
Abstract
Vascular cognitive impairment (VCI) is the diagnostic term used to describe a heterogeneous group of sporadic and hereditary diseases of the large and small blood vessels. Subcortical small vessel disease (SVD) leads to lacunar infarcts and progressive damage to the white matter. Patients with progressive damage to the white matter, referred to as Binswanger’s disease (BD), constitute a spectrum from pure vascular disease to a mixture with neurodegenerative changes. Binswanger’s disease patients are a relatively homogeneous subgroup with hypoxic hypoperfusion, lacunar infarcts, and inflammation that act synergistically to disrupt the blood–brain barrier (BBB) and break down myelin. Identification of this subgroup can be facilitated by multimodal disease markers obtained from clinical, cerebrospinal fluid, neuropsychological, and imaging studies. This consensus statement identifies a potential set of biomarkers based on underlying pathologic changes that could facilitate diagnosis and aid patient selection for future collaborative treatment trials.
Keywords
Introduction
Vascular cognitive impairment (VCI) refers to cognitive alterations caused by vascular disease.1,2 The aging of the populations worldwide and the increase in vascular disease with age has led to projections of major growth in the numbers of patients with VCI over the next 30 years. 2 However, in spite of its growing importance, very few specific treatments, apart from treatments for stroke, have been tested in VCI. In addition, there is increased awareness of the role played by vascular disease and neuroinflammation in accelerating the course of Alzheimer’s disease (AD),3,4,5,6 with some investigators raising the possibility that white-matter changes are the starting point of AD.7,8,9 Several factors have impeded progress in organizing treatment trials in VCI, including heterogeneity of clinical presentations, and lack of pathologic consensus, making identification of homogeneous subpopulations of VCI patients a critical unmet need. 10 The use of biomarkers aids identification of homogeneous patient groups.11,12 Large vessel strokes result in a sporadic pattern of brain damage, making it difficult to predict the natural history. On the contrary, damage to small vessels, involving the subcortical white- and gray-matter nuclei often follows a progressive course with gradual changes over several years, providing information on the natural history, which can be used in treatment trials.13,14,15
Since changes in the subcortical and periventricular white matter accrue over time in the elderly, the deep white matter is a common site for ischemic and inflammatory injury. Patients with subcortical lesions have been separated from the larger group of VCI patients and referred to as subcortical small vessel disease (SVD). The challenge is to identify patients with similar underlying pathologic processes at an early stage through the use of disease markers derived from clinical, imaging, and biochemical studies to establish a relatively homogeneous population to test treatments developed in animal models. This special issue is a consensus statement for treatment guidelines in patients with progressive SVD of the white matter.
Historical perspective
In the early 1900s, clinical/pathology studies by Otto Binswanger, Oskar Fischer, and Alois Alzheimer separated arteriosclerotic dementia with multiple lacunar strokes,
Currently, there is general agreement about the diagnosis of VCI in patients with large vessel strokes due to either thrombosis or embolism, which can be readily seen on neuroimaging. 2 Some of these multi-infarct patients show a cognitive decline with each stroke.23,24 However, diagnosis of vascular dementia due to SVD was more controversial because of the frequent occurrence of white-matter changes in normal elderly, the high incidence of overlap with other neurodegenerative disorders, and the lack of consensus on the use of clinical, cerebrospinal fluid (CSF), neuroimaging, and neuropathologic findings in the diagnosis. 10
Definitions of vascular cognitive impairment
Major diagnostic categories for vascular cognitive impairment patients.
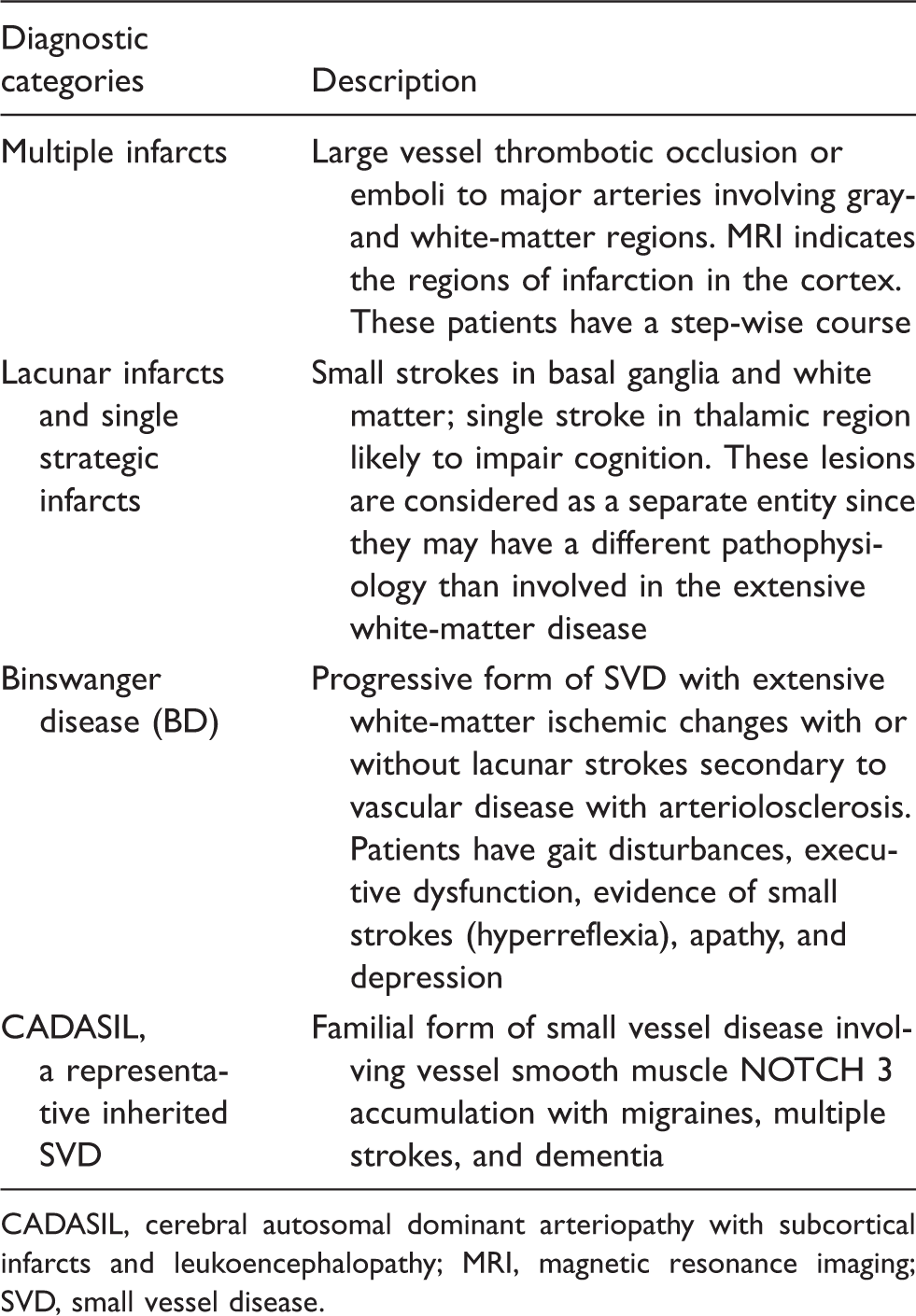
CADASIL, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; MRI, magnetic resonance imaging; SVD, small vessel disease.
Multi-Infarct Dementia
Atherosclerosis of the carotids, vertebral and major intracranial arteries mainly cause large vessel strokes. Emboli from the heart, particularly with atrial fibrillation and from the atherosclerotic aortic arch and carotid generally lead to large strokes, but on occasion showers of small emboli can occur. Initial attempts to standardize diagnostic criteria for multi-infarct dementia required the temporal relationship of the stroke to the decline in cognition, which failed to occur in many patients with a progressive course, which more closely resembled neurodegeneration.21,22 Although temporal relationship between the infarct and the loss of cognitive function was considered as critical for diagnosis, it was soon realized that many patients with vascular causes of dementia had a progressive course that overlapped in the early stages with AD, while MRI showed that many of these patients had abnormal signal in the white matter, suggesting possible cerebrovascular disease.
