
Introduction
Human and animal studies indicate that hyperglycaemia worsens outcome in acute ischemic stroke, especially after reperfusion or thrombolysis. No treatment has been shown to overcome its detrimental effects. The mechanism by which hyperglycaemia worsens stroke outcome is not established. Prior work indicated that reperfusion vascular injury rapidly impairs eNOS resulting in a contractile phenotype, impairing reperfusion blood flow and worsening the ischemic deficit. Intriguingly, therapeutic ultrasound can rapidly increase perfusion of ischemic tissue, possibly via phosphorylation of eNOS. The CLOTBUST trial (Alexandrov et al NEJM 2004; 351(21): 2170–8) demonstrated enhanced lytic activity of tPA when augmented with diagnostic pulsed wave Doppler ultrasound. We hypothesised that hyperglycaemic stroke subjects might benefit from ultrasound therapy and that this effect would not be solely due to enhanced recanalisation.
Methods
126 acute MCA ischemic stroke subjects treated within 3 hours with tPA were randomised to either sham or active continuous ultrasound therapy of the MCA. Primary outcome was 90 day modified Rankin Scale score of 0–2. We sought an interaction between glucose and active ultrasound treatment in a simple logistic regression model, subsequently searching for potential confounding variables using backwards elimination. Age and baseline NIHSS were included in the final model. The interaction term was tested using a likelihood ratio test.
Results
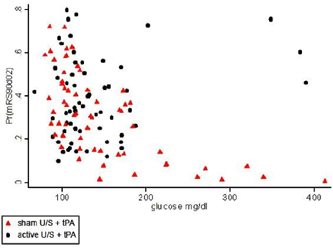
32% of controls and 33% of active ultrasound subjects had baseline serum glucose levels >140 mg/dL. High glucose levels predicted a lower probability of functional independence in the control but not the active ultrasound group, as demonstrated by a statistically significant interaction between glucose and treatment group (p=0.043). This beneficial effect of ultrasound on outcome was particularly prominent at high glucose levels (Figure 1). Of subjects with admission glucose >200 mg/dl, none of the controls recanalised at 2 hours, compared to 24% in the active ultrasound group (NS, p=0.417). None of these controls were functionally independent at 90 days, compared to 75% of the active ultrasound subjects (p=0.024), even though no early recanalisation was demonstrated in half of the active ultrasound subjects.
Discussion
Ultrasound exposure overcame the negative effect of hyperglycaemia on outcome. This is the first therapy that has improved functional outcome in hyperglycaemic stroke subjects. Additional analyses supported our hypothesis that the mechanism of benefit is not due to enhanced or earlier recanalisation, suggesting that ultrasound may act through other mechanisms, including beneficial vasodilatory actions within the vessel wall and downstream. Future planned studies will test this hypothesis prospectively.