
Abstract
Several potential vascular risk factors exist for the development and accumulation of subcortical white matter disease in older people. We have reported that in older people followed for up to 4 years white matter hyperintensity (WMH) lesions on magnetic resonance imaging nearly doubled in volume and were associated with alterations in mobility and cognitive function. Herein we review the genetic, metabolic, and vascular risk factors that have been evaluated in association with the development and pathogenesis of WMH in older persons. Our research efforts have focused on systemic hypertension, particularly in the out-of-office setting as 24-hour ambulatory blood pressure (BP) has proven to be a stronger indicator of the progression of WMH in older people and the associated functional decline than doctor’s office BP. Based on relations between 24-hour systolic BP levels, the accrual of WMH, and functional decline, we have designed the INFINITY trial, the first interventional study to use ambulatory BP to guide antihypertensive therapy to address this problem in the geriatric population.
Keywords
Introduction
White Matter Hyperintensity Lesions and Functional Decline
White matter hyperintensities that represent small vessel brain disease are associated with vascular risk factors, including hypertension, in older people.1,2 The postmortem histopathology of white matter hyperintensity (WMH) shows nonspecific brain changes with gliosis, loss of myelin and axons from arteriosclerosis, tissue rarefaction and lipohyalinosis.3,4 Although the pathophysiology of WMH remains unclear, there are several proposed mechanisms including hypoxia, hypoperfusion because of altered cerebrovascular autoregulation, blood–brain barrier leakage, inflammation, degeneration, and amyloid angiopathy. 5 Marstrand et al. 6 demonstrated that cerebral blood flow and cerebrovascular reactivity were reduced in areas of WMH making tissue damage more likely during hypoperfusion states.
In most instances, WMH lesions are bilateral and symmetrical on T2-weighted magnetic resonance imaging (MRI). They are distributed in the periventricular and deep white matter regions and less frequently in the infratentorial areas of the brain. On computed tomography scan, WMH lesions appear as hypodensities.1,7 They are commonly assessed using visual rating scales, such as Fazekas scale and Scheltens scale.
5
Another approach uses semiautomated, computerized analyses of the MRIs providing a quantitative distribution of cerebral small vessel brain disease lesions suitable for longitudinal numerical comparisons and regional localizations (Figure 1).
8