Subcortical Small Vessel Disease
Small vessel disease is a broad term that includes lesions in subcortical gray and white matter. Small strokes produce lacunes, which can be seen in the basal ganglia and deep white matter. Isolated infarcts in the basal ganglia and thalamus cause stroke-like events with an unpredictable course, and have been classified in the multiple stroke category. Diffuse white-matter lesions, which may have a different pathophysiology, tend to enlarge over time, making it possible to determine a natural history that could potentially be altered by treatment. Lacunes are often present along with extensive white-matter changes, which are often the case in hypertensive SVD.3,27 Studies of the blood–brain barrier (BBB) permeability show increased leakiness in white matter remote from the index infarct in patients with lacunar strokes. 31 Many white-matter hyperintensities (WMHs) may have lacunes at the edges along the course of perforating vessels supplying the respective brain region, which may be a factor in the enlargement of the WMH. 32 Microinfarcts in the cortex, which are being identified with pathologic studies and 7T MRI, are associated with acceleration of AD, but their role in white-matter pathology remains to be established. 33 Many of the patients with sleep apnea have cognitive impairment, but the relationship of sleep apnea to WMHs needs further study. 34
Binswanger’s Disease
Binswanger’s disease (BD) before CT and MRI was an infrequent pathologic diagnosis that was made when there was extensive demyelination associated with arteriolosclerosis of deep white-matter vessels.35,36 Diagnosis before death is now possible from clinical, imaging, and biochemical features; the typical patient with BD has an insidious onset suggestive of small strokes and clinical findings of executive dysfunction on neuropsychological testing, early onset of motor findings with prominent gait impairment, apathy, incontinence, and in the advanced stages, pseudobulbar findings with full-blown dementia.37,38,39,40,41 There is generally a progressive course with some waxing and waning of symptoms. Vascular risk factors are common, particularly hypertension.
34
Congestive heart failure can lead to intermittent symptoms, depending on the cardiac output. Atrial fibrillation with episodic hypoperfusion may be present. Medical diseases, such as hypothyroidism, B12 deficiency, collagen vascular disease, and hematological disorders, need to be ruled out. Cerebrospinal fluid should be tested to exclude infections and in younger patients to rule out multiple sclerosis. Binswanger’s disease is a spectrum disorder; a collection of clinical, imaging, and molecular markers will be needed to approach diagnostic certainty. Diagnosis of BD is complicated by the overlap with AD and white-matter changes of aging (Figure 1).
Venn diagram of the various categories of small vessel vascular cognitive impairment (VCI). White-matter changes of aging or leukoaraiosis indicate that the etiology is uncertain. White-matter changes of aging can overlap with small vessel disease (SVD) in patients with Binswanger’s disease. When Alzheimer’s disease overlaps with SVD, mixed dementia is the appropriate term. Inherited forms of SVD (ISVD), such as CADASIL, are a separate category of SVD. CADASIL, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy.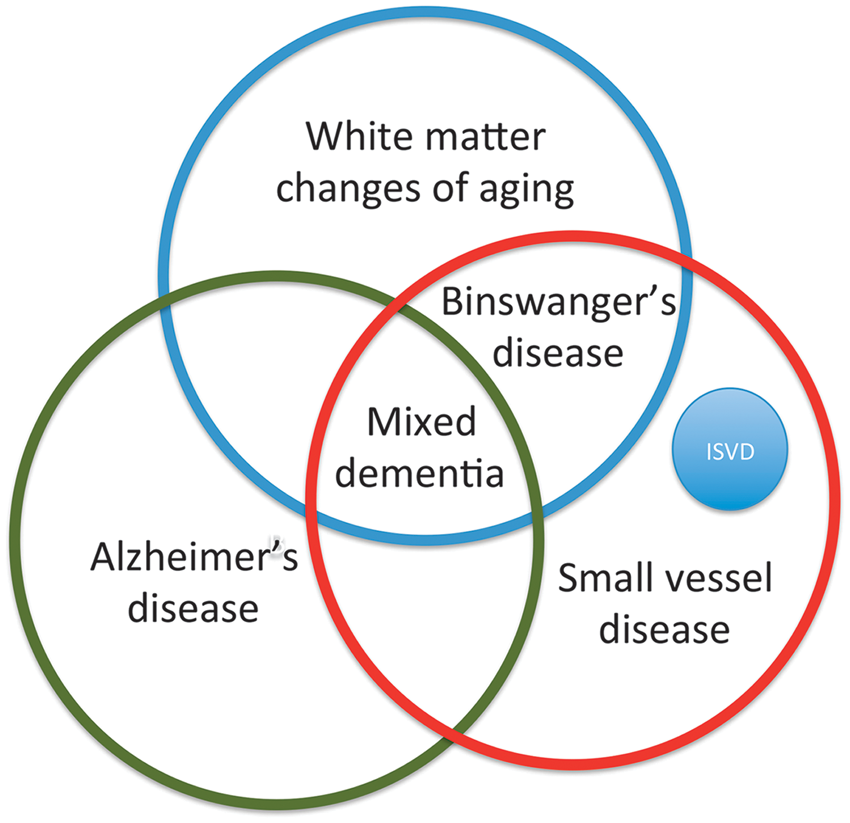
Age-Related White-Matter Damage
Periventricular WMHs are commonly observed in older persons on fluid attenuated inversion recovery (FLAIR) MRI. Population-based and cohort studies have helped to define the course and clinical significance of WMHs in the periventricular and deep white matter. The conclusions reached are highly dependent upon study design, demographics, and definition of WMHs. In community dwelling individuals over the age of 75, using a quantitative definition of WMHs (>0.5% of intracranial volume), periventricular WMHs were found in 2/3 of an age-stratified cohort (75 to 89 y/o) selected for mobility (stratified from normal to impaired) with relatively normal cognition. Over 4 years, the most important risk factors for progression were age, hypertension, and WMH volume at baseline with the cohort demonstrating significant decrements of mobility and measures of cognitive processing speed with periventricular WMH accrual from 0.99% to 1.74% of intracranial contents volume. 42 The growth of WMHs occurred by expansion of preexisting periventricular lesions, generally extending outward from the anterior and posterior horns of the lateral ventricles, making it less likely that they were due to acute ischemic pathophysiology. 43 One explanation is that periventricular WMHs are caused by benign venous collagenosis as opposed to deep WMHs that are related to reduced blood flow with hypoxia. 44 Although this condition and BD are linked with hypertension and likely microvascular disease, the age of onset, prevalence, clinical manifestations, rate of progression, and site of lesions differ, suggesting that other factors are also operative. Separation of elderly individuals with age-related periventricular WMHs from those related to BD will aid treatment trials by reducing the numbers of patients to treat.
Inherited Forms of Small Vessel Disease
There are several recognized forms of inherited SVD. Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), the most common inherited SVD, which is a systemic vascular disorder characterized by recurrent subcortical strokes leading to vascular dementia, will be the focus of this review. It is due to a mutation in the
Leukoaraiosis
Leukoaraiosis was derived from the Greek words for ‘white’ and ‘rarified’, and was originally proposed to describe the low signal seen on CT in the white matter for which a concise etiology was lacking. 47 The attenuated signal on CT corresponds to high signal on T2-weighted MRI. The impetus for the use of this descriptive term was originally to avoid the over use of the association of white-matter changes, which were seen in some normal individuals, with the pathologic process in BD. It is a ‘neutral’ term to be used when neither a definite pathologic change nor a specific clinical deficit has been linked with the CT and MR changes. The use of a purely descriptive term was to preclude ‘premature presuppositions’ and encourage the search for causes.
Mixed Dementia
While relatively pure forms of BD and AD are found, it appears that the largest group of patients has a combination of both diseases.5,6,48 This important group of patients has remained essentially undefined, until the advent of amyloid positron emission tomography imaging. 49 These patients generally are older than the typical patient with vascular disease. Often memory impairment is present along with executive dysfunction. White-matter changes are present on the MRI, which may be difficult to differentiate between those accruing over time in the elderly from those due to hypoxic hypoperfusion with incomplete ischemia due to arteriolosclerosis or cerebral amyloid angiopathy; this is an important distinction because the latter group could have both AD and SVD. In the patients with AD, cerebral amyloid angiopathy results in microbleeds that tend to be localized to the posterior white matter, and which are suggestive of mixed type pathology. This group most likely will require multiple treatments related to the vascular and AD aspects of the pathology. The key will be to determine the dominant features early in the course and to initiate treatment directed to the major factors.
Pathophysiology of white-matter injury in small vessel disease
The deep white matter is a watershed region that is vulnerable to reductions in CBF and oxygen delivery.
50
The vasculature supplying the subcortical white matter originates on the cortical surface and narrows as the vessels descend into the deeper regions, leaving white matter around the ventricles vulnerable.
