
Abstract
Knowledge about the longitudinal change of cerebral small-vessel disease–related magnetic resonance imaging abnormalities increases our pathophysiologic understanding of cerebral microangiopathy. The change of specific lesion types may also serve as secondary surrogate endpoint in clinical trials. A surrogate endpoint needs to progress fast enough to allow monitoring of treatment effects within a reasonable time period, and change of the brain abnormality needs to be correlated with clinical change. Confluent white matter lesions show fast progression and correlations with cognitive decline. Thus, the change of confluent white matter lesions may be used as a surrogate marker in proof-of-concept trials with small patient numbers needed to show treatment effects on lesion progression. Nonetheless if the expected change in cognitive performance resulting from treatment effects on lesion progression is used as outcome, the sample size needed to show small to moderate treatment effects becomes very large. Lacunes may also fulfill the prerequisites of a surrogate marker, but in the general population the incidence of lacunes over short observational periods is small. For other small-vessel disease–related brain abnormalities including microbleeds and microstructural changes in normal-appearing white matter longitudinal change and correlations with clinical decline is not yet fully determined.
Introduction
Cerebral small vessel disease is the second most common endemic entity of the aging brain following Alzheimer pathology. White matter lesions (WML), lacunar infarctions and cerebral microbleeds are the hallmark lesions of cerebral small vessel disease.
1
They can be non-invasively depicted by brain magnetic resonance imaging. Figure 1 displays the spectrum of small vessel disease-related brain abnormalities.
The spectrum of small-vessel disease–related brain changes in magnetic resonance imaging (MRI). White matter lesions ranging from punctuate foci to extensive confluent abnormalities (a, b, and c), cerebral microbleeds (d), and lacunar infarcts (e and f).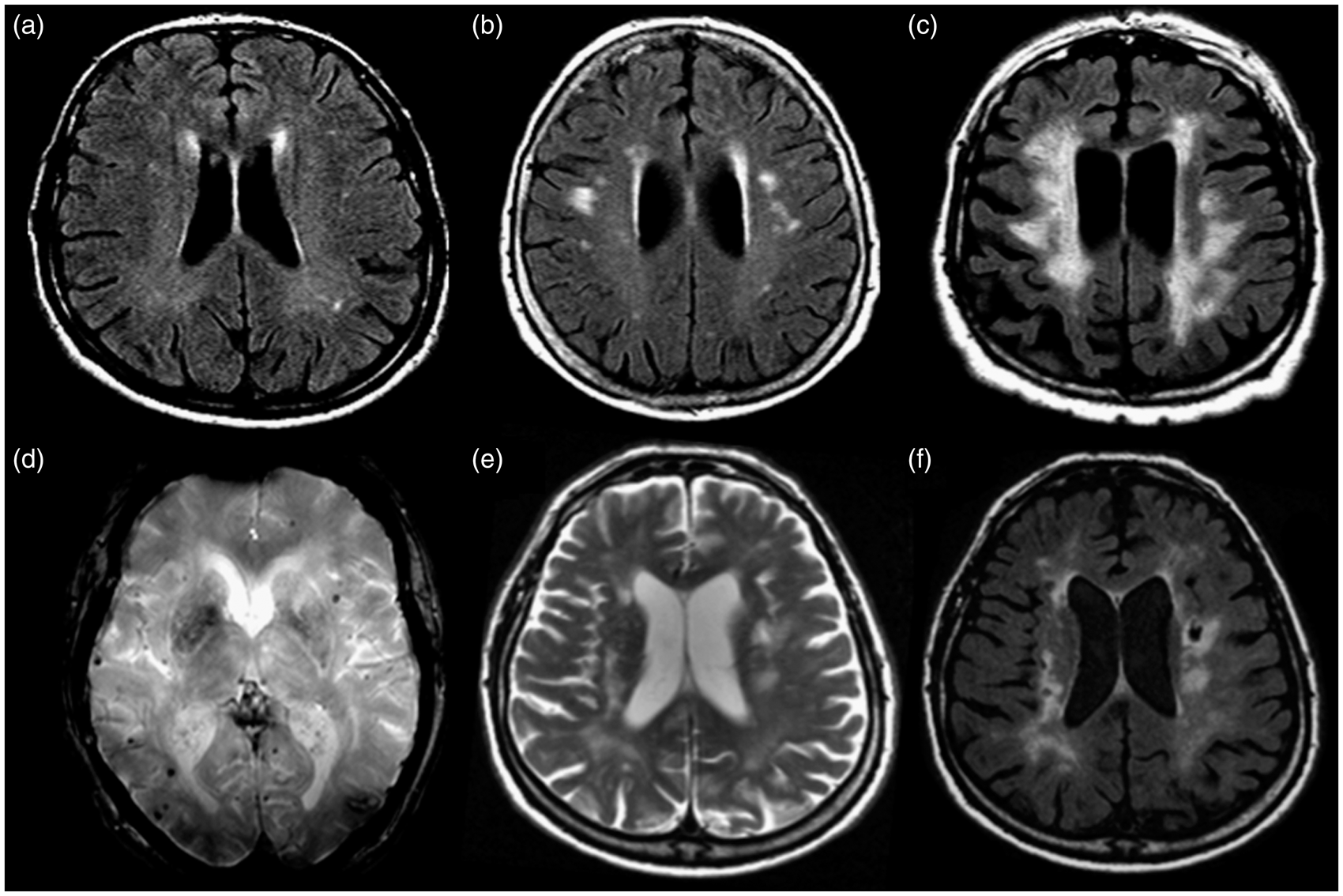
Up to 90% of patients above the age of 65 years present WMLs of varying severity when undergoing MRI. 2 Lacunes occur less commonly with a frequency ranging from 6% to 20%, 3 and microbleeds affect 5% to 15% of the general elderly population. Decreased mobility caused by disequilibrium and gait abnormalities, and progressive cognitive impairment up to dementia are frequent clinical sequelae of cerebral microangiopathy. 1 An often neglected dysexecutive syndrome with slowing of mental processing, inhibition, and only mild memory impairment are the core cognitive dysfunctions. Because of the slow progressive course of these clinical correlates, symptoms remain often unnoticed in clinical evaluations. Nonetheless, they represent important causes of physical disability of older persons and thus are thought to have an enormous socioeconomic impact. 4 Recent advances in imaging techniques have highlighted the importance of normal-appearing brain tissue in the context of age-related white matter abnormalities. In fact, these studies show that there is more widespread tissue damage associated with WMLs and possibly also other small-vessel disease–related lesion types that is not visible in conventional MR images. Such microstructural tissue abnormalities can be detected by new quantitative MR techniques, such as diffusion tensor imaging (DTI) and magnetization transfer imaging (MTI).5,6 Microstructural changes in normal brain tissue have been shown to be more closely related to the patients’ clinical presentation than the volume of visible white matter abnormalities.