The figure depicts the location and frequency of white matter hyperintensities captured over three time points during 4 years of prospective evaluation (baseline (left column), 2 years (center column), and 4 years (right column) in 67 older study participants. The white matter hyperintensities are overlaid on the grayscale slice (0.87 m thickness) of the common anatomical brain (International Consortium of Brain Mapping). Columns show two slices separated by 12.2 mm. The vertical color bar represents the frequency (%) of white matter hyperintensities (e.g., color corresponding to 70% indicates the percent of participants with the white matter hyperintensities in that brain area. The lettering below the color bar indicates right (R), left (L), anterior (A), and posterior (P) brain aspects. From Wolfson et al.
8
with permission from Oxford University Press on behalf of The Gerontological Society of America.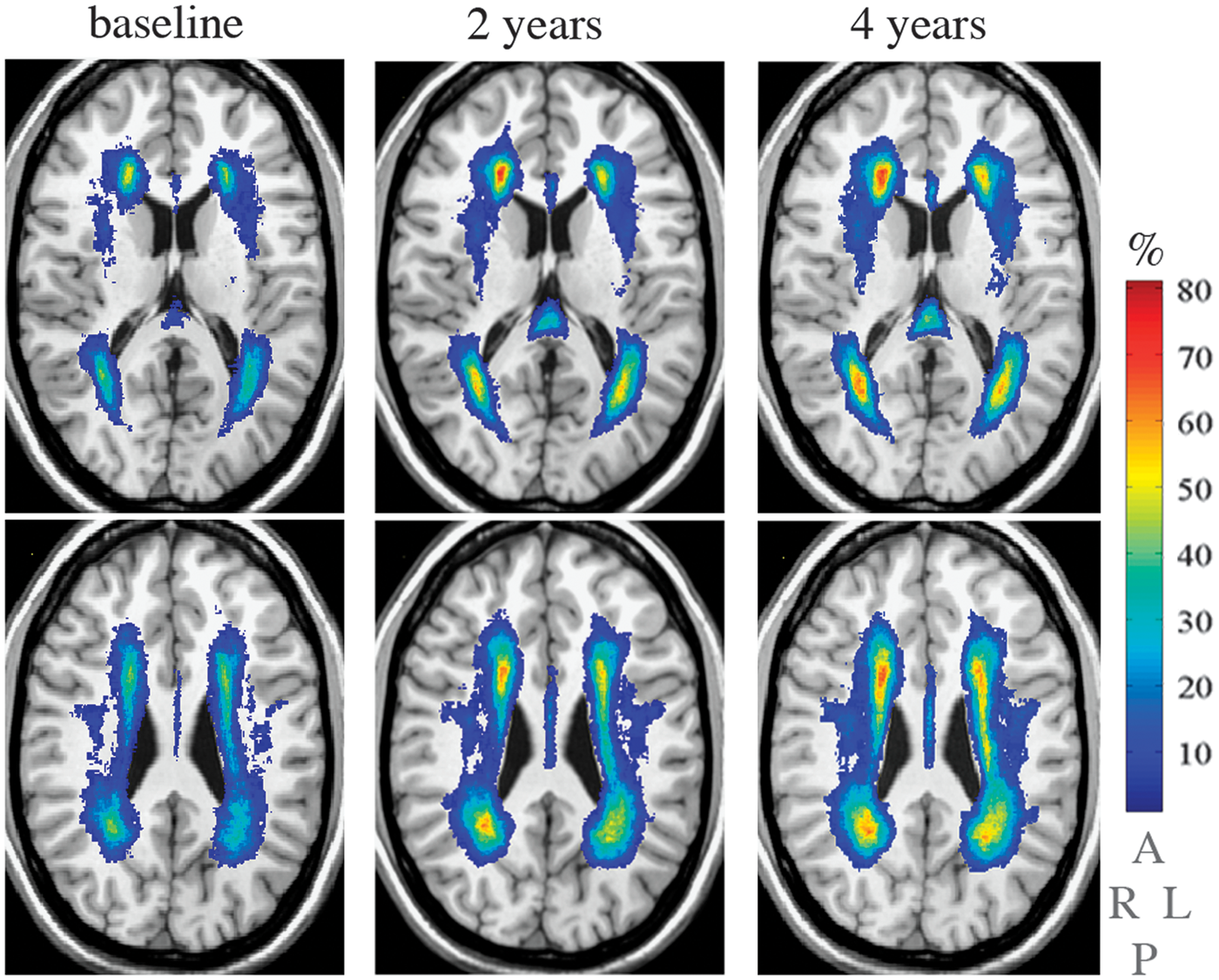
Cognitive function
Higher white matter disease burden is associated with impaired cognitive function, mobility impairment, depression, and impaired urinary function.1,9,10 The frequency of falls even in the absence of obvious neurologic deficits is more common in people with WMH lesions. 8
Cognitive impairment has been studied extensively in persons with WMH lesions on MRI.9,11–
18
Perceived cognitive dysfunction as measured by Cognitive Difficulties Scale was found to be worse with higher WMH burden and the annual rate of decline on the mini-mental status examination was 0.035 points per standard deviation increase in periventricular WMH.
19
In addition, steeper declines in performance are found on measures of speed of processing and executive functioning, such as the Stroop Color Word test (
Importantly, among patients with a history of stroke and/or transient ischemic attack in the Perindopril Protection Against Recurrent Stroke Study, the dementia risk during a median follow-up period of 3.9 years was found to be 7.7 times higher in patients with white matter disease than those without it at the time of study enrolment.
16
A meta-analysis performed by Debette and Markus
20
also showed a significant association between white matter disease and risk of dementia (odds ratio (OR) 1.9, 95% confidence intervals (CIs), 1.3–2.8,
Mobility and balance
In addition to the aforementioned relationships between WMH burden and cognitive function, small vessel disease of the brain is also associated with impaired gait and balance in the older population.
8
Furthermore, severe WMH burden has been linked to increased risk of falls (relative risk = 1.63, 95% CI, 1.11–2.40).
10
In Leukoaraiosis and DISability Study, walking speed correlated with the white matter disease burden (1.24 ± 0.28 m/s for mild, 1.18 ± 0.32 m/s for moderate, 1.09 ± 0.31 m/s for severe categorizations respectively;
Genomics of Vascular Risk Factors Associated with White Matter Lesions
White matter hyperintensities volumes are highly correlated in monozygotic twins and greater than in dizygotic twins. In a study involving US twins aged 68–79 years, the concordance rate for white matter disease (WMH > 0.5% of total intracranial volume) is 61% in monozygotic twins and 38% in dizygotic twins. 23 These data are suggestive of a genetic component in the etiology of cerebral small vessel disease.
