedule may be applicable in identification of ischemic infarct and evaluating therapeutic effects 2 . These data also confirm the usefulness of MR imaging of the sagittal sinus to non-invasively track arterial input functions.
Footnotes
Acknowledgements
Grant support: Supported by RO1NS38540 and American Heart Association-Bugher oundation Award (0270176N)