51
Brun has described the damage to the region as ‘incomplete infarction’.
52
Hypertension has the major effect of narrowing the vessel lumen and thickening the vessel outer wall; in spontaneously hypertensive rats (SHR), spironolactone, a potassium-sparing diuretic, used as an antihypertensive, reverses these changes.
53
Arterioles are primarily affected showing arteriolosclerosis, lipohyalinosis, and fibrinoid necrosis.30,54 The narrowed lumen restricts CBF producing an intermittently hypoxic environment. The vessels become stiff and respond poorly to dilatation in response to reduced blood pressure (cerebrovascular autoregulation) or when there is a need to increase the supply of oxygen, such as during brain activation.55,56 This leads to induction of hypoxia inducible factor-1 Hypothetical pathophysiologic mechanisms for white-matter damage secondary to vascular risk factors (hypertension, diabetes etc.). Damage to the blood vessels leads to fibrosis with narrowing of the vessel lumen and thickening of the walls. There is reduction of cerebral blood flow with hypoxia/ischemia that triggers a molecular injury cascade, beginning with hypoxia inducible factor-1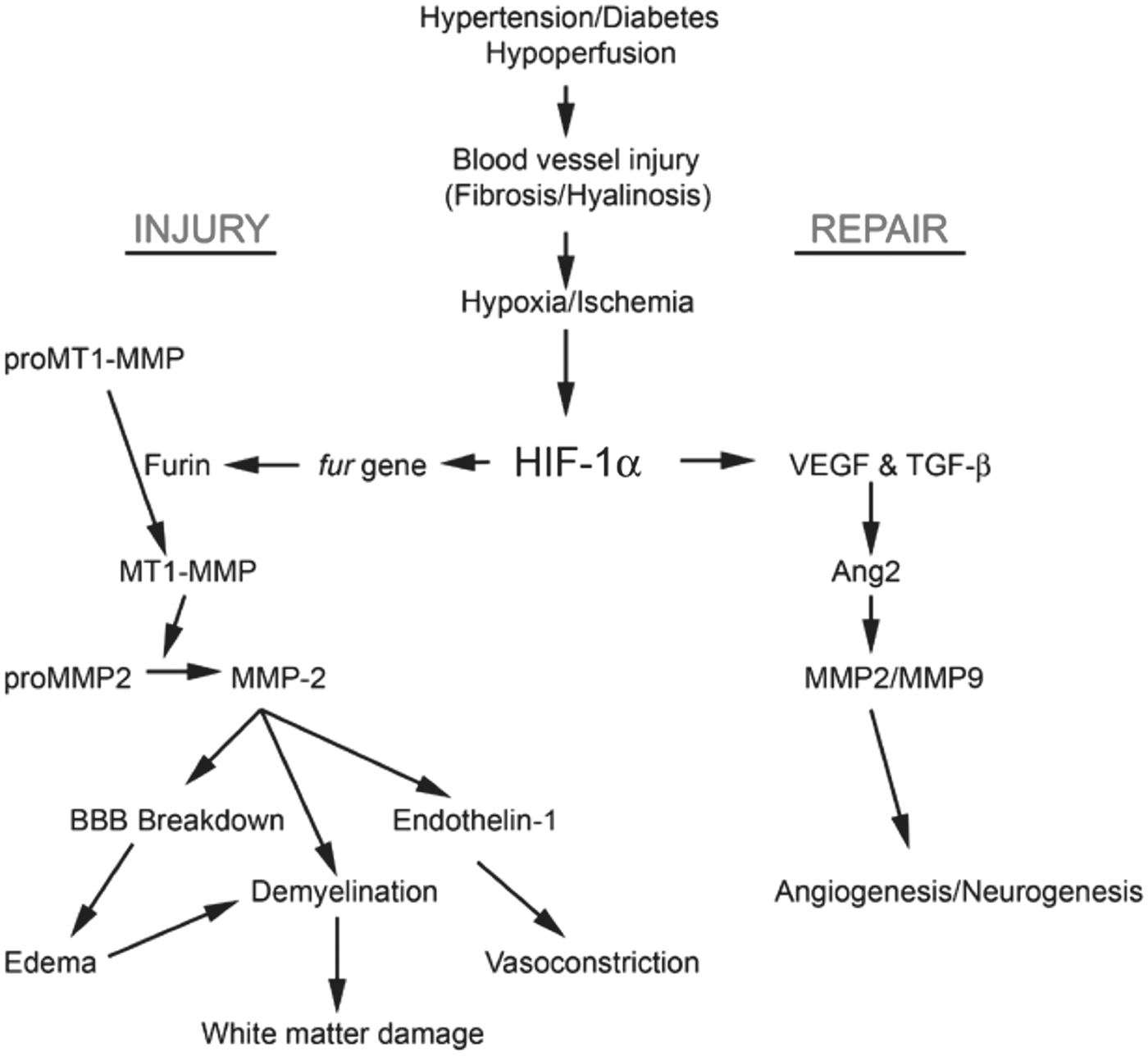
Elevated levels of albumin suggest blood-derived protein crossed a disrupted BBB. 62 Pathologic studies showed blood-derived proteins in the brains of patients with SVD. 63 Magnetic resonance imaging studies with gadolinium-DTPA show increased permeability.64,65,66,67 Patients with lacunar strokes have increased permeability in deep white matter remote from the lacunar infarct, and the increased BBB permeability shortened the time to functional dependency as measured 3 years later. 68 By the time of death, brain tissue shows multiple pathologies, which may or may not reflect the early events, making it necessary to use neuroimaging and CSF markers to identify initiating events.
In CADASIL, pathogenetic mutations in
Patients with SVD often have enlargement of the Virchow-Robin perivascular spaces,73,74 which are associated with amyloid angiopathy, hypertension, and lobar microbleeds.75,76 At this time, the clinical significance of the dilatation of the perivascular spaces remains to be determined.
Diagnostic tests in vascular cognitive impairment
Magnetic Resonance Imaging
Magnetic resonance imaging has dramatically impacted the evaluation of patients with cerebrovascular disease through the sensitivity to white-matter changes and lacunar infarcts. 77 Magnetic resonance imaging is essential for initial screening of patients for cortical infarcts, lacunes, WMHs, microbleeds, enlarged perivascular spaces, and cortical atrophy. However, the MRI has limitations as a diagnostic tool because of the poor specificity and the significant numbers of normal elderly with moderate to severe WMHs of uncertain etiology.78,79 Neuropathologic validation of imaging findings is complicated by alterations of postmortem brain tissue.80,81
Magnetic resonance neuroimaging diagnostic tests useful in evaluation of patients with VCI.
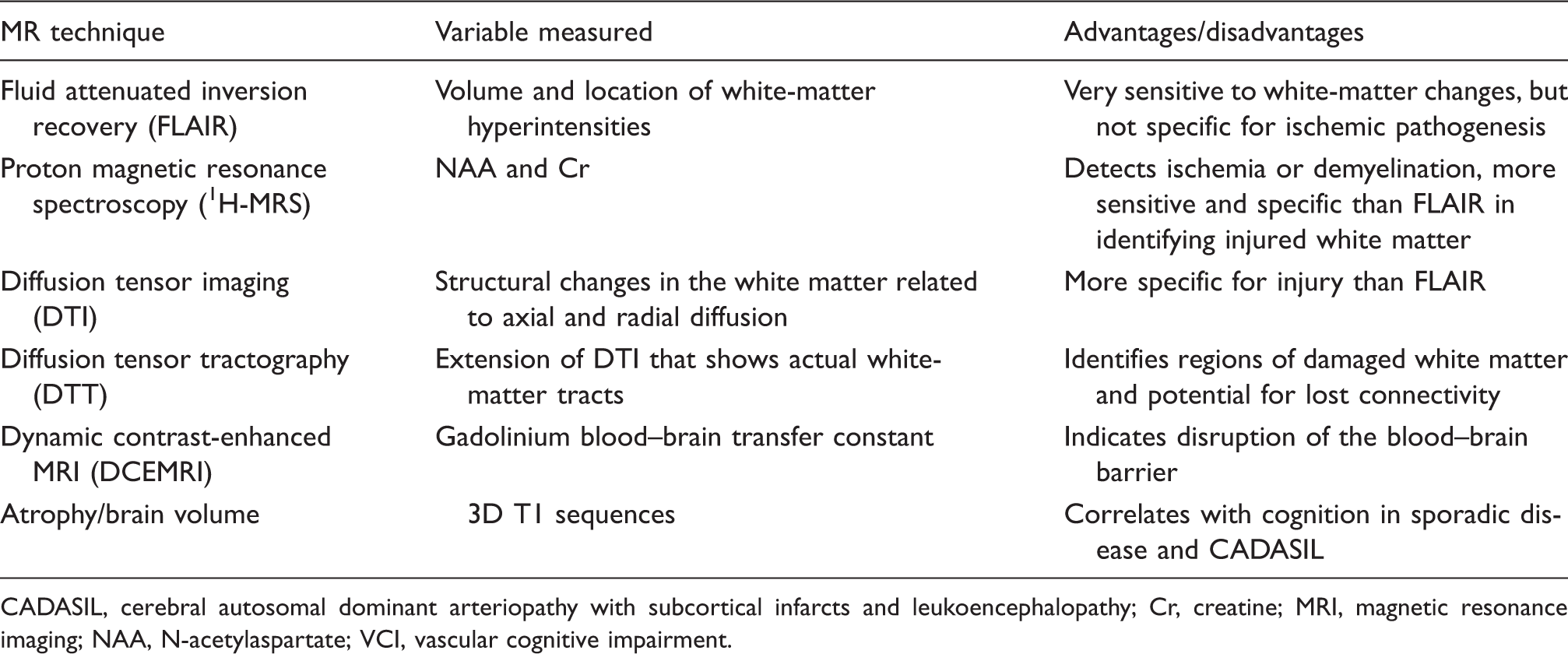
CADASIL, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; Cr, creatine; MRI, magnetic resonance imaging; NAA, N-acetylaspartate; VCI, vascular cognitive impairment.