Mutations in the NOTCH3 gene result in a syndrome of cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy, which has clinicopathologic features similar to age-related cerebral small vessel disease.
24
Schmidt et al.
25
found four common single-nucleotide polymorphisms (SNPs) (minor allele frequency ≥5%)—rs1043994, rs10404382, rs10423702, and rs1043997—scattered over the
In the Ohasama study in Japan, the homozygous deletion (DD) polymorphism of adrenomedullin 2 (also known as intermedin or IMD) gene is associated with increased prevalence of WMH (66.7%) compared with 39.4% and 43.4% with homozygous insertion (II) and heterozygous carriers (ID), respectively (
Using targeted genome-wide association analyses, French et al. demonstrated that a forkhead transcription factor (FOXC1) mutation adjacent to a cerebral small vessel disease locus resulted in the development of WMH lesions. Cerebral small vessel disease was evident with this gene mutation in individuals as young as 1 year. Mutations of the FOXC1-interacting transcription factor PITX2 gene were associated with phenotypes that develop WMH. 29 In another analysis, SNPs for the gene encoding angiotensinogen (AGT rs699) was found to be correlated with the development and progression of WMH, particularly in the deep white matter, and independent of hypertension. 30 Patients with such genetic variations have been reported to have high levels of angiotensinogen.30,31
Recently, the presence of haptoglobin 1 allele (Hp 1-1) in patients with Type 1 diabetes mellitus from the participants of the Pittsburgh Epidemiology of Diabetes Complication study was found to increase WMH burden but not lacunar infarcts and gray matter atrophy. 32 Associations were strongest for the interhemispheric connecting fibers of the corpus callosum. The Hp 1-1 genotype is also associated with development of stroke in Type 1 diabetes. 33
Metabolic Factors Related to Cerebral Small Vessel Disease
A number of metabolic biomarkers have been studied in small caliber vascular disease in the brain, including individuals with diabetes mellitus, dyslipidemia, homocystinemia, and the metabolic syndrome. A strong association between metabolic syndrome and the presence of subcortical (OR = 1.99; 95% CI, 1.28–3.10;
Findings relating glycemic status, WMH lesions, and/or cognitive function are variable in the literature. For example, in a population of patients with Type 1 diabetes mellitus aged 25–40 years (mean hemoglobin A1c of 7.8), there was no difference in WMH lesions compared with nondiabetic control group and in 3,300 elderly people. The Cardiovascular Health Study did not find any correlation between fasting blood glucose and white matter disease.
36
In contrast, in a study of healthy old people, a linear positive association was found between fasting glucose and subclinical cerebrovascular disease (
Nonglycemic biomarkers and white matter lesions
Homocysteine, an important inflammatory marker associated with atherosclerosis and large artery vascular disease, has also been found to be strongly associated with the development of dementia, including Alzheimer’s disease, in a sample from the Framingham study.
40
In addition, an analysis of 259 stroke-free participants from the Northern Manhattan Study found that total homocysteine levels >1 s.d. above the mean (>11.9
Other studies have also suggested a relationship between endothelial dysfunction, inflammatory endothelial activation, and the extent of white matter lesions in older people. In a study from Hong Kong in 175 older people without neurologic deficits, the measured plasma concentration of soluble ICAM-1 was associated with the severity of WMH, independent of age, and hypertension.
43
In fact, patients in the highest quartile of plasma sICAM-1 had fourfold increased risk of developing WMH. In the population-based Rotterdam Scan study, strong associations between the presence and progression at 3.3 years of WMH lesions and serum C-reactive protein level (OR, 3.1 and 5.6 for periventricular WM and subcortical white matter, respectively) were observed in 636 participants, including after adjustments for conventional cardiovascular risk factors and the presence of carotid atherosclerosis.
4
In contrast, among a Japanese community based study of 689 older people, the serum C-reactive protein level was lower than that observed in the Rotterdam study and was not associated with presence of WMH lesions after controlling for other vascular risk factors and carotid disease.