Although the majority of data on the clinical effects of small-vessel disease–related brain abnormalities still come from cross-sectional studies, numerous longitudinal MRI studies have meanwhile been conducted and increase our understanding of the natural history of cerebral small–vessel disease in general, and of differences in the evolution of related lesion types, in particular. Most importantly, there exists, not yet any, established treatment, which was proven to modify the evolution of small-vessel disease–related brain damage. Progression of small-vessel disease–related brain lesions has been suggested to facilitate treatment development by serving as secondary surrogate endpoints in clinical trials on subcortical vascular cognitive impairment. There are several prerequisites that need to be fulfilled for any MRI abnormality to be considered as a potential surrogate endpoint. 7 These include (1) a reasonable confidence that the observed tissue changes are indeed related to cerebral microangiopathy; (2) evidence for a rate of progression, which is fast enough to allow monitoring of treatment effects within a reasonable period of time; and (3) a correlation between the change of the imaging marker with changes in clinical outcomes. In this review, we report the progression rate and clinical consequences of the different types of small-vessel disease–related brain abnormalities and provide sample size calculations for trial planning for each abnormality.
White matter lesions
Progression of WMLs in different longitudinal MRI studies.
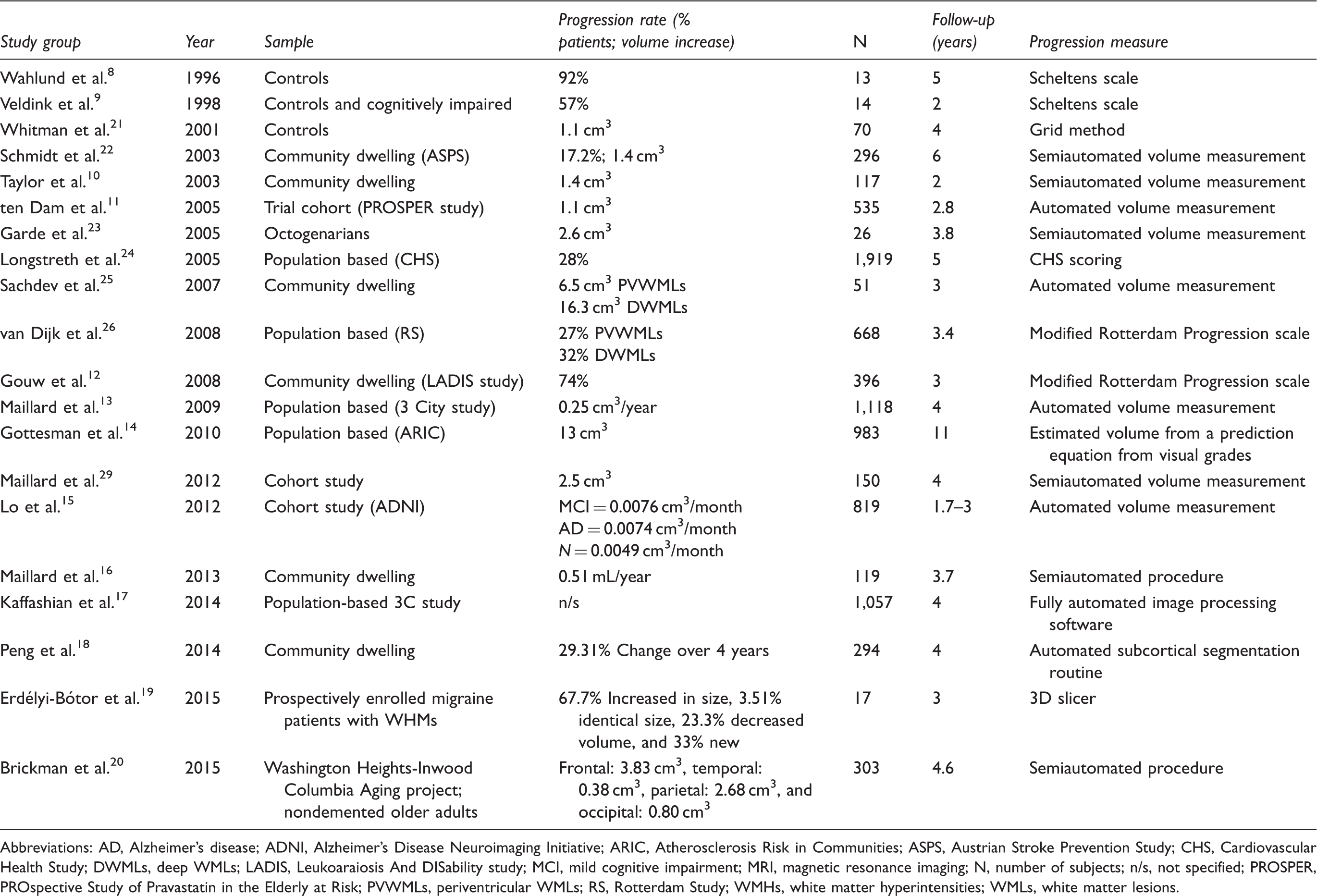
Abbreviations: AD, Alzheimer's disease; ADNI, Alzheimer’s Disease Neuroimaging Initiative; ARIC, Atherosclerosis Risk in Communities; ASPS, Austrian Stroke Prevention Study; CHS, Cardiovascular Health Study; DWMLs, deep WMLs; LADIS, Leukoaraiosis And DISability study; MCI, mild cognitive impairment; MRI, magnetic resonance imaging; N, number of subjects; n/s, not specified; PROSPER, PROspective Study of Pravastatin in the Elderly at Risk; PVWMLs, periventricular WMLs; RS, Rotterdam Study; WMHs, white matter hyperintensities; WMLs, white matter lesions.