NMR Spectroscopy and Diffusion Tensor Imaging
Other MR techniques that are more sensitive to pathologic changes in the white matter are proton NMR spectroscopy (1H-MRS) and DTI. 1H-MRS, which shows reductions in
Diffusion tensor imaging is a sensitive method to show microstructural damage in white matter. There is growing evidence that DTI, particularly the mean diffusivity component, is a more sensitive biomarker of white-matter injury than T2 or FLAIR. Ischemic changes in the white matter can be seen by either 1H-MRS or DTI and the results are comparable. 91 Diffusion tensor imaging allows measurements of fractional anisotropy and mean diffusivity. 92 Quantification of DTI may be confounded by the heterogeneity of white-matter regions with crossing fiber tracts, which can often be overcome with appropriate image processing methods. Methods are needed to standardize groups of patients, and atlases of controls are used to normalize regional variations. 93 A penumbra surrounds WMHs where DTI is less severely affected than in the center of the lesions, but more affected than normal appearing white matter.93,94 Similar changes in DTI in the penumbral region around the WMHs were seen in CADASIL patients who had incident lacunes that arose along the perforating arteries at the edges of the WMHs. 32
Blood–Brain Barrier Permeability Measurements
Measurement of BBB permeability is possible with contrast-enhanced MRI.68,95,96 Quantitative transfer constants for BBB permeability can be obtained with dynamic contrast-enhanced MRI (DCEMRI), using the Graphical Method of Patlak, originally developed for calculation of transfer constants with isotopes and autoradiography, and adapted to human studies with MRI.96,97,98 Increased BBB permeability can be seen in regions of lacunar infarcts and in the deep white matter.64,65,67 In addition to numerical transfer constants, interesting patterns of increased permeability can be seen by the construction of permeability maps, which provide insight into the pathologic changes underlying the increases in permeability. Such maps show a diffuse pattern of permeability change in normal appearing white matter, increased permeability around the WMHs, and reduced permeability within the WMHs (Figure 3). Recently, studies of permeability in gray matter have shown increased permeability of the hippocampus in normal elderly subjects, which was more pronounced in patients with mild cognitive impairment, suggesting a role of the BBB in AD.
99
Representative permeability maps in the white matter obtained with dynamic contrast-enhanced magnetic resonance imaging (DCEMRI). White-matter hyperintensities (WMHs) are colored in green and are derived from fluid attenuated inversion recovery (FLAIR) MRI. The color scale in the right indicates the amount of permeability change with yellow being the highest values and red being the lowest. (a) Upper row shows representative permeability maps for normal subjects. Scattered areas of red show that mild increases in permeability can be seen in normal some of whom have WMHs (white arrows). (b) Lower row shows white-matter permeability maps from several Binswanger’s disease (BD) patients. The large amount of green indicates that they have extensive WMHs. Areas of high permeability, which were not seen in the normal are seen as yellow areas at the edges of the WMHs (white arrows). Normal appearing white matter shows increased permeability. (Figure courtesy of Arvind Caprihan, PhD, MIND Research Network, Albuquerque, NM).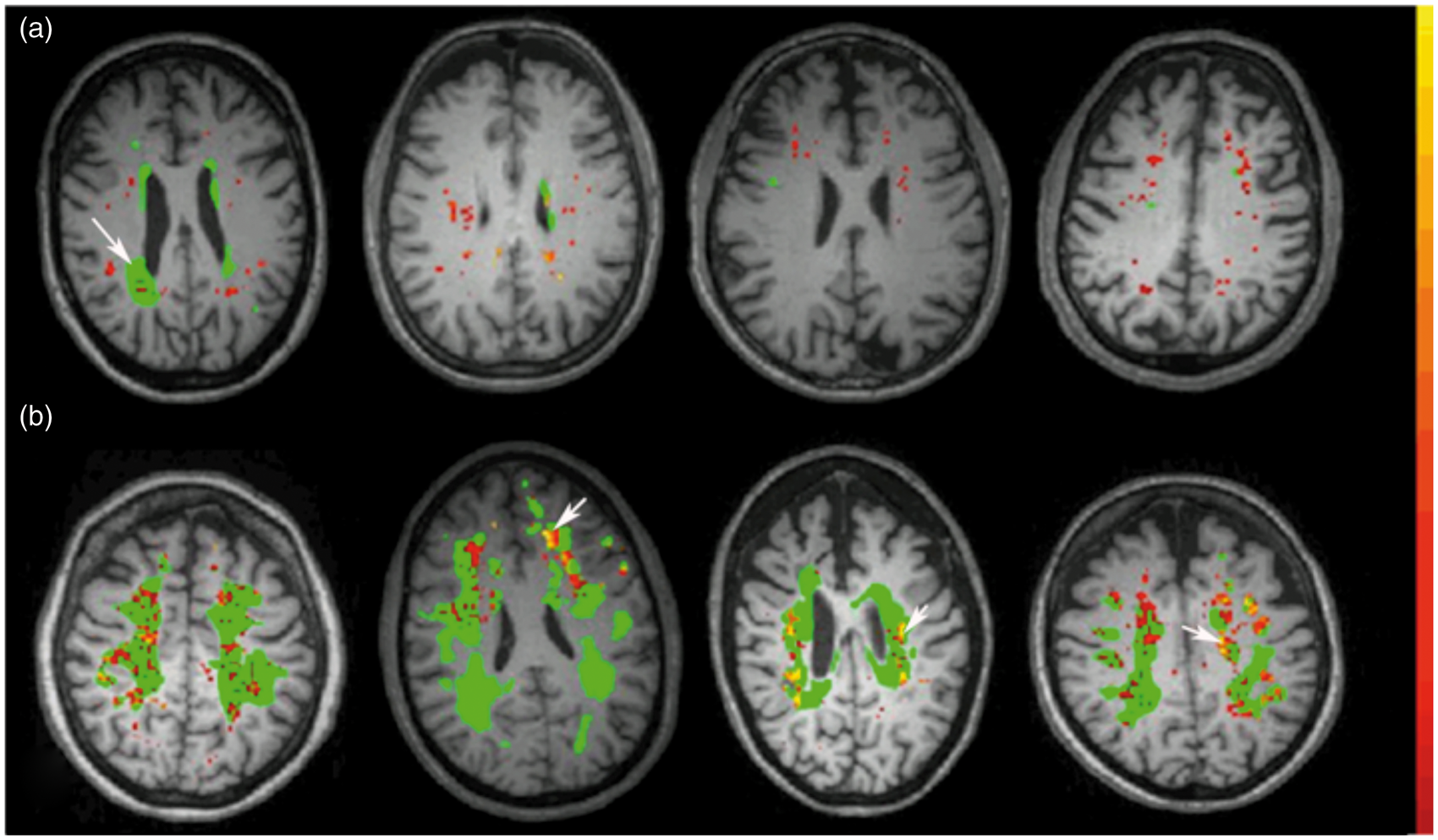
Biochemical Markers in Diagnosis of Small Vessel Disease
Cerebrospinal fluid findings in patients with white-matter injury in VCI.