44
Hence, the importance of C-reactive protein in association with WMH lesions may be heterogeneous depending on the ethnicity and race. Other inflammatory and prothrombotic markers that have been correlated with WMH lesions in smaller studies include plasma nitric oxide metabolites and urinary 8-iso-prostaglandin F2
Lipoproteins
Similar to the glycemic data noted above, studies have shown heterogeneous findings relating lipid abnormalities to small vessel disease of the brain. Fukuda and Kitani
47
reported no correlation between lipid abnormalities (defined as total cholesterol > 220 mg/dL, triglycerides > 150 mg/dL, high-density lipoprotein < 40 mg/dL, low-density lipoprotein (LDL) > 130 mg/dL) and WMH lesions among 253 patients (mean age = 66 years) receiving no medical therapy for dyslipidemia. Population-based data from the 3C-Dojon Study (
In a separate study of patients who had sustained an acute ischemic stroke, Jimenez-Conde et al.
50
reported that hyperlipidemia (defined as prestroke recorded serum cholesterol concentration >220 mg/dL or serum triglyceride concentration >150 mg/dL, and use of medication prescribed to control hyperlipidemia) may have a protective role in cerebral small vessel disease among patients with acute ischemic stroke (
The Importance of Blood Pressure as a Risk Factor for White Matter Lesions and Functional Decline in Older Persons
Comparison of some characteristics of stroke and white matter hyperintensity lesionsa.
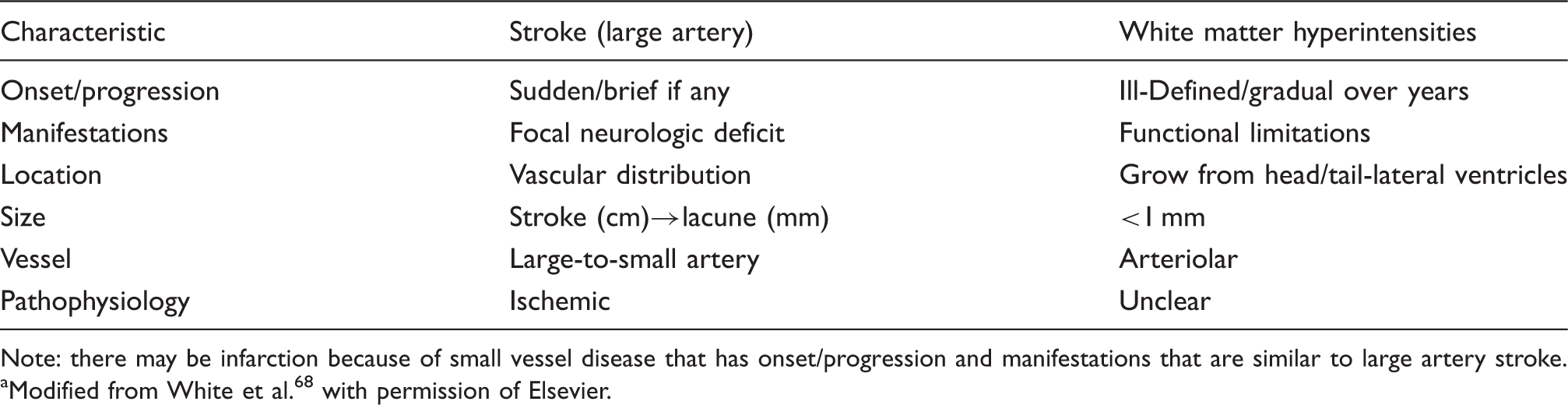
Note: there may be infarction because of small vessel disease that has onset/progression and manifestations that are similar to large artery stroke.
Modified from White et al.68 with permission of Elsevier.
White matter lesions have also been associated with deterioration of mobility, urinary control, and cognition. 59 – 64 Evidence of WMHs within brain pathways known to support mobility, cognition or voiding confirms this association.63,64 Details seen on MRI of the brain have allowed localization and quantification of the disseminated WMHs. 65 Cross-sectional and prospective cohort studies have documented the relationships among WMHs and neurologic function in older people and the distinctive nature of the distribution and volume of brain WMHs that are responsible for deterioration of these functions, particularly in older groups. Approximately two-thirds of individuals over 75 years of age have detectable WMH using MRI of the brain. 54 The lower limit of detection of WMH by experts in neuroradiology is ∼0.2–0.3% of intracranial contents and 0.5% is easily visible to the naked eye based on our experience.8,54,65 Our cohort studies have demonstrated an increase of WMH volume from 0.99 to 1.47 to 1.7% of the intracranial contents volume from baseline to 2 and 4 years, respectively.8,54 This increase was even present in participants with normal mobility throughout the study period.