A faster rate of progression was observed in people with arterial hypertension (0.14 to 0.54 cm3/year) 27 and in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukencephalopathy patients (3.96 cm3/year). 28
The annual increase in WML volume in percentage ranges between 12.5% and 14.4% in subjects with early confluent lesions and between 17.3% and 25.0% in those with confluent abnormalities. 22
There is evidence that WMLs do not progress randomly. One recent study on 150 cognitively normal and demented people found that up to 80% of incident WMLs occurring over an observational period of 4 years represented extensions of preexisting lesions. 29 In 365 patients with CADASIL and in 588 healthy elderly subjects from the Austrian Stroke Prevention Study, WMLs expanded from the periventricular white matter, where they were most prevalent, preferentially toward the subcortical white matter. They grew favorably along the trajectories of small perforating arteries, suggesting the vascular end zone as a predilection site for WMLs. 30
Several studies reported that baseline WML grade is the strongest predictor of future progression of such changes,22,25,26,31 followed by arterial hypertension.9,26,32– 34
Notably in the study by Verhaaren et al., 33 people with uncontrolled untreated hypertension had significantly more WML progression than people with uncontrolled, but treated hypertension. 33 Similar results come from the Three-City (3C)-Dijon Magnetic Resonance Imaging study. In a sample of 1,319 elderly individuals, antihypertensive treatment was related to a smaller increase in WML volume over a 4-year follow-up period. 34
If blood pressure treatment influences WML progression sufficiently to slow down cognitive decline, has to be determined. Other, commonly reported risk factors for WML progression are higher age, 26 previous stroke and diabetes, 12 hyperhomocysteinemia, 35 and the presence of the apolipoprotein E e4 allele. 36
Genetic association studies in the setting of the Austrian Stroke Prevention Study described that polymorphisms in the renin–angiotensin system 31 increased the susceptibility for progression of cerebral small–vessel disease 3.19-fold, independent of arterial hypertension. Also genetic variants of the paraoxonase gene, a gene important for antioxidative defense mechanisms, 37 relate to WML progression. Recently, four single nucleotide polymorphisms within the neurogenic locus notch homolog protein 3 gene, that is responsible for CADASIL, were found to be associated with both the presence and progression of WMLs. 38
Progression of WMLs and correlation with clinical outcome.
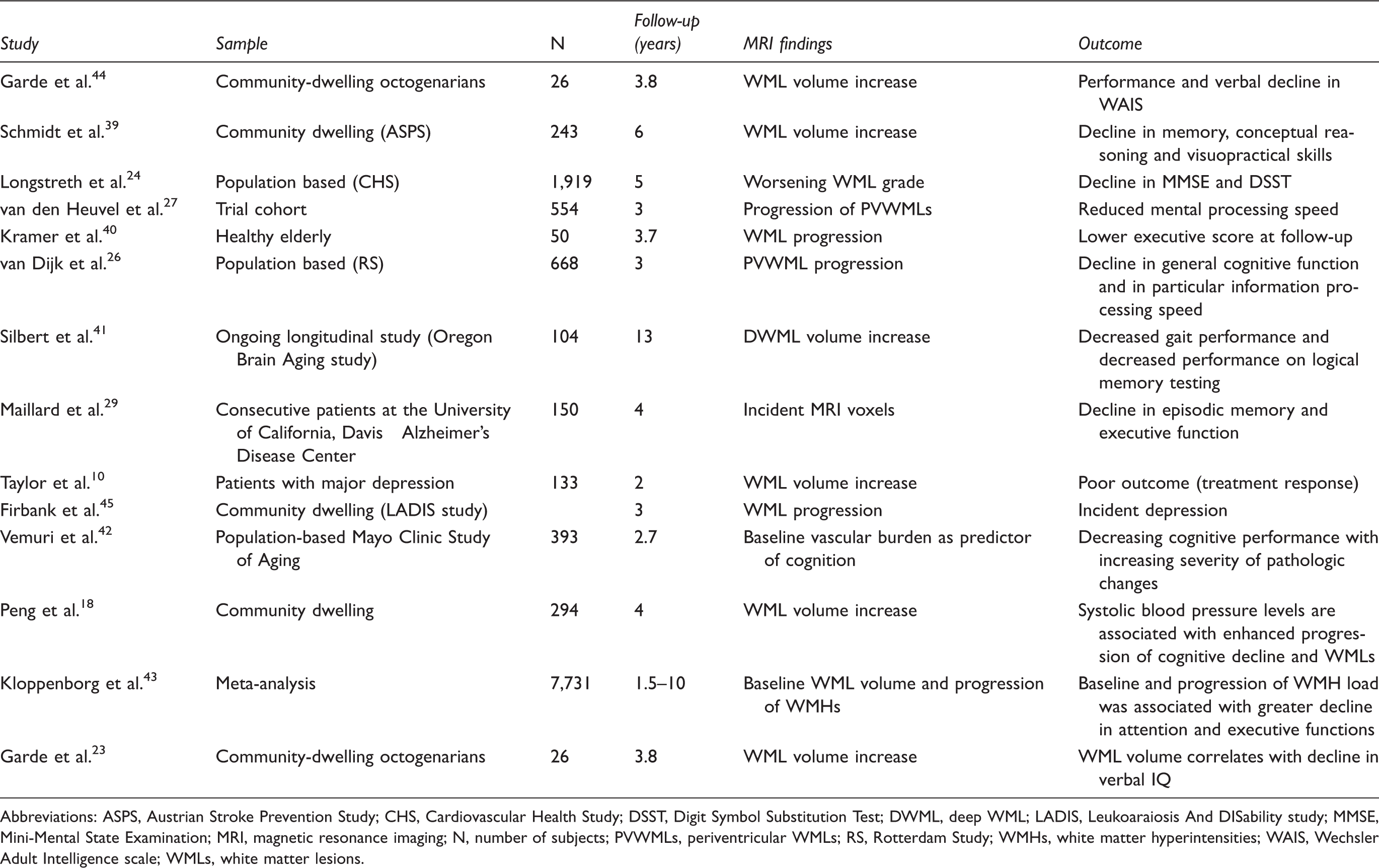