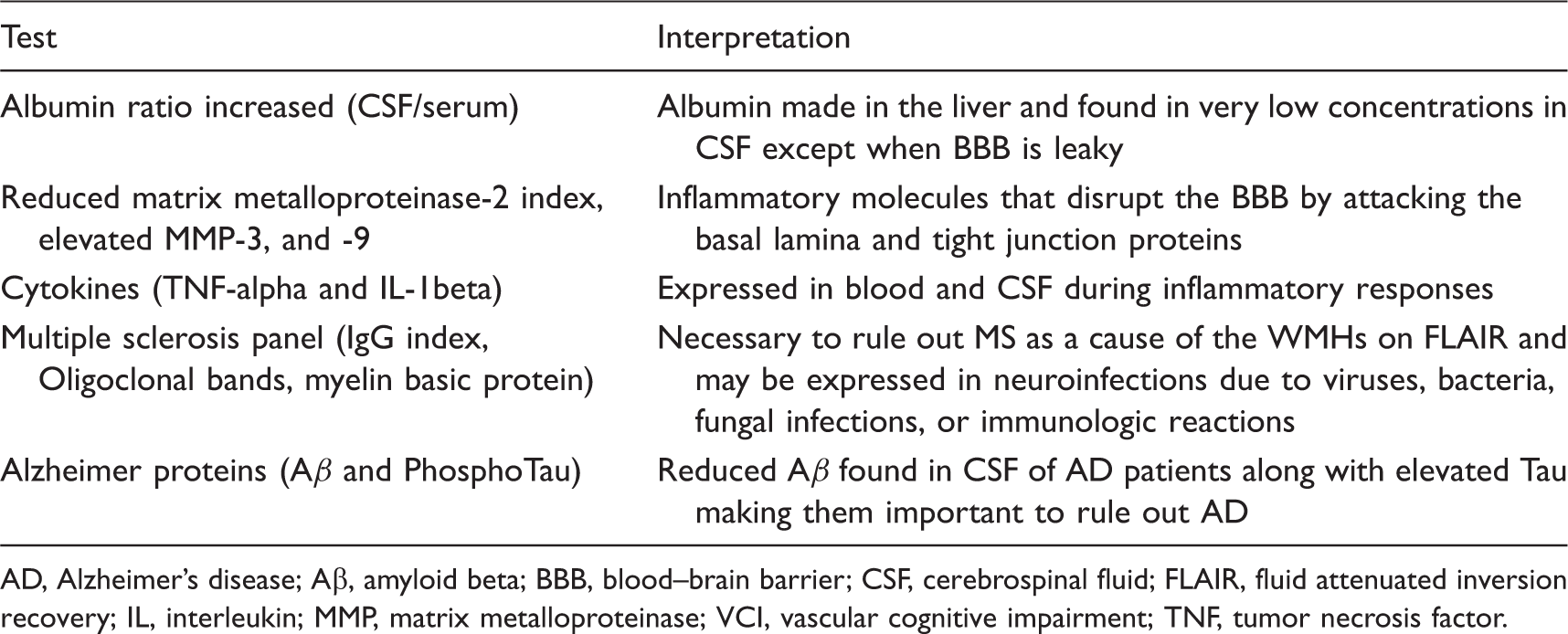
AD, Alzheimer's disease; Aβ, amyloid beta; BBB, blood–brain barrier; CSF, cerebrospinal fluid; FLAIR, fluid attenuated inversion recovery; IL, interleukin; MMP, matrix metalloproteinase; VCI, vascular cognitive impairment; TNF, tumor necrosis factor.
In addition to indicators of BBB opening, the CSF can show neuroinflammation and byproducts of myelin breakdown. Matrix metalloproteinases participate in the neuroinflammatory response by attacking the proteins in the basal lamina around cerebral blood vessels and breaking down the tight junction proteins.59,100,101 During an inflammatory response, there is a shift of the constitutive MMPs to the inducible MMPs that are more disruptive. Inflammation increases the levels of MMP-9 and MMP-3 in the CSF, while the constitutive MMP-2 that is normally present in a proform is reduced in the CSF, most likely due to activation; MMP-3 and -9 are not normally present in CSF, making them readily detectable when elevated in inflammation.102,103,104
Matrix metalloproteinases exist in the blood and move into the CSF when there is disruption of the BBB, contributing to the CSF level. To determine the intrathecal production of MMPs, an index can be calculated by creating ratios with the albumin in the CSF and blood, which is similar to the IgG Index used in the diagnosis of multiple sclerosis.
105
The index is formed as follows: MMP index = [(MMP/albumin)CSF]/[(MMP/albumin)blood]. Combining the MMP-2 index and the MMP-3 activity effectively separates BD from controls (Figure 4).
104
Matrix metalloproteinases are latent and once activated are rapidly removed. Measurements of active MMPs are possible with either gel zymography or immunocapture and fluorometric assays, which are available for the active forms for MMP-3 and MMP-9.
106
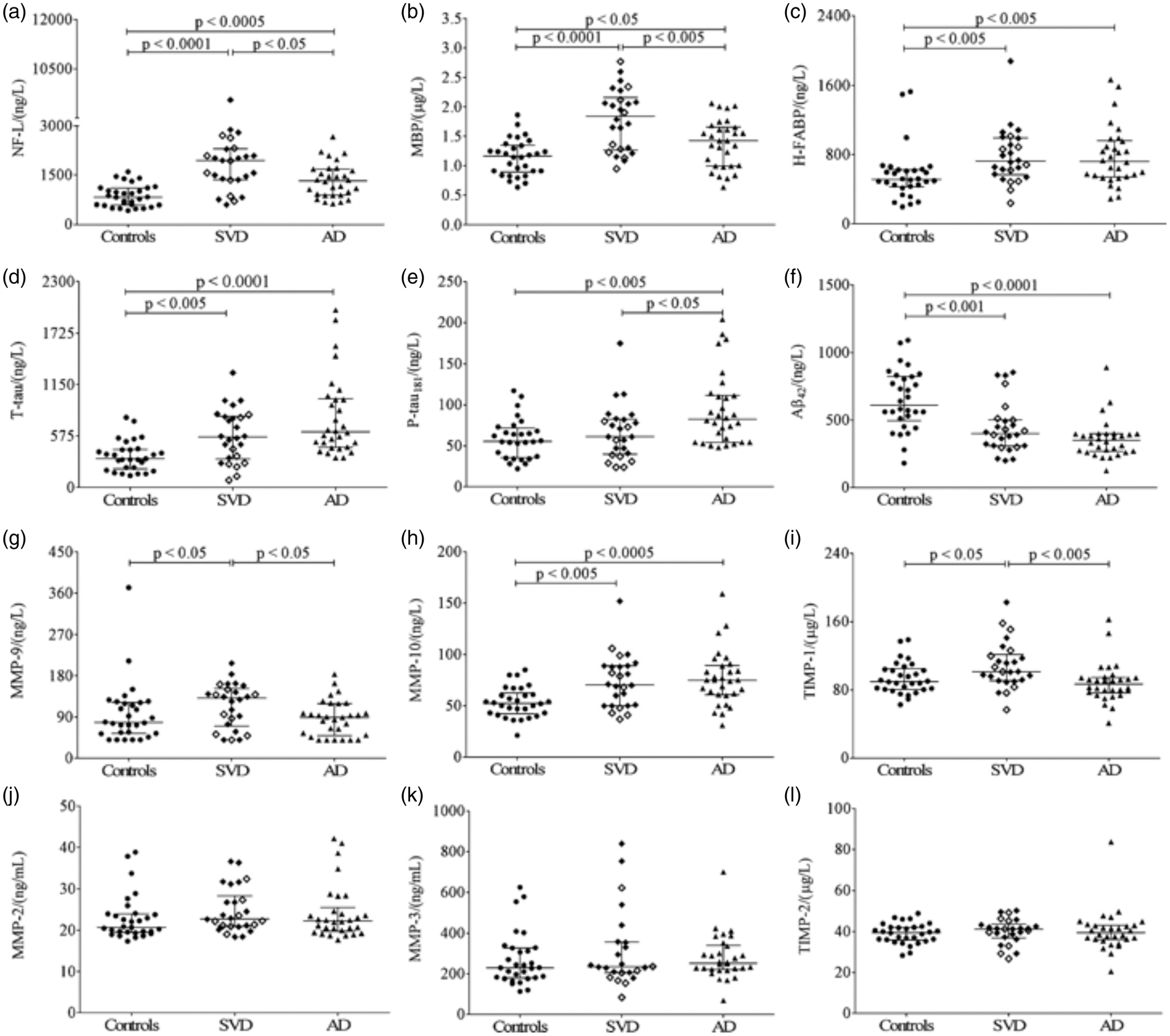
Other CSF biomarkers include neurofilament light, myelin basic protein, and heart fatty acid binding protein.