We have also observed that progression of WMH over time was strongly linked to the initial presence of WMH.8,66 We have observed that accumulation of WMH often occurred by expansion of preexisting periventricular lesions in a stereotyped manner. Regional analysis of the distribution of WMH lesions demonstrated a robust link to expansion of lesions in the splenium of the corpus callosum, a posterior periventricular structure important for the integration of cortical sensorimotor function. 66
Blood pressure and other cardiovascular risk factors noted above have been related to brain WMH although predictors of quantitative WMH progression and their effect on the function of older persons have not been well understood. In our past work in this area, we have evaluated the progression of WMH over 2 and 4 years in a cohort of 99 patients 75–90 years (mean baseline age, 82 years) who had office and ambulatory BP and volumetric MRI.54,65 Neither clinic (doctor’s office) BP nor changes in clinic BP predicted progression of WMH, while the 24-hour ambulatory BP and changes in ambulatory BP significantly correlated with both WMH volume ( (A) White matter hyperintensity and ambulatory blood pressure. Locally weighted scatterplot smoother plots of 24-hour average systolic blood pressure and white matter hyperintensity lesions (as percent of total intracranial volume); (a) change in 24-hour systolic blood pressure and white matter hyperintensity (%); (b) and change in 24-hour systolic blood pressure and change in white matter hyperintensity (%) at 24 months (c). (B) White matter hyperintensity and