Abbreviations: ASPS, Austrian Stroke Prevention Study; CHS, Cardiovascular Health Study; DSST, Digit Symbol Substitution Test; DWML, deep WML; LADIS, Leukoaraiosis And DISability study; MMSE, Mini-Mental State Examination; MRI, magnetic resonance imaging; N, number of subjects; PVWMLs, periventricular WMLs; RS, Rotterdam Study; WMHs, white matter hyperintensities; WAIS, Wechsler Adult Intelligence scale; WMLs, white matter lesions.
In the Cardiovascular Health Study, increase in WML grades was related to global cognitive decline. 24 In the Rotterdam Study, progression of periventricular WMLs was associated with decline in general cognitive performance and information processing speed. 26
In the Austrian Stroke Prevention Study, we observed a complex interaction between increasing volume of WMLs, brain atrophy and cognition. Brain volume change mediated the association between WML progression and cognitive decline. This was seen for domains of memory, executive function, and visuopractical skills. 39 Greater WML load at baseline predicts conversion from normal aging to mild cognitive impairment 46 and conversion from amnestic mild cognitive impairment to Alzheimer's disease. 47 This highlights the clinical importance of WMLs. In the Leukoaraiosis And DISability (LADIS) study, baseline WML load also predicted global functional decline and disability over a relatively short observational period of 2.42 years. 48
In the Austrian Stroke Prevention Study, we estimated that ∼200 individuals with confluent lesions would be necessary per treatment arm to show a 20% reduction in disease progression over a 3-year time period. 7 Thus, WML progression became an interesting outcome measure for proof-of-concept studies in cerebral small–vessel disease.
Owing to the fact that volumetric measurements of WML change are laborious and time consuming, a visual rating scale to assess progression might be better suited in clinical trials.
A recent publication from the LADIS study evaluated the association between WML progression determined on the visual Rotterdam Progression scale 49 and cognitive functioning, and provided sample size calculations for clinical trials using the Rotterdam Progression scale rated WML progression as surrogate endpoints. 50
Progression was seen in 73.6% of the study participants. In line with previous studies, 51 WML grade at baseline was the strongest predictor of future WML progression.
Sample size estimates per treatment arm according to WML grade at baseline in a 3-year trial in which treatment reduces WML progression by one gradea.
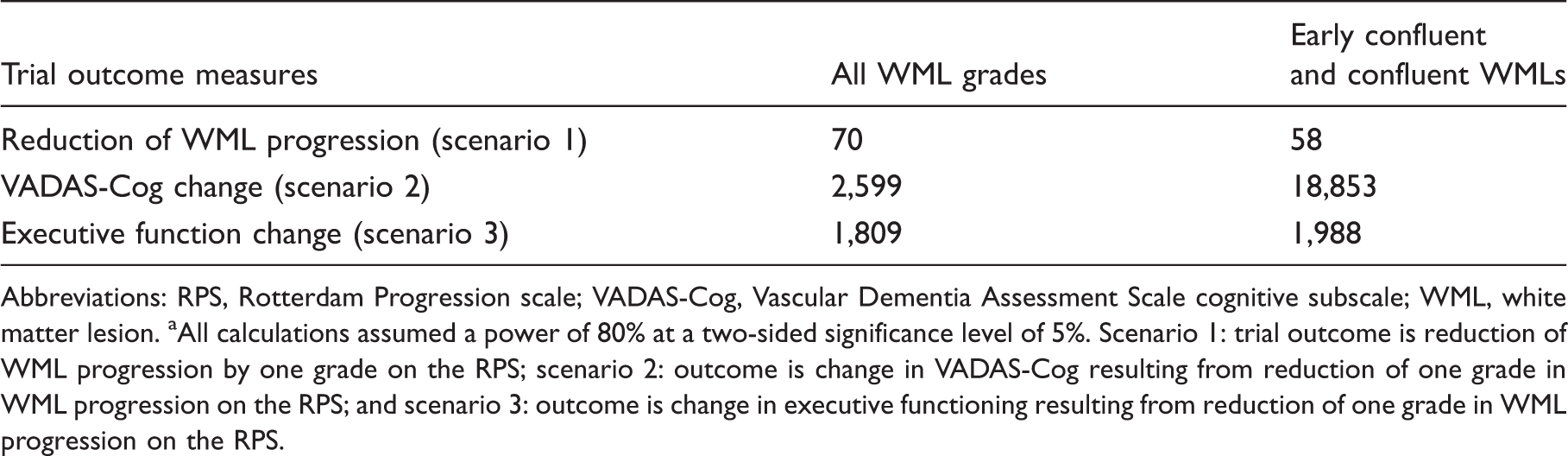
Abbreviations: RPS, Rotterdam Progression scale; VADAS-Cog, Vascular Dementia Assessment Scale cognitive subscale; WML, white matter lesion.
