Objectives
Emboli generation during cardiac surgery is known to contribute to postoperative neurocognitive outcome. Cardiopulmonary bypass (CPB) seems to be a major cause for both intraoperative microemboli generation and cerebral hypoperfusion. In opposition to cardiopulmonary bypass off-pump coronary artery bypass grafting (OPCAB) reduces microemboli generation. On the other hand OPCAB carries the risk for hemodynamic instability due to manipulation on the beating heart. Hemodynamic impairment during surgical revascularisation causes postoperative morbidity and mortality. Therefore an intracardiac left ventricular microaxial bloodpump was used to augment cardiac output during beating heart myocardial revascularisation in this adult porcine model. The effect of these three different operative techniques on emboli generation, cerebral perfusion and water content was studied.
Methods
In 27 swines a bypass from the internal mammarian artery to left anterior descending coronary artery was constructed using CPB with cardioplegic arrest (n=9), OPCAB surgery (n=9) or Impella microaxial bloodpump supported OPCAB (n=9). 9 animals received a sham operation. Emboli count in the right common carotid artery was monitored. Regional cerebral perfusion (RCP) was assessed in 21 biopsies from the Cortex cerebri, Mesencephalon, Hippocampus, Thalamus, Hypothalamus, Medulla oblongata, Pons and Cerebellum with 15μm fluorescent microspheres. Mean arterial pressure (MAP), cardiac output (CO), left ventricular dp/dt (LV dp/dt), LV ejection fraction (LVEF) and arterial blood gases were recorded. These variables were analysed 30 minutes before, several times during the procedure and four hours postoperatively. Four hours after surgery the brain was removed and the water content in a part of the frontal lobe was determined.
Results
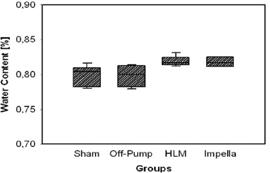
During CPB and Impella assistance a significant amount of embolies were registrated. A minimal amout of cerebral embolies was counted during OPCAB surgery and in control animals. During CPB regional cerebral perfusion was unaffected, but afterwards RCP showed reactive hyperemia during early reperfusion in all observed areas. During and after OPCAB RCP remained unchanged and showed low flow during and after Impella pump-run (p<0.05). Cerebral water content was significantly increased after CPB and Impella assistance. There was no difference in cerebral water content between control and OPCAB animals. MAP significantly decreased during revascularisation in all groups staying below preoperative values thereafter (p<0.05). After CPB norepinephrine was administered to maintain MAP. CO, LVdp/dt and LVEF were impaired more distinct during OPCAB than Impella (p<0.05) with subsequent recovery. Arterial bloodgases remained stable throughout all experiments.
Conclusions
Highflow normothermic CPB with cardioplegic arrest led to emboli generation with consecutive cerebral reactive hyperemia although cardiac output, mean arterial pressure and arterial bloodgases stayed in uncritical ranges resulting in a signifcant increase in cerebral water content. OPCAB surgery did not generate significant cerebral emboli load. However hemodynamic depression without adverse effects on RCP was observed. Hemodynamic depression can be reduced by the Impella bloodpump. On the other hand regional cerebral blood flow is decreased by massive emboli formations resulting in the most pronounced increase in cerebral water content (See Figure 1).