clinic blood pressure. Locally weighted scatterplot smoother plots of clinical systolic blood pressure and WMH lesions (as percent of total intracranial volume); (a) change in clinical systolic blood pressure and white matter hyperintensity (%); (b) and change in clinical systolic blood pressure and change in white matter hyperintensity (%) at 24 months (c). From White et al.
54
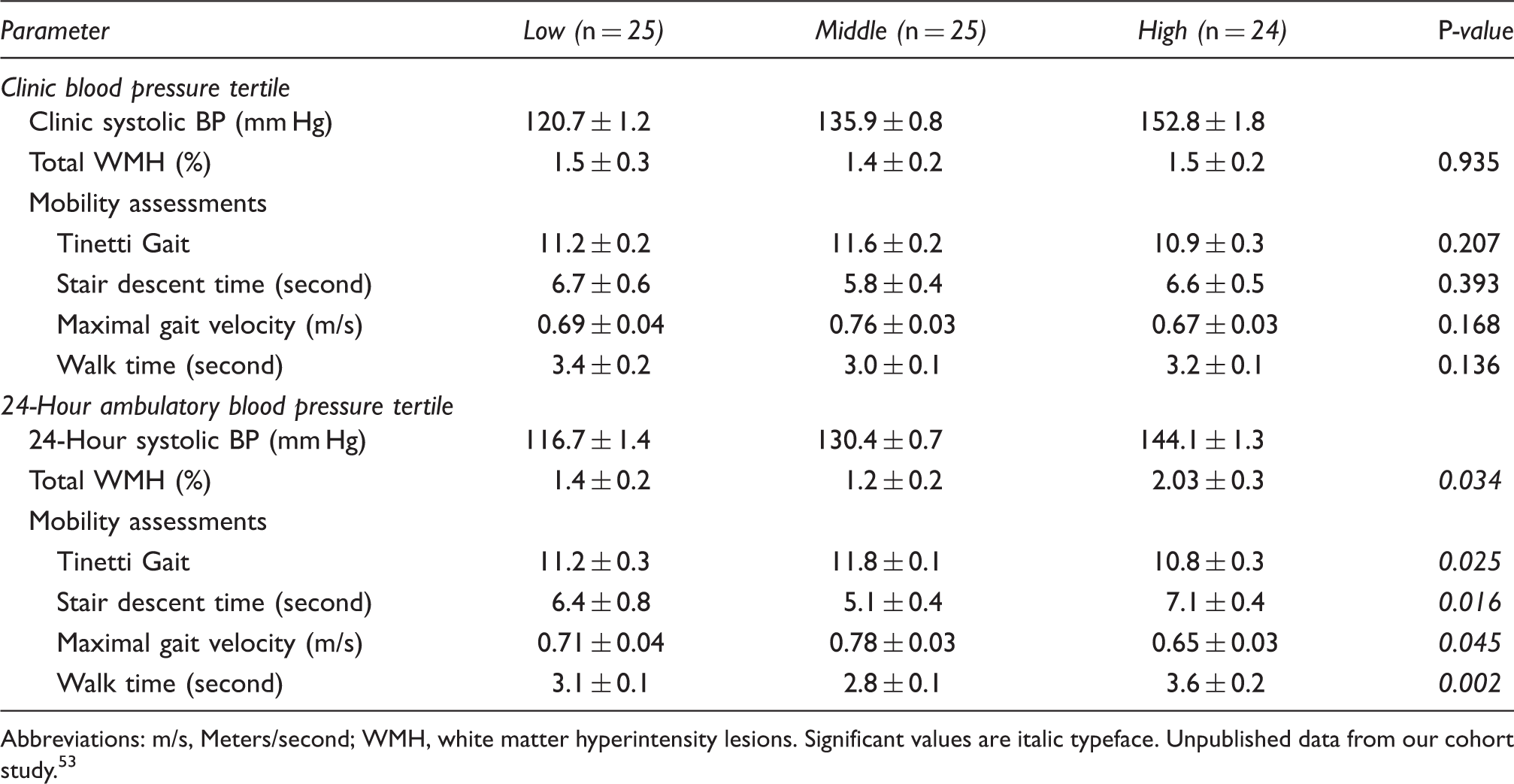
with permission of the American Heart Association. Functional parameters at 24 months of observation according to clinic and ambulatory blood pressure. Abbreviations: m/s, Meters/second; WMH, white matter hyperintensity lesions. Significant values are italic typeface. Unpublished data from our cohort study.53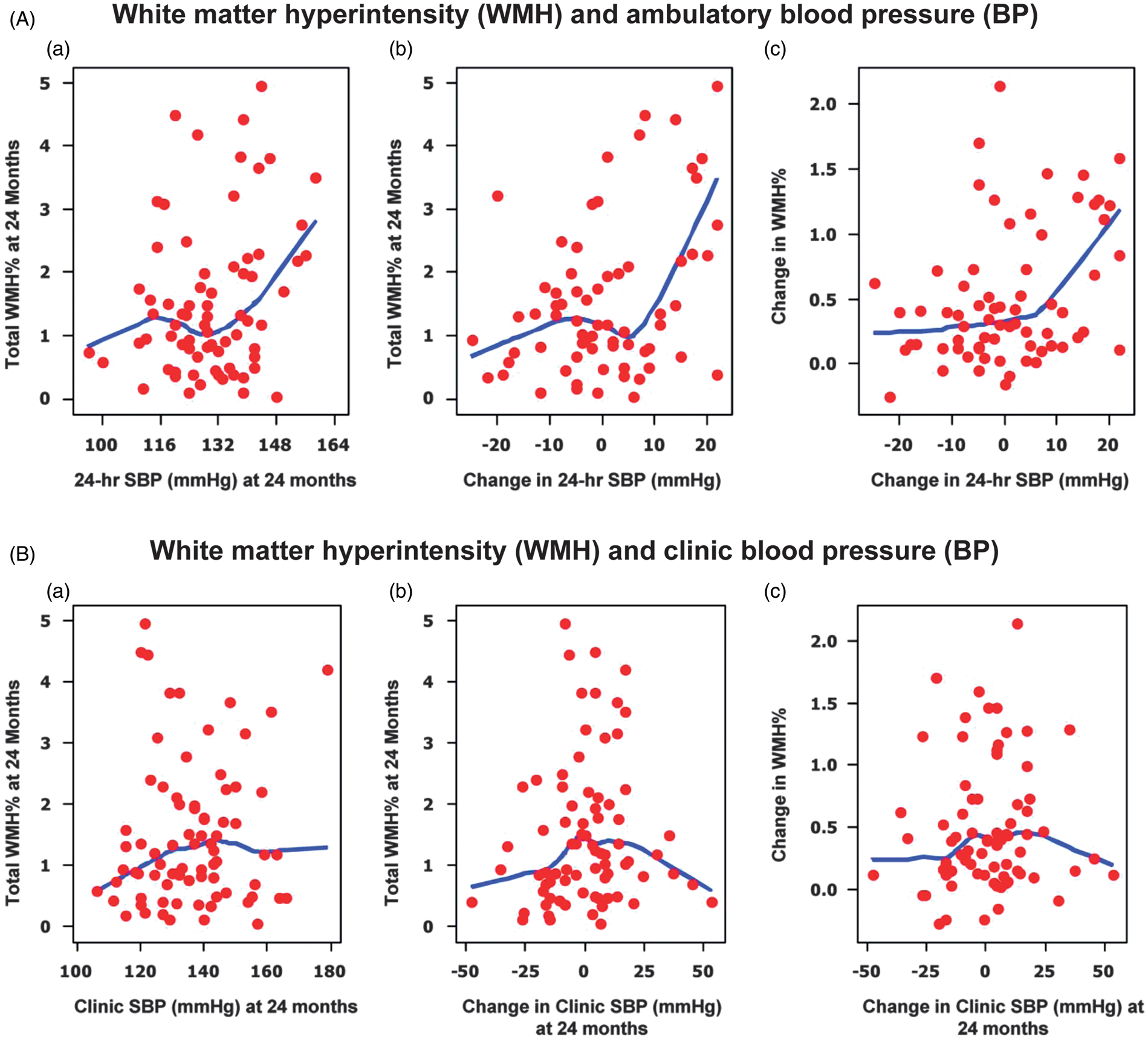
The results of our cohort studies have been supported by a larger longitudinal population-based study of 665 persons from the Rotterdam study.
55
Over a 5-year period, clinical BP and WMH lesion progression was measured 3.5 years apart and after adjusting for baseline WMH, only systolic BP was significantly associated with progression (0.05 mL/year of s.d. increase). Of interest, people with uncontrolled and untreated hypertension had significantly greater white matter lesion progression than people with uncontrolled but treated hypertension (Figure 3). These studies suggest that antihypertensive treatment could reduce white matter lesion progression in uncontrolled hypertension. However, guiding therapy through the use of ambulatory BP monitoring could make this process more precise since ambulatory BP is more reproducible than clinical BP in older people