All calculations assumed a power of 80% at a two-sided significance level of 5%. Scenario 1: trial outcome is reduction of WML progression by one grade on the RPS; scenario 2: outcome is change in VADAS-Cog resulting from reduction of one grade in WML progression on the RPS; and scenario 3: outcome is change in executive functioning resulting from reduction of one grade in WML progression on the RPS.
As can be seen from Table 3, low subject numbers are required per treatment arm in scenario 1 trials in which WML progression is the primary outcome measure. Such settings will allow lowering sample sizes when including only individuals with early confluent or confluent lesions. For scenarios 2 and 3, in which the expected change in cognitive performance resulting from treatment effects on WML progression was the outcome, 2,599 or 18,853 subjects per treatment arm would be necessary for Vascular Dementia Assessment Scale cognitive subscale and 1,809 or 1,988 for the executive function test. These data underline that sample size strongly depends on both baseline WML grade and applied cognitive tests. 50
The tremendously large sample sizes in a trial in patients with early confluent or confluent WMLs using Vascular Dementia Assessment Scale cognitive subscale as the clinical outcome was probably caused by a pronounced cognitive deterioration in individuals with early confluent and confluent WMLs irrespective of future lesion progression.
Lacunes
Frequency of incident lacunes in different MRI studies.
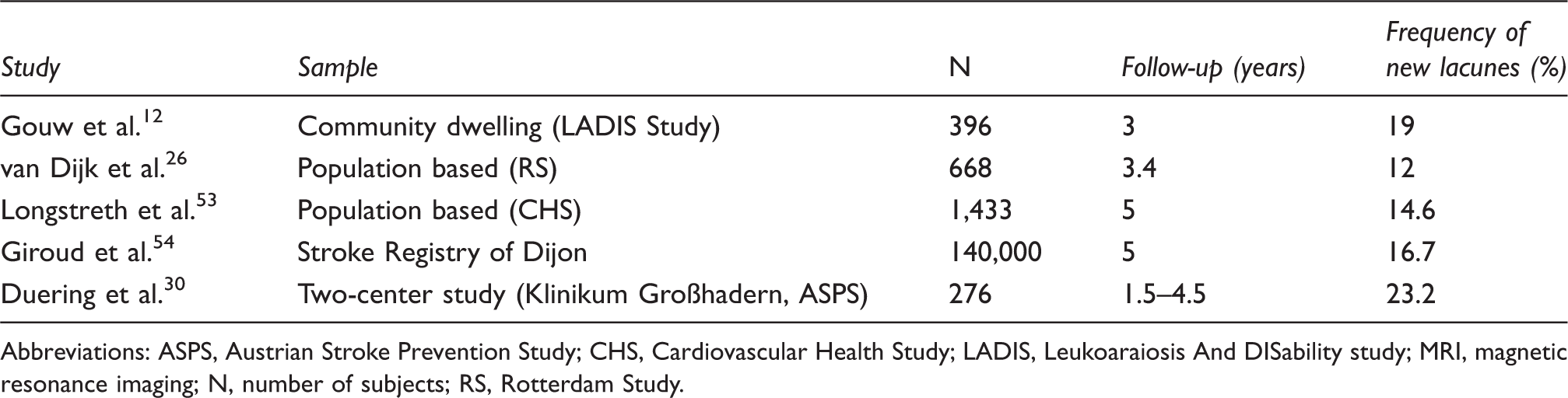
Abbreviations: ASPS, Austrian Stroke Prevention Study; CHS, Cardiovascular Health Study; LADIS, Leukoaraiosis And DISability study; MRI, magnetic resonance imaging; N, number of subjects; RS, Rotterdam Study.
New evidence on the pathophysiology of lacunes was reported by Duering et al.
30
In 365 CADASIL patients, 91.3% of incident lacunes appeared in brain regions showing contact or partial overlap with preexisting WMLs. Only 5.8% developed fully inside a preexisting WMLs and only 2.9% developed in the normal-appearing white matter at baseline. Figure 2 shows a schematic of incidence of lacunes with regard to their vicinity to WMLs, proposed by Duering et al.
30
Thus, tissue adjacent to WMLs might be especially susceptible to further ischemia including formation of lacunes. Such subtle changes in the white matter surrounding WMLs are detectable on DTI and have been described and termed ‘white matter hyperintentity penumbra’ by Maillard et al.
56
Incident lacunes and their location regarding preexisting white matter lesions (WMLs) according to Duering et al.
