
Abstract
Individualized stroke treatment decisions can be improved by accurate identification of the extent of salvageable tissue. Magnetic resonance imaging (MRI)-based approaches, including measurement of a ‘perfusion-diffusion mismatch’ and calculation of infarction probability, allow assessment of tissue-at-risk;however, the ability to explicitly depict potentially salvageable tissue remains uncertain. In this study, five predictive algorithms (generalized linear model (GLM), generalized additive model, support vector machine, adaptive boosting, and random forest) were tested in their potency to depict acute cerebral ischemic tissue that can recover after reperfusion. Acute T2-, diffusion-, and perfusion-weighted MRI, and follow-up T2 maps were collected from rats subjected to right-sided middle cerebral artery occlusion without subsequent reperfusion, for training of algorithms (Group I), and with spontaneous (Group II) or thrombolysis-induced reperfusion (Group III), to determine infarction probability-based viability thresholds and prediction accuracies. The infarction probability difference between irreversible—i.e., infarcted after reperfusion— and salvageable tissue injury—i.e., noninfarcted after reperfusion—was largest for GLM (20 ± 7%) with highest accuracy of risk-based identification of acutely ischemic tissue that could recover on subsequent reperfusion (Dice's similarity index = 0.79 ± 0.14). Our study shows that assessment of the heterogeneity of infarction probability with MRI-based algorithms enables estimation of the extent of potentially salvageable tissue after acute ischemic stroke.
Keywords
INTRODUCTION
Contemporary treatment protocols for patients suffering from acute ischemic stroke ask for adequate and early identification of tissue at risk of infarction to allow for proper clinical decision making. Current thrombolytic treatment guidelines indicate safe treatment time windows of 3 to 4.5 hours after stroke onset. 1 However, this time window may be too strict in particular cases, unnecessarily excluding patients who may benefit from reperfusion therapy. 2
Neuroimaging, particularly with magnetic resonance imaging (MRI), provides a powerful tool for characterization of acute cerebral ischemic tissue status, which can aid in treatment decision making in individual patients. 3 In particular, diffusion-weighted imaging, for detection of acute ischemic tissue damage, 4 and perfusion-weighted imaging, for detection of hemodynamic disturbances, 5 provide sensitive and specific means for acute stroke diagnosis. Dichotomization of MRI-derived perfusion- and diffusion-based lesion volumes into overlapping and nonoverlapping areas enables selection of patients with a ‘perfusion-diffusion mismatch’ who may be eligible for thrombolytic treatment.2,6,7 However, lack of standard postprocessing procedures and threshold values may compromise robust characterization of a ‘perfusion-diffusion mismatch',3,8 and volumetric analysis may obscure and oversimplify the complex and heterogeneous status of the affected tissue.7,9,10 This mismatch area may therefore overestimate the actual tissue area at risk,5,11,12 as well as exclude injured tissue that is potentially salvageable. 13
The complex relation between multiple pathophysiologic factors involved in stroke lesion progression may be better caught and described using multiparametric imaging-based statistical algorithms. These algorithms allow voxelwise integration of multiple MRI-based tissue and perfusion parameters to compute a single quantitative probabilistic index.14,15 Multiparametric algorithms can more accurately estimate risk of infarction compared with single MRI-based parameters, and show good correspondence with actual lesion outcome.14,16 However, it is unclear whether such algorithms also enable accurate differentiation between irreversibly damaged and potentially salvageable tissue, which would significantly advance the value of this approach for selection and planning of therapeutic intervention.12,17
We hypothesized that acute imaging-based predicted infarction areas can be subdivided into volumes of irreversible and reversible tissue injury. Hence, we selected five well-established predictive algorithms and determined each algorithm's efficacy in (1) early detection of tissue at risk of infarction and (2) differentiating irreversibly damaged tissue from potentially salvageable tissue, based on multiparametric MRI data after experimental stroke. To that aim, we compared early measures of infarction risk with final outcome after ischemic stroke in rats with or without subsequent reperfusion.