67
and ambulatory BP recordings would provide a means to target BP elevations during sleep, a period which is strongly related to WMH and cerebrovascular disease.54,68
Mean white matter hyperintensity progression in mL (95% confidence interval; black bars) on top of the baseline white matter lesion volume (gray bars) for four blood pressure categories. Categories were defined as follows based on their mean blood pressure and medication use in the 5 years before the first scan: (1) normotensives: normal mean blood pressure and receiving no antihypertensive medication (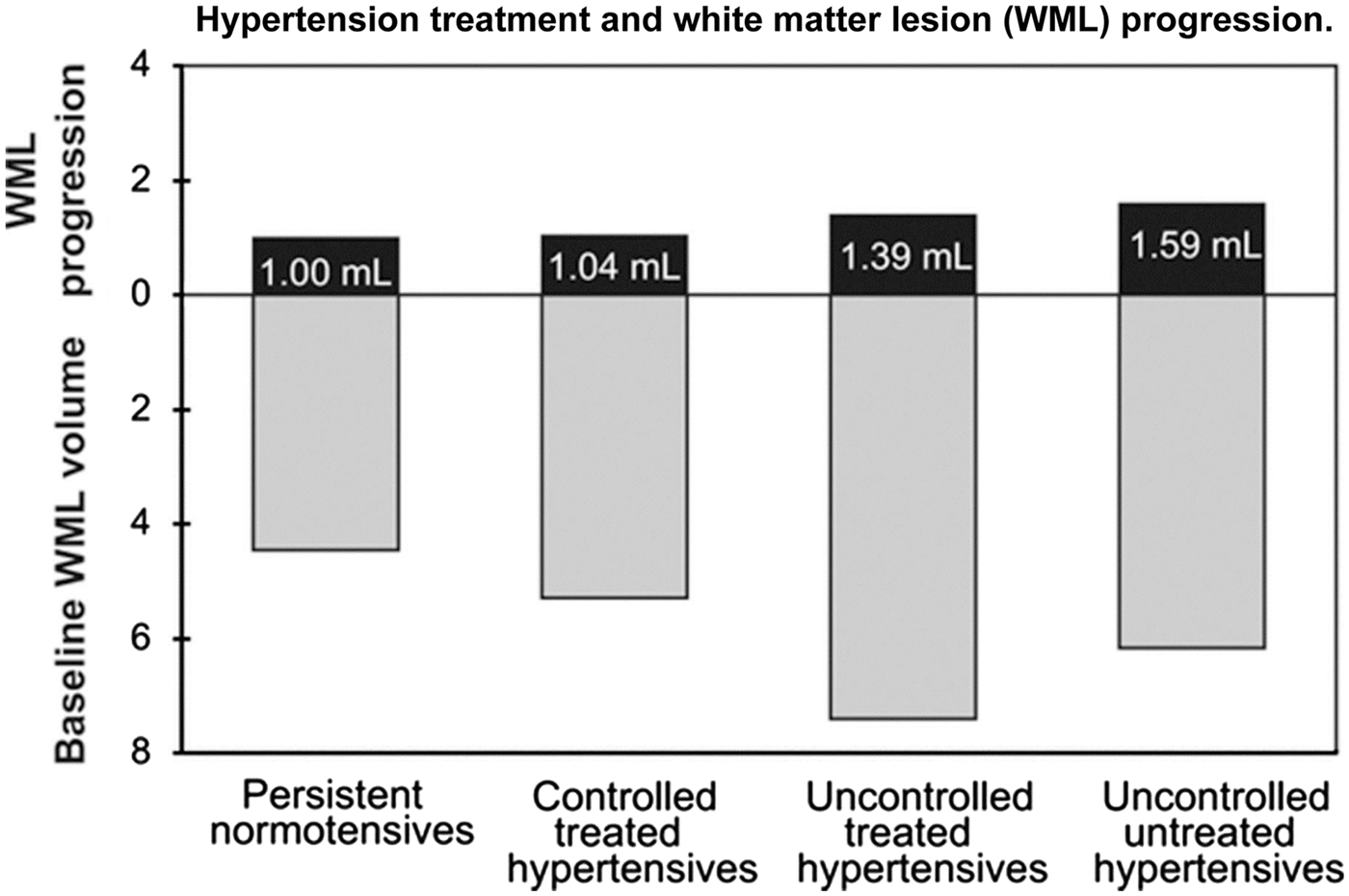
The INFINITY study
The Intensive versus Standard Ambulatory Blood Pressure Lowering to Prevent Functional DecliNe in The ElderlY (INFINITY) study 69 has been designed to evaluate the functional impact of a clinically relevant separation in 24-hour mean ambulatory systolic BP in an older population (that is, <130 mmHg versus <145 mmHg. The study has been designed to evaluate these two levels of ambulatory BP control in hypertensive individuals 75 years or older with normal or mildly impaired mobility and cognition who already have detectable cerebrovascular disease (≥0.5% WMH fraction of intracranial volume). The key outcomes monitored over the 3 years of the trial are white matter lesion progression and measures of mobility and cognition. INFINITY is a prospective, randomized, open-label trial with blinded end points that will evaluate the changes from baseline in mobility and cognitive function and accumulation of WMH volume and changes in diffusion tensor imaging.