30
Based on the rating, lacunes are classified as (a) grade 0: no contact with WMLs (2.9%), (b) grade Ia: contact with WMLs but no overlap (45.2%), (c) grade Ib: partial overlap (46.1%), and (d) grade II: complete overlap (5.8%).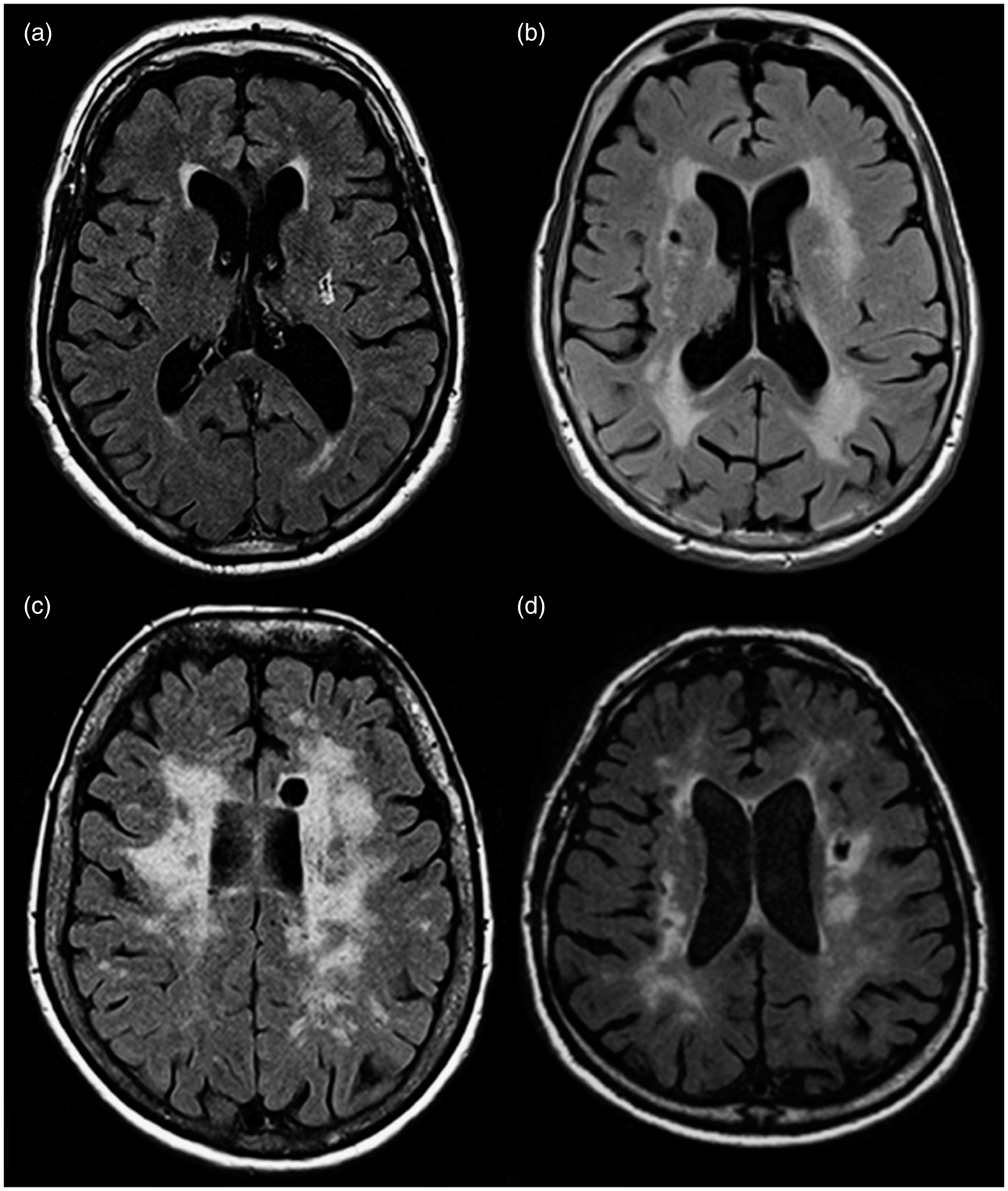
Incident lacunes and correlation with clinical outcome in longitudinal studies.
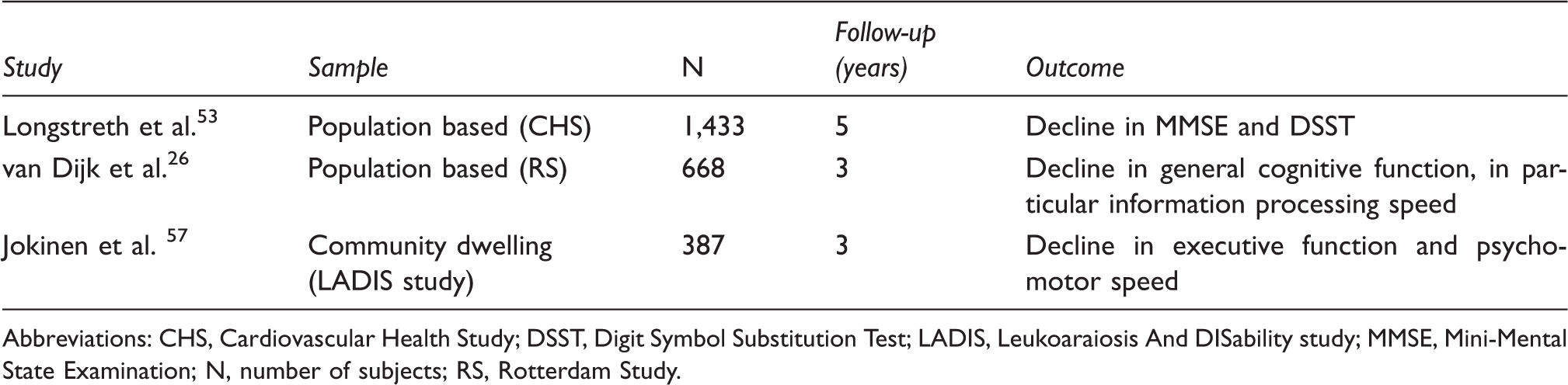
Abbreviations: CHS, Cardiovascular Health Study; DSST, Digit Symbol Substitution Test; LADIS, Leukoaraiosis And DISability study; MMSE, Mini-Mental State Examination; N, number of subjects; RS, Rotterdam Study.