MATERIALS AND METHODS
Animal Procedures
We partly included data from animals that have been previously used for another study. 18 The current study provides new and original results that have not been described in our previous study. Animal procedures were conducted according to the guidelines of the European Communities Council Directive and approved by the Ethical Committee on Animal Experiments of the University Medical Center Utrecht and Utrecht University. Surgical procedures have been described in detail elsewhere.18,19 In brief, before surgery male Wistar rats (275 to 400 g, Harlan, Horst, The Netherlands) received an intramuscular injection of gentamicin sulfate (5 mg/kg) as antibiotic treatment, and 2.5 mL glucose-saline solution to prevent dehydration. Subsequently, animals were anesthetized by a subcutaneous injection of 0.5 mL/kg fentanyl citrate (0.315 mg/mL) and fluanisone 10 mg/mL (Group I), or by mechanical ventilation with 2% isoflurane in air to O2 (7:1) (Groups II and III). Body temperature was maintained at 37.5 (±0.5)1C with a temperature-controlled heating pad. The right carotid artery was exposed by a ventral incision in the neck. A modified catheter was advanced into the internal carotid artery, until the tip was proximal to the middle cerebral artery (MCA). Unilateral MCA occlusion was induced by insertion of an intraluminal filament (Group I) (1), or by slow injection of a homologous blood clot (50 mm long, 24-hour old) (Groups II and III). Subsequently, the wound was closed and animals received a subcutaneous injection of buprenorphine (0.03 mg/kg) for pain relief, and 5 mL glucose-saline solution to compensate for loss of water and minerals. In the first three days after surgery, excessive weight loss was partially compensated by subcutaneous injection of Ringer's lactate solution (0 to 10 mL, depending on degree of weight loss). Within 30 minutes after MCA occlusion (MCAo), animals were positioned in the MR scanner, and acute imaging was conducted between 0.5 and 2 hours after stroke. Immediately after the first imaging session, Group II and III animals received saline (Group II) or 10.0 mg/kg recombinant tissue plasminogen activator (rt-PA; Actilyse, Boehringer Ingelheim, Alkmaar, The Netherlands, 3.0 mg/mL) (Group III), intravenously administered over a 30-minute period (10% bolus injection; 90% continuous infusion). Animals were allowed to recover afterwards. Group I animals underwent a second MRI session at 72 hours after onset, whereas for Group II and III animals MRI was repeated at 24 hours after MCAo to confirm reperfusion and 168 hours to establish actual tissue injury.
In Group I, 7 out of 14 rats with an acute lesion in the MCA territory survived up to 3 days to undergo the second MRI session. In Groups II and III, survival rate after successful MCAo was higher: 7 out of 9 animals in Group II and 5 out of 7 animals in Group III survived up to day 7. This led to the following sample sizes for the present study: Group I:
Image Acquisition
Magnetic resonance imaging was conducted on a 4.7-T scanner (Varian, Palo Alto, CA, USA). Group I animals underwent MRI—with a 9.0-cm inductively coupled Helmholtz coil for signal transmission and detection—at 0.5 to 2 hours and at 72 hours after MCAo. For each session, MRI consisted of T2-weighted spin echo (repetition time (TR) = 3,000 ms; echo time (TE) = 17.5 ms; number of echoes = 8; data matrix = 128 × 128 × 11; field-of-view (FOV) = 25 × 25 × 13.2 mm
3
; 0.13 mm interslice gap), diffusion-weighted multislice echo planar imaging (TR = 2,000 ms; TE = 80 ms; data matrix = 128 × 128 × 11, FOV = 25 × 25 × 1.2 mm
3
; 0.13 mm interslice gap;
Group II and III animals underwent MRI with an updated protocol—using a 9.0-cm inductively coupled Helmholtz coil and an inductively coupled 2.5-cm surface coil for signal detection, respectively—at 0.5 to 2, 24, and 168 hours after MCAo. Magnetic resonance imaging consisted of T2-weighted spin echo (TR = 3,600 ms; TE = 15 ms; number of echoes = 12; data matrix = 256 × 128 × 19; FOV = 32 × 32 × 19mm
3
), diffusion-weighted 8-shot echo planar imaging (TR = 3,500 ms; TE = 38.5 ms;
Image Processing
Parametric maps of the
Tissue Outcome Prediction
To predict poststroke tissue infarction, we used predictive algorithms that combine a carefully balanced set of acutely acquired MRI parameters (
Generalized linear model, GAM, and SVM estimate
In contrast to GLM, GAM, and SVM, which define a single effective classification function,
Details on operational parameter optimization of the algorithms can be found in Supplementary Data.
Each algorithms’ prediction accuracy was determined in Group I with a jack-knifing (i.e., leave-one-out) approach to prevent bias.
33
Predictions in Group II and III were based on aggregated data from Group I-trained models. Prediction accuracy was assessed by comparing the estimated infarction probability to the follow-up
Differentiation Between Irreversibly Damaged and Potentially Salvageable Tissue
Group II and III animals were then used to differentiate between irreversibly damaged tissue, and tissue at risk of infarction that could be saved on reperfusion. Therefore, acute infarction risk maps were further partitioned into (1) normal appearing tissue (acute infarction probability <50%); (2) irreversibly damaged tissue (acute infarction probability >50% and tissue abnormality at follow-up stage); and (3) potentially salvageable tissue at risk (acute infarction probability > 50% and normal tissue appearance at follow-up stage). The infarction probability threshold that optimally separated potentially salvageable from irreversibly damaged tissue was determined by calculating interclass and intraclass infarction probability variance at probability values between 1% and 100%. Optimal differentiation was considered at the threshold for which interclass and intraclass variances were highest and lowest, respectively. 36 The derived threshold was then applied to assess the overlap (with DSI) of: acutely predicted irreversibly damaged tissue and infarction at follow-up (i.e., TP); acutely predicted irreversibly damaged tissue and salvaged tissue at follow-up (i.e., FP); acutely predicted potentially salvageable tissue and normal appearing tissue at follow-up (i.e., TN); and acutely predicted potentially salvageable tissue and infarction at follow-up (i.e., FN).
