Intensive Insulin Therapy is Associated with Reduced Extracellular Glucose and Increased Oxygen Extraction Fraction after Severe Traumatic Brain Injury
Introduction
Reductions in extracellular glucose after traumatic brain injury (TBI) is associated with poor outcome and may be related to substrate limitation. Intensive insulin therapy is a commonly used treatment in intensive care and is considered to be crucial in limiting brain damage and brain lactic acidosis after a TBI.
Hypothesis
Intensive Insulin therapy (IIT) to maintain normoglycemia may provoke reductions in available brain glucose and precipitate changes in oxidative metabolism.
Methods
Nineteen patients with severe TBI underwent cerebral microdialysis (1 uL/min) in normal appearing brain tissue before and during insulin infusion aimed at maintaining glucose levels in normal range (5–7 mM). Serial hourly changes in extracellular glucose, lactate and pyruvate were tracked. Single session oxidative positron emission tomography (PET) was obtained in each subject during spontaneous uncontrolled states of glycemia. Regional and whole brain quantitative rates of oxygen extraction fraction (OEF) were determined and compared with serum glucose and extracellular glucose values.
Results
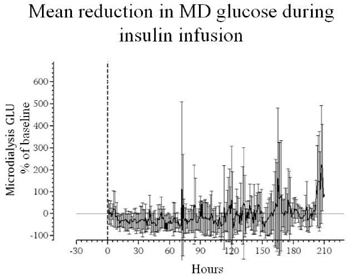
During IIT, extracellular glucose decreased by 70% ± 11of hyperglycemic baseline in 2/3 of patients (responders). In responders, the extracellular glucose decreased to low levels (<0.2 mmol/l) in 31% of samples with a corresponding increase in the lactate/pyruvate ratio >40 in 61% of samples. In nonresponders, the total duration of elevated lactate/pyruvate was nonsignificantly less than that of the responders (p < 0.06). Regional PET OEF correlated poorly with extracellular glucose (−0.03) but whole brain OEF negatively correlated with serum glucose (−0.61, r = 0.01). Serum glucose values of 5–5.5 mM (the goal of IIT) were associated with the highest PET OEF, ranging from 0.5–0.8. These effects were independent of severity of injury.
Conclusion
During IIT, the brain exhibits signs of metabolic distress with decreases in extracellular glucose, elevation of lactate/pyruvate ratio and increases in OEF (See Figure 1).