Studies consistently show that incident lacunes exert detrimental functional effects. The Cardiovascular Health Study reports that the incidence of lacunes was related to decline in the Mini-Mental State Examination and the Digit Symbol Substitution Test. 53 Similar associations were found in the Rotterdam Scan Study where incident lacunes were related to a decline in general cognitive function and information processing speed. 26 In the LADIS study, a relationship between incident lacunes at 3-year follow-up and steeper decline in executive functions and psychomotor speed was reported. 57
According to the previously published data on the rate of incident lacunes,12,26,30,53,54 detection of a 20% treatment effect in a 3-year trial with 80% power would require samples sizes in the range between 1,540 and 3,678 patients.
Microbleeds
The Rotterdam Scan Study showed that the incidence of cerebral microbleeds strongly depends on age. 58 The rate of lesions was reported to be 7.6% in subjects aged 60 to 69 years, it increased to 15.6% in the age range between 70 and 79 years, and 18.6% in subjects older 80 years. Subjects with microbleeds at baseline showed more than five times higher risk for newly occurring microbleeds as compared with their counterparts without such baseline abnormalities. 59
In a smaller longitudinal study, which reassessed patients with stroke or transient ischemic attack after >12 months, 53.9% of the patients with cerebral microbleeds at baseline showed new microbleeds at follow-up. 60
So far, little information exists on the clinical consequences of incident cerebral microbleeds. There are only a few longitudinal studies available. 61 – 64 Although Gregoire et al. 64 report on the predictive value of baseline microbleeds considering executive functions over 5.7 years, Meier et al. 62 report on decreasing executive functions if at least two microbleeds are present. Liem et al. 61 identified increasing cognitive decline with increasing number of incident microbleeds in CADASIL patients over 7 years of follow-up. Moreover, patients with warfarin therapy and baseline microbleeds had an increased risk for additional microbleeds. 63 Because of the lack of clinical correlative data the validation status of these lesions as a possible surrogate marker in vascular cognitive impairment trials has to be considered incomplete and sample size calculations are thus not provided.
Microstructural changes in normal-appearing brain tissue
Recent advances in imaging techniques have highlighted the importance of normal-appearing brain tissue in the context of WMLs. There is more widespread tissue damage associated with WMLs, which is not visible in conventional MRI but can be detected by DTI and MTI.5,6 Diffusion tensor imaging provides information about the microstructural integrity of brain tissue by measuring the direction and magnitude of water diffusion in the intracellular compartment of the axons. Because of the restriction by lipid bilayers and other cell components, water diffusion in brain tissue is anisotropic with the highest diffusivity along the directions of the axons. MTI is an approach to explore the composition of brain tissue. Protons bound to macromolecules such as the myelin lipids and proteins have relaxation properties that make them invisible for conventional MRI. However, the pool of bound protons can be imaged indirectly by exploiting magnetization transfer. Animal models and postmortem studies indicate that quantitative DTI and MTI measures correlate with markers of myelin integrity, and axonal damage and density. 65 – 68 A study in brain hypoperfused mice examined the complementary value of DTI and MTI measures for delineation of white matter damage. 68 After continuous moderate hypoperfusion over 1 month the authors found that the reduction in fractional anisotropy paralleled a decrease in magnetization transfer ratio in several tissue compartments. They concluded that both techniques are adequately suited to detect microstructural tissue alterations at least in the white matter of the murine brain. Postmortem histopathologic analyses assessing myelin content, axonal density, and gliosis revealed similar correlations in the brains of patients with Alzheimer’s disease 65 and multiple sclerosis. 69
There is evidence that normal-appearing white matter magnetization transfer ratio decreases with increasing WML burden and magnetization transfer ratio within WMLs is on average ∼10% lower than that of normal-appearing white matter, indicating microstructural tissue damage within and outside WMLs.70,71 Similar observations have been made using DTI. Important in this context, the prognostic value of baseline local DTI parameters for WML progression within a 4-year period has been reported. 72
Longitudinal microstructural changes.
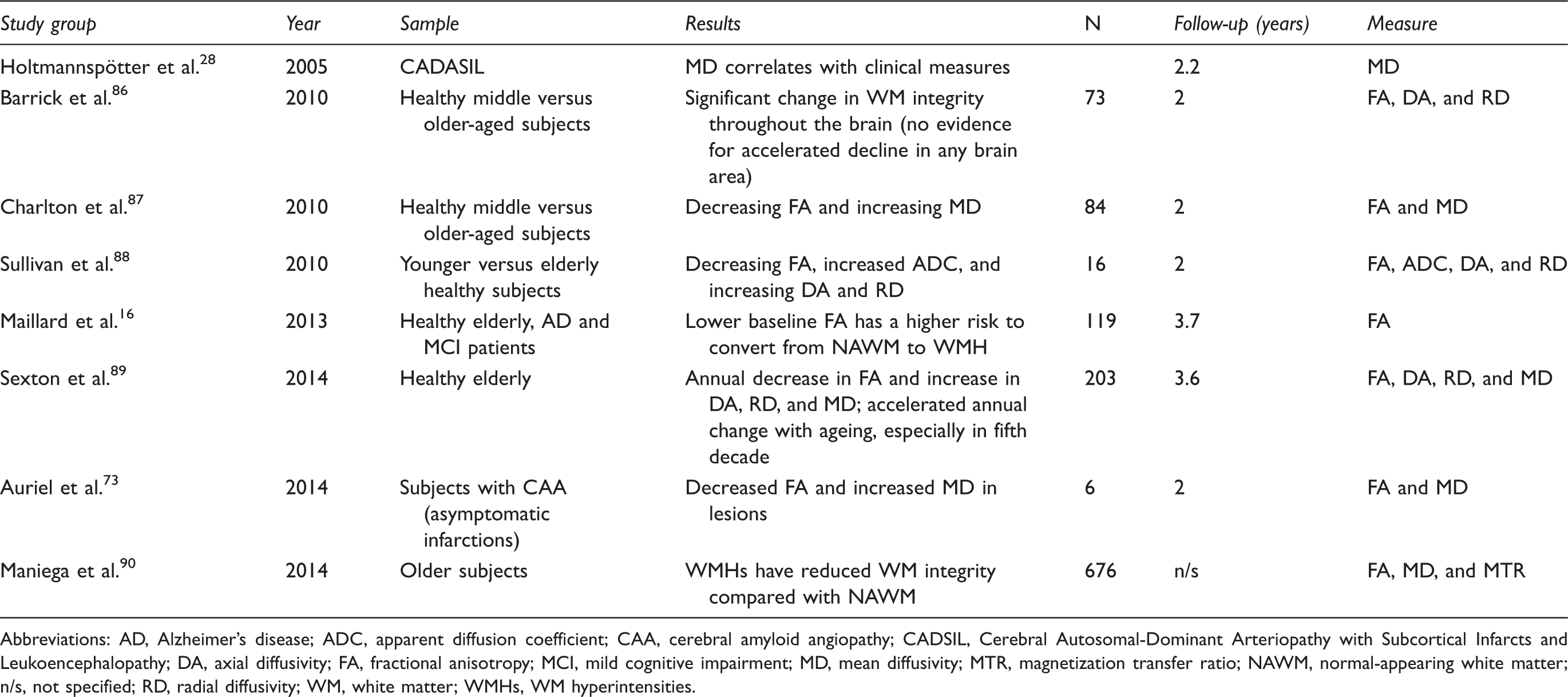