Statistical Analysis
Mean predicted infarction risk for each algorithm was compared using repeated measures ANOVA with
RESULTS
Acute and Follow-Up Lesion Volumes
Figure 1 shows lesion volumes, expressed as hemispheric lesion fraction (HLFs), calculated from acute diffusion, acute perfusion, and follow-up T2 MRI. In the acute phase, diffusion- and perfusion-based lesion volumes were not statistically different between groups; at follow-up, however, infarct volumes in Group I (permanent filament MCAo; day 3) were significantly larger than those in Groups II and III (embolic MCAo with reperfusion; day 7). All groups showed a significantly smaller acute diffusion-based lesion volume as compared with the volume of acute perfusion loss, i.e., ‘perfusion-diffusion mismatch'. Follow-up T2-based lesion volume was comparable to the acute perfusion-based lesion volume in Group I, and to the acute diffusion-based lesion volume in Groups II and III. Magnetic resonance imaging at 24 hours after stroke revealed that the tissue volume with perfusion abnormality had reduced by >40% in all but one (Group III) animal in Groups II and III, indicative of reperfusion.
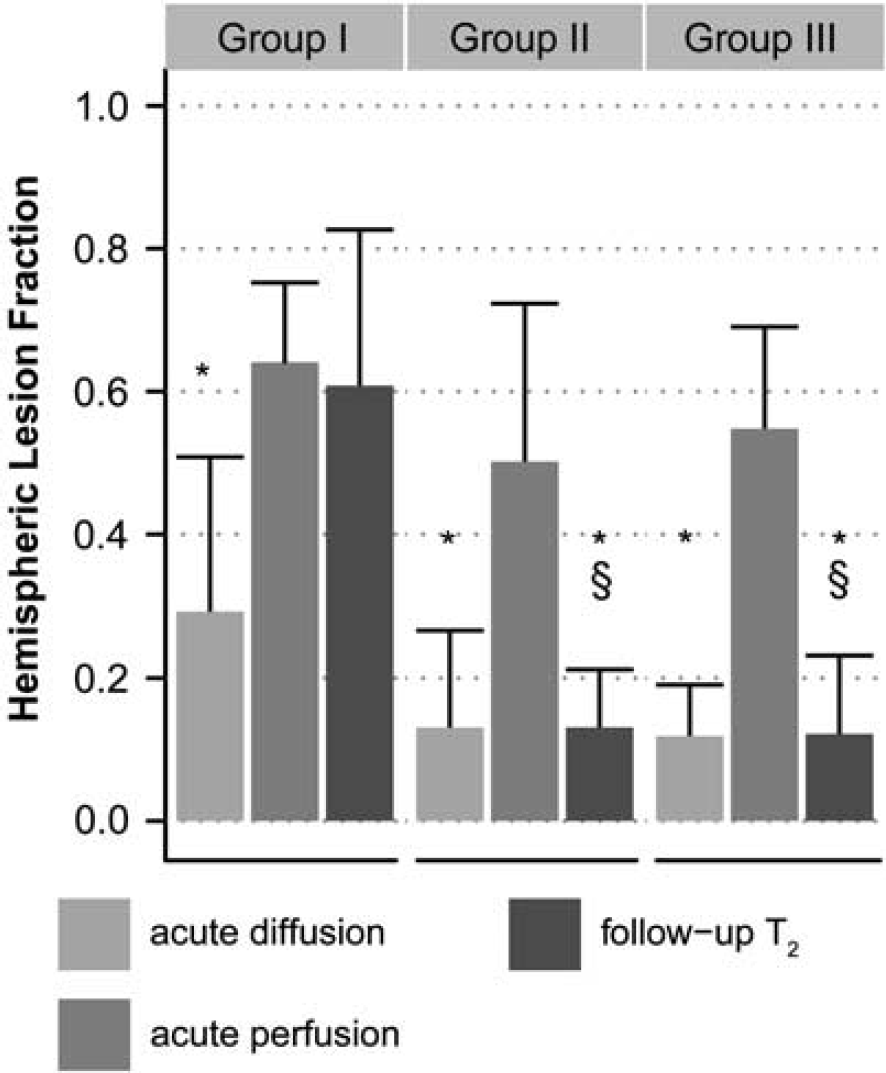
Hemispheric lesion fractions (HLFs) based on abnormal values on acute apparent diffusion coefficient (ADC) maps ('acute diffusion'), acute mean transit time (MTT) maps ('acute perfusion') and follow-up
Prediction of Infarction
The five predictive algorithms were trained with Group I data and subsequently applied to Group I, II, and III data. Figure 2 shows examples of resultant infarction probability maps in Group I, II, and III animals. Based on AUCroc, AUCpr, sensitivity, and specificity values, all algorithms predicted actual infarction approximately equally well in (training) Group I (Figure 3). The size of overlap between the 50% risk-thresholded predicted infarction and actual infarcts on follow-up was similar for all algorithms (mean DSI = 0.77 ± 0.11;