Our objective is to achieve a 24-hour systolic BP of ≤130 mmHg in an intensively treated group or standard goal of 24-hour systolic BP of ≤145 mmHg for a total of 36 months using similar classes of antihypertensive therapies. Data from the Hypertension in the Very Elderly Trial demonstrated that antihypertensive therapy decreases stroke mortality even in patients in their mid-80s.
70
In Hypertension in the Very Elderly Trial, the goal of therapy was to reduce systolic BP to <150 mmHg and this intervention did result in a 39% reduction in stroke mortality that was related to a 15 mmHg difference in systolic BP between the active treatment and placebo groups. To our knowledge, there is no other information on level of systolic BP and cardiovascular outcomes in a hypertensive population over the age of 80 years. Hence, the goal of the standard of care systolic BP in the clinic in this age group is ∼150 mmHg, while the ambulatory BP goal is 145 mmHg. Furthermore, no clinical trial in hypertensive patients has used ambulatory BP to guide therapy and to assess cerebrovascular outcomes. The primary outcome of INFINITY is based on mobility parameters. A regression of gait velocity >8 feet/s on our covariates of age, gender, and 24-hour systolic BP at baseline in our prior cohort study
8
showed an
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been supported by National Institutes of Health R01AG022092 and R01DA024667, and The Lowell P Weicker, Jr. Clinical Research Center, University of Connecticut Health Center, Farmington.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.