Abbreviations: AD, Alzheimer's disease; ADC, apparent diffusion coefficient; CAA, cerebral amyloid angiopathy; CADSIL, Cerebral Autosomal-Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy; DA, axial diffusivity; FA, fractional anisotropy; MCI, mild cognitive impairment; MD, mean diffusivity; MTR, magnetization transfer ratio; NAWM, normal-appearing white matter; n/s, not specified; RD, radial diffusivity; WM, white matter; WMHs, WM hyperintensities.
A multimodal study evaluating MRI parameters as surrogate markers of cerebral small–vessel disease reported a 1.18% decrease in peak height of mean diffusivity and a 10.73% increase in fractional anisotropy in patients with lacunar stroke and leukoaraiosis over 1 year despite unchanged lesion load and brain volume. 78
Diffusion tensor imaging changes correlate more closely to cognitive functioning than the volume of visible small-vessel disease–related changes such as WMLs. So far, only few longitudinal studies on the relationship between increase of microstructural damage and cognitive decline are available. We know even less about the relationship between longitudinal MTI measures and cognition.
Results from the LADIS study showed that microstructural changes, detected with diffusion weighted imaging in normal appearing brain tissue, predict faster decline in cognitive parameters. 79 In a longitudinal study, in 62 CADASIL subjects the changes in mean diffusivity correlated with changes in the Rankin score, national institute of health stroke scale and structured interview for the diagnosis of dementia of the Alzheimer type, multiinfarct dementia and dementias of other aetiology within a 2-year observation period. 28
Diffusion tensor imaging was also used in early detection80,81 and monitoring of disease progression from mild cognitive impairment to Alzheimer's disease. 82
Sample size calculation based on 2-year follow-up data in CADASIL patients showed that one would need 1,944 subjects per treatment arm to show a treatment effect of 20% with an 80% power when mean diffusivity is used as the trial outcome. 28
Conclusions
Presently, only confluent WMLs are MRI correlates of cerebral SVD for which a vascular origin, fast progression, and relation to cognitive decline has been established. Lacunes may fulfill these prerequisites in selective patient samples but in the general population the occurrence of new lacunes over short time periods is rather small and sample size in trials focusing on lacunes would therefore need to be large. In line with current data, confluent WMLs are ideal surrogate markers in proof-of-concept studies in patients with subcortical vascular cognitive impairment. However, if such trials aim to show slowing of cognitive decline resulting from treatment effects on WML progression, sample sizes will need to increase remarkably. Up to now, only few proof-of-concept studies on vascular cognitive impairment have included WMLs. The effect of antihypertensive therapy and statin use on WML progression was evaluated in the PROspective Study of Pravastatin in the Elderly at Risk study and in the Perindopril Protection Against Recurrent Stroke Study.11,83
The MRI substudy of PROspective Study of Pravastatin in the Elderly at Risk assessed the influence of daily therapy with pravastatin on the progression of ischemic brain lesions, including WMLs. After a mean time period of 33 months, there was no difference in progression of WML volume between the 265 participants in the treatment group versus the 270 participants in the placebo arm.
Perindopril Protection Against Recurrent Stroke Study examined whether blood pressure lowering therapy with perindopril and indapamide reduces the progression of WMLs in patients with cerebrovascular disease. The study included 192 individuals who had cerebral MRI at baseline and after 36 months. The authors found that an active blood pressure–lowering regimen stopped or delayed the progression of WMLs.
Recent data from the Vitamins To Prevent Stroke study showed that daily B-vitamin supplementation for 2 years did not significantly reduce the progression of WML volume in a sample of 359 patients with recent stroke or transient ischemic attack and cerebral SVD, but may do so in the subgroup of patients with severe cerebral SVD. 84 These studies provide important first evidence for possible treatment strategies in cerebral SVD, which is still a severely understudied disorder with important implications on the functional status of our aging population. The perspective of new treatment targets originating from recent genetic association studies 85 underscores the importance of having validated surrogate markers, which will allow to conduct proof-of-concept studies in a timely manner at relatively low cost.
Footnotes
Funding
The authors disclosed no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.