103
Sulfatide predicted progression of white-matter lesions over 3 years, which may reflect remyelination.
107
Separation of SVD from AD has been shown to be possible in studies of CSF biomarkers. The CSF biomarkers that perform well in differentiating AD and white-matter pathology are phosphylated-tau (p-tau) and amyloid- Relationship of matrix metalloproteinase (MMP)-2 index to MMP-3 activity for the SVD and control groups. (a) Scatter plot of MMP-2 index and MMP-3 activity shows that the controls clustered in the high MMP-2 index and low MMP-3 activity quadrant (black dots). The SVD group clustered in the low MMP-2 index and high MMP-3 activity (red dots). (b) A density plot of the ratio of MMP-2 index to MMP-3 activity shows that the two groups could be separated based on their means with a Scatter plots showing univariate analyses of cerebrospinal fluid (CSF) biomarkers for controls, SVD, and AD. The SVD patient group consists of MD (filled diamonds) and VaD (open diamonds). Error bars are represented by median and interquartile range. (a) neurofilament light (NF-L), note the broken axis; (b) myelin basic protein (MBP); (c) heart fatty acid binding protein (H-FABP); (d) total tau (T-tau), one missing value (mv) in controls; (e) tau phosphorylated at threonine 181 (P-tau181), two mv in controls and one in MD; (f) amyloid beta 1–42 (A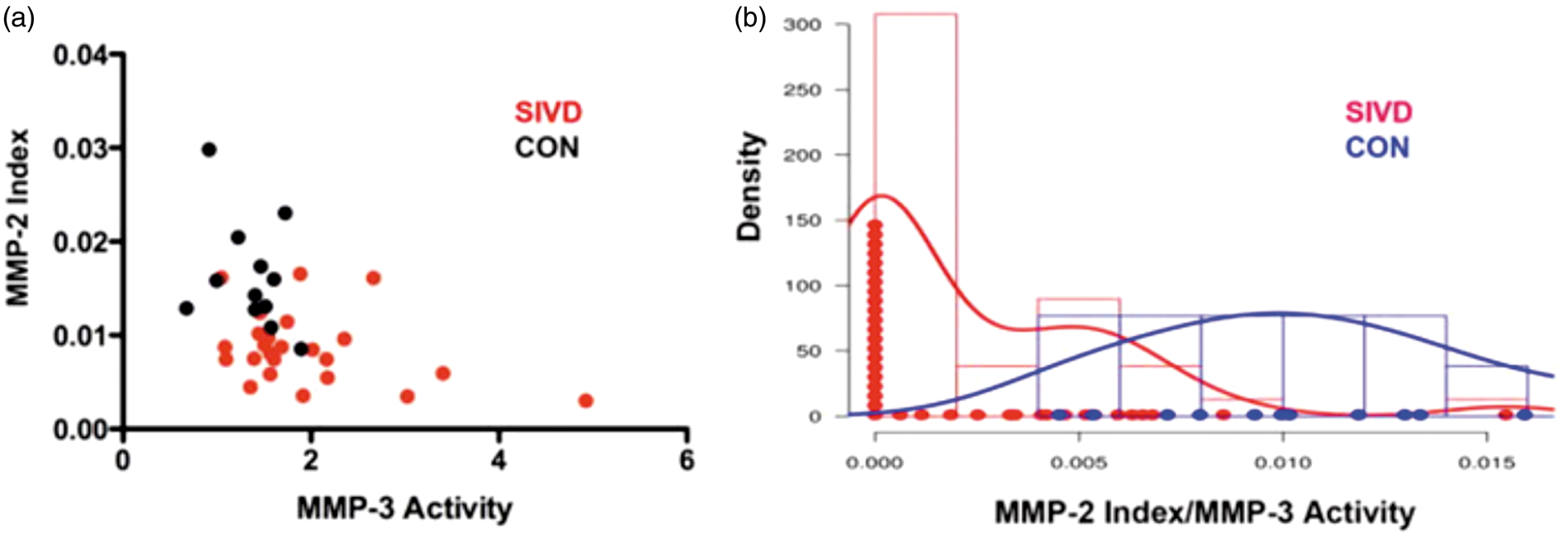
There are no validated blood biomarkers for BD. However, studies using blood have indicated that a systemic low-grade inflammation leading to endothelial dysfunction is involved in SVD pathophysiology. Several blood-derived biomarkers have been studied, including C-reactive protein, interleukin-6 (IL-6), Intracellular adhesion molecule-1, and thrombomodulin. Interleukin-6 appears to be strongly associated with silent infarctions.108,109 Intracellular adhesion molecule-1 was elevated in patients with lacunar stroke and leukoaraiosis, 110 and in a prospective community-based study predicted progression of WMHs. 111 Homocysteine, which has been shown to cause endothelial dysfunction, was elevated in patients with lacunar stroke and leukoaraiois, and this association was attenuated after controlling for circulating markers of endothelial activation suggesting it was mediated via endothelial dysfunction.
Amyloid
Animal models of small vessel disease to identify drug targets
Several animal models have been developed to study VCI.114,115 The heterogeneity of the disease necessitates a variety of animal models to encompass the multiple causes. Most animal studies are based on either hypoxic hypoperfusion secondary to bilateral carotid artery occlusion in normotensive rats or SVD secondary to hypertension in the spontaneously hypertensive/stroke prone rat (SHR/SP).69,116
Bilateral Carotid Artery Occlusion
Bilateral carotid artery occlusion (BCAO) produces hypoxic hypoperfusion, which primarily affects the deep white matter. 117 The tissue is assumed to be hypoxic although direct measurements of tissue oxygen levels have not been made. White matter shows demyelination with breakdown of the BBB; MMPs are expressed in the hypoxic tissue and contribute to the myelin damage.118,119 In addition to the white matter there is cellular damage in the hippocampus. Cerebral blood flow is reduced in white matter, hippocampus, and some areas of the cortex shortly after the vessels are occluded; there is restoration of CBF over time. A drawback of the BCAO model is that the changes in the CBF occur acutely and resolve chronically. To overcome this limitation, gradual occlusion of the carotids with a device that constricts over time has been used. Gradual narrowing of the both common carotid arteries using the ameroid constrictor device instead of ligation circumvents the acute phase of CBF reduction and acute inflammatory response observed in the BCAO model. 120
Spontaneously Hypertensive/Stroke Prone Rats
Spontaneously Hypertensive/Stroke Prone rats develop pathologic changes that resemble those in SVD. 121 Bred originally from Wistar-Kyoto rats, they evolved into a hypertensive species and finally into the current SHR/SP. 122 Without modifications SHR/SP generally live for over 1 year, developing strokes and intracerebral bleeding before death. In addition to a diffuse brain SVD that closely mimics human sporadic SVD, they have damaged blood vessels in the kidneys.
Dietary modifications with high salt or low protein diets (Japanese Permissive Diet) accelerate the pathologic changes. 123 Recently, occlusion of one carotid artery to increase the hypoxic injury was added to the Japanese permissive diet in the SHR/SP animals. 124 Depending on the purpose of the study, various modifications can be made. For example, in studies involving intracerebral hemorrhage, the high salt or Japanese Permissive diet is introduced at age 6 weeks, which is 4 weeks before the onset of severe hypertension; this results in hemorrhages around 6 to 8 weeks later. If the dietary changes are delayed until the twelfth week, then there are prominent changes in the white matter that resemble those seen in BD and aging.
Both BCAO in the normotensive rats, and low protein, high salt diets with unilateral carotid artery occlusion in the SHR/SP, damage neurons and white matter through hypoxic hypoperfusion. Measurements of the level of oxygen in the white matter over an extended period of time have been performed using the minimally invasive technique of electron paramagnetic resonance. 125 The oxygen content in the white matter begins to gradually increase by the nineth week reaching a maximum at 12 weeks after birth. After unilateral carotid artery occlusion and abnormal diet, which are started at 12 weeks, the oxygen content in the white matter falls precipitously to hypoxic levels where it remains until the animal dies around week 16. Therapeutic manipulations with BBB-directed strategies, such as with activated protein C analogs eliminated postischemic microbleeds in SHR, suggesting that enhancing BBB integrity might have beneficial in ischemic model in SHR. 126
Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy Mouse Models
Transgenic mice expressing mutated NOTCH3 protein in the ECD recapitulate the preclinical stage of the disease with NOTCH3ECD and granular osmiophilic material deposits and white-matter lesions. 127 Vascular accumulation of NOTCH3ECD is the earliest pathologic change, a finding, which was suspected from the immunohistochemical analysis of skin biopsies from asymptomatic NOTCH3 mutation carriers.127,128 Mutant mice have a lower threshold for cortical spreading depression, which could explain the higher incidence of migraine with aura in CADASIL patients. 129 Also, mutant mice have impaired cerebrovascular reactivity, with reduced functional hyperemia and compromised autoregulation of CBF. Myogenic responses have a major role in normal hemodynamic processes in the brain, modulating vascular resistance and contributing to local and global CBF regulation. Notably, analysis of isolated vessels have showed reduced myogenic responses in both pial and parenchymal arteries in mutant mice, a finding that could account for the impaired cerebrovascular reactivity in these mice. 130 Importantly, the data indicate that cerebral arteries are dysfunctional in the absence of overt smooth muscle degeneration and fibrosis, and that cerebrovascular dysfunction is detectable before the appearance of white-matter lesions, suggesting that the former could cause the latter. 130
Treatments in Animal Models
The optimal model to use for testing of drugs will vary with the pathologic process suspected. In the hypertensive vascular disease of the elderly, SHR/SP is best. In normotensive rats, BCAO can be used as a model to study inflammatory mechanisms. For hereditary forms of SVD, mouse models with specific genes will be needed. Treatments in rats with hypoxic hypoperfusion due to either BCAO or spontaneous hypertension have indicated a number of potential therapeutic agents.114,131 Cyclosporin A suppressed both glial activation and white-matter changes after chronic cerebral hypoperfusion, suggesting that immunologic reaction may have a role in the pathogenesis of the white-matter changes. 132 Cyclosporine A inhibits BBB breakdown in APOE4 Tg mice by inihibiting cyclophilin A-MMP-9 pathway in pericytes leading to reversal of neuronal dysfunction and secondary neurodegenerative changes. 133 A number of anti-inflammatory agents and free radical scavenging agents have shown benefit. 114 Treatments with minocycline significantly attenuated the hypoxia-ischemia-induced brain injury and improved neurobehavioral performance; the protection of minocycline was associated with its ability to reduce microglial activation. 134 In the SHR/SP with the Japanese permissive diet and unilateral carotid artery occlusion, treatment with minocycline blocked the full development of white-matter injuries seen on MRI and improved behavior in the Morris water maze. 135
Based on mouse models of CADASIL, targeting the synthesis of NOTCH3 or the clearance of NOTCH3ECD deposits, might represent a first therapeutic option. 136 Upregulation of Kv1 channels in cerebral arteries has been shown to be the molecular mechanism underlying the diminished myogenic responses in mutant mice. 137 Treatment of hypertension and other vascular risk factors, anti-aggregants, and anti-inflammatory drugs are other possible avenues.
Multimodal approach to biomarkers in vascular cognitive impairment diagnosis
Multiple pathologic processes produce the final changes in the brains of patients with VCI. Depending on the time of encountering the patient, there may be one or more pathologies present. Autopsy is of less use in VCI since by the time of death the majority of patients have a variety of diseases, ranging from cerebral infarctions to AD.6,138 A more practical approach based on the need to identify the initiating factors in a multiple disease process is to use biomarkers that would ideally reflect the brain pathology in the early stages of the disease. 139 Since the natural history can be determined in BD, this is most likely the optimal form to use biomarkers to separate from other forms for the purpose of treatment trials.
Although there are a number of potential disease markers from the clinical, imaging, and biochemical perspective, none of them is diagnostic, making it necessary to use a combination of these markers. 140 Biomarkers derived from MRI are the best studied with growth of both WMHs on FLAIR and FA decrease on DTI, indicating progressive damage. 141 Information on the use of a number of biomarkers of diagnosis of BD is available, but most have not been used in longitudual studies. For diagnosis, there are studies showing that clinical and neuropsychological testing, 1H-MRS, and CSF measurements of albumin, MMPs, and neurofilament light can be used. It is possible to create a diagnostic scale by summing a series of biomarkers, which when a given number of factors are present, the likelihood of the diagnosis being BD is increased. A statistical approach can be used to optimize the diagnostic set through use of exploratory factor analysis. Two processes are involved: initially, diagnostic biomarkers need to be determined, and secondarily, the biomarkers that can be followed to show progressive tissue damage need to be selected. Biomarkers to be used in diagnosis should be obtained at the early stages with the diagnoses confirmed after a period of follow-up.
A potential multimodal approach would include three groups of possible markers: clinical, imaging, and biochemical, which are like three axes with grades of closeness to the full diagnosis of BD at points along each axis. Clinical factors come from the neurologic examination and the neuropsychological testing: features from the examination include vascular risk factors, hyperreflexia, and gait impairment; neuropsychological testing includes impaired executive function with relative preservation of memory and language; imaging features based primarily on MRI include reduced NAA on 1H-MRS, increased BBB permeability with DCEMRI, reduced FA and increased mean diffusivity on DTI. Cerebrospinal fluid measures include increased albumin ratio, reduced MMP-2 index, elevated neurofilament light, and the absence of AD biomarkers. A complicating factor is that there is considerable overlap between AD and VCI, which is not always be possible to document by clinical or imaging means alone. 54
Identifying an optimal set of markers will be challenging since different investigators may have access to a limited number of the possible biomarkers. It may be necessary to have a ‘high tech’ set of markers done by a limited number of investigators with the goal of selecting optimal ones, and a ‘low tech’ group of markers that are available at all research sites. Additional factors such as age will need to be taken into consideration.
An approach to targeted treatment trials
Treatment trials in VCI have used drugs designed to treat AD with limited success in heterogeneous populations. 11 Treating vascular risk factors by aggressively lowering blood pressure, controlling diabetes, reducing hyperlipidemia, and encouraging exercise should be performed in all VCI patients. The BD subpopulation of VCI patients with white-matter injury related to hypoxic hypoperfusion has inflammation, which could be targeted for treatment along with vascular risk factors. A recent epidemiologic study in the cohort of participants in the third generation of the Framingham Study showed that hypertension begins to cause white-matter damage in middle age, supporting aggressive treatment of hypertension in mid-life. 142 This has lead to a reassessment of the normal range of blood pressure at various ages since it may be beneficial to aggressively lower blood pressure in the younger hypertensive patients, while avoiding excessive blood pressure lowering in the very old, although the age boundaries are still to be determined. 143
While it remains a challenge to separate inflammation from multiple lacunar strokes as the primary mechanism of injury to the white matter, the interaction between ischemia and Inflammation is an emerging concept that may be relevant in those individuals with progressive decline rather than discreet strokes. 144 It is likely that the extensive white-matter injury evolves from small strokes that trigger either an inflammatory response around the vessels or an inflammatory response is initiated in the vessels damaged by hypertension or diabetes. Since the disruption of the BBB suggests inflammation, reducing permeability may be beneficial and could be tested. Although the inflammatory cascade causes damage in the early stages of an injury, in the secondary stage when recovery with angiogenesis is beginning, inflammation appears to be necessary for recovery, which could compromise treatment with anti-inflammatory agents. These studies have been performed in the acute injury models and they need to be performed in the chronic injury models to determine the long-term effects of agents that block inflammation.
A major challenge will be to identify the optimal biomarkers both for diagnosis and for surrogate endpoints for treatment trials. Rather than attempt to categorize patients solely on the basis of one diagnostic test, developing operational definitions based on combinations of features may help. This requires understanding the contribution of each of the factors to the clinical presentation. For example, in the clinical examination it is well known that motor findings are uncommon in the early stages of AD, where memory loss and language problems are the dominant factors. However, motor findings such as hemiparesis and asymmetric hyperreflexia can be frequently present at the onset in SVD. Similarly, executive dysfunction occurs early in SVD. Confluent WMHs on MRI are highly suggestive of BD, although it can be seen in AD and normal elderly. Biochemical measurements of NAA with 1H-MRS are more specific for ischemic damage to the white matter, and DTI provides a more sensitive measure of white-matter damage than FLAIR or T2-weighted images. DTI has the advantage that it can be performed in a shorter time and is readily available on most MRI machines. Currently, confluent WMHs are the only MRI correlates of cerebral SVD for which the requirement of a surrogate marker is fulfilled; progression of confluent white-matter lesions correlates with cognitive decline.13,147 Amyloid and tau imaging with positron emission tomography could also be helpful to diagnose comorbidity with AD in the patients with mixed disease, 145 with the caveat that amyloid deposits can also be present in cognitively normal individuals. 146
Biochemical CSF studies provide the third axis of diagnosis; elevated albumin ratio indicates that the BBB is compromised, which is more likely to occur in SVD than in AD. Furthermore, CSF shows changes in proteins associated with AD, including A
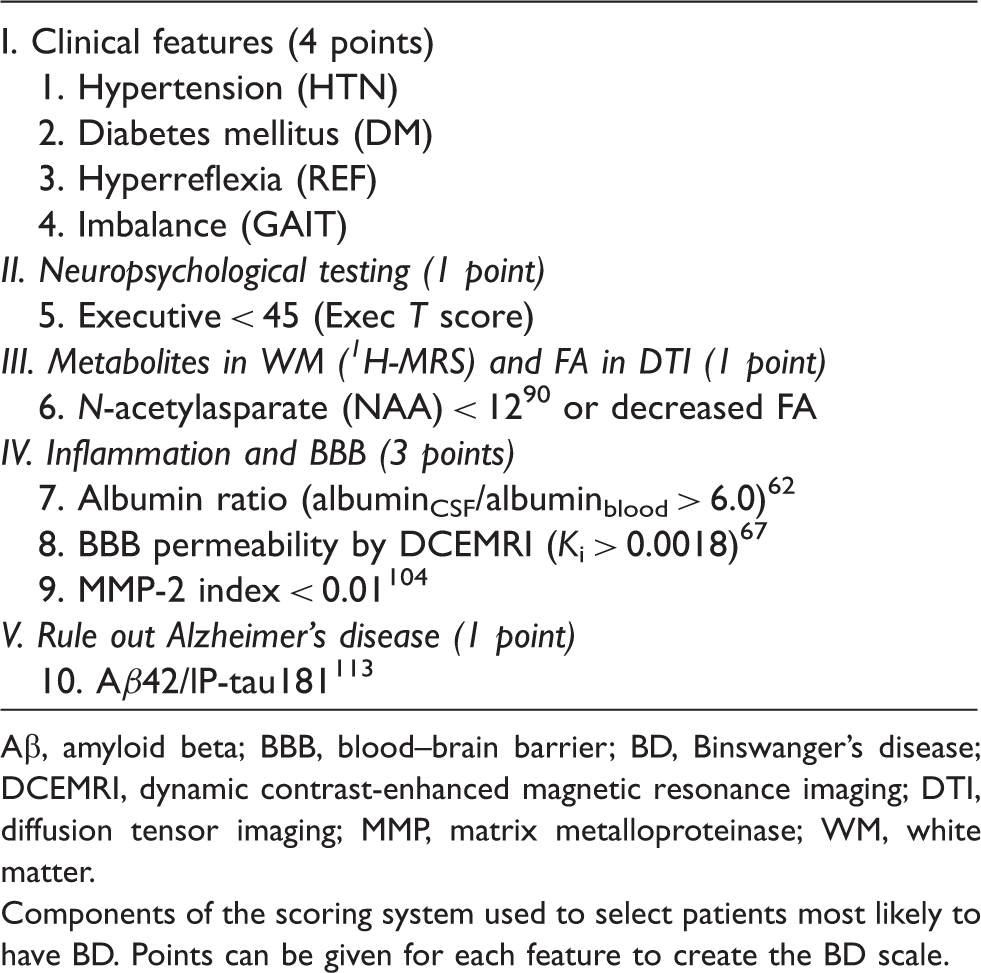
Discreet cut-points for the factors used to diagnose BD are difficult to determine since it is a spectrum disorder with AD at one end and BD at the other, and a large group of patients with overlapping disease in the middle (Figure 6). Utilizing a combination of these factors it is possible to construct scales that reflect the underlying pathophysiologic changes occurring in the brain. One such scale is shown in Table 4, which is based on a single center study, using cut-points that have been determined in studies of individual factors in patients and controls. High or low scores on these scales would suggest the ‘pure’ forms, while intermediate scores would indicate ‘mixed’ pathologic processes. Furthermore, since these biomarkers are dynamic and change at different stages of the disease, it would be possible to stage the disease process and modify treatments based on the stage.
148
The spectrum nature of Binswanger’s disease (BD) is illustrated. At one end of the spectrum on the left side is Alzheimer’s disease with high levels of amyloid and tau proteins. At the other end (right) is BD with vascular risk factors and without amyloid and tau. In the middle are the mixed dementia patients, which represent the majority of the patients with relative levels of pathology of both diseases. Potential biomarkers and other features to create BD scale for diagnosis. Aβ, amyloid beta; BBB, blood–brain barrier; BD, Binswanger’s disease; DCEMRI, dynamic contrast-enhanced magnetic resonance imaging; DTI, diffusion tensor imaging; MMP, matrix metalloproteinase; WM, white matter. Components of the scoring system used to select patients most likely to have BD. Points can be given for each feature to create the BD scale.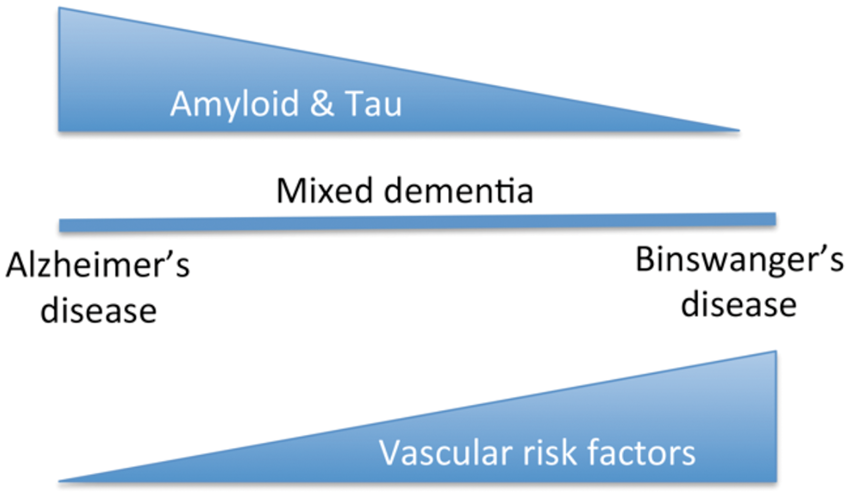
Clarification of the optimal factors to include in classification scales would require a concerted effort of multiple centers and a harmonization of the data collection methods. 149 Such large data sets could be mined statistically to identify best classification features. An even more important exercise for such an endeavor to succeed would require agreement as to diagnoses. These would have to be made after several years of follow-up at each center based on the clinical picture. Using this iterative approach, it would be possible to construct retrospective databases that then could be used prospectively to identify patients for targeted treatment trials.
Recommendations for future directions
Treatment trials in animal models can help identify agents to test in patients. Ideally, the drugs to be tested would show benefits in several models and both sexes as now required for acute drug studies in stroke. 150 Drugs that have been approved for other uses, for example, the anti-inflammatory agents and free radical scavengers, minocycline and simvastatin, all of which have been shown to have beneficial effects in animals models and could be tested in humans.151,152 A biologic product, E-selectin, has been shown to reduce inflammation after induction of nasal tolerance in the hypertensive rat. 153 Reliable end points will need to be established. For example, quantification of BBB permeability could show reduction in short-term studies of several months. Reduction in the rate of growth of WMHs by DTI could show improvement in 6 to 12 months. Slowing the rate of cognitive decline may require 2 to 3 years. The addition of neuropathologic studies will help confirm diagnoses. This is an ambitious project that requires identification of homogeneous populations with biomarkers, development of potential drugs in appropriate animal models, and establishment of consortium of investigators to test promising agents, using agreed upon end points. Such a procedure has recently been suggested for amyloid angiopathy and could be applied to BD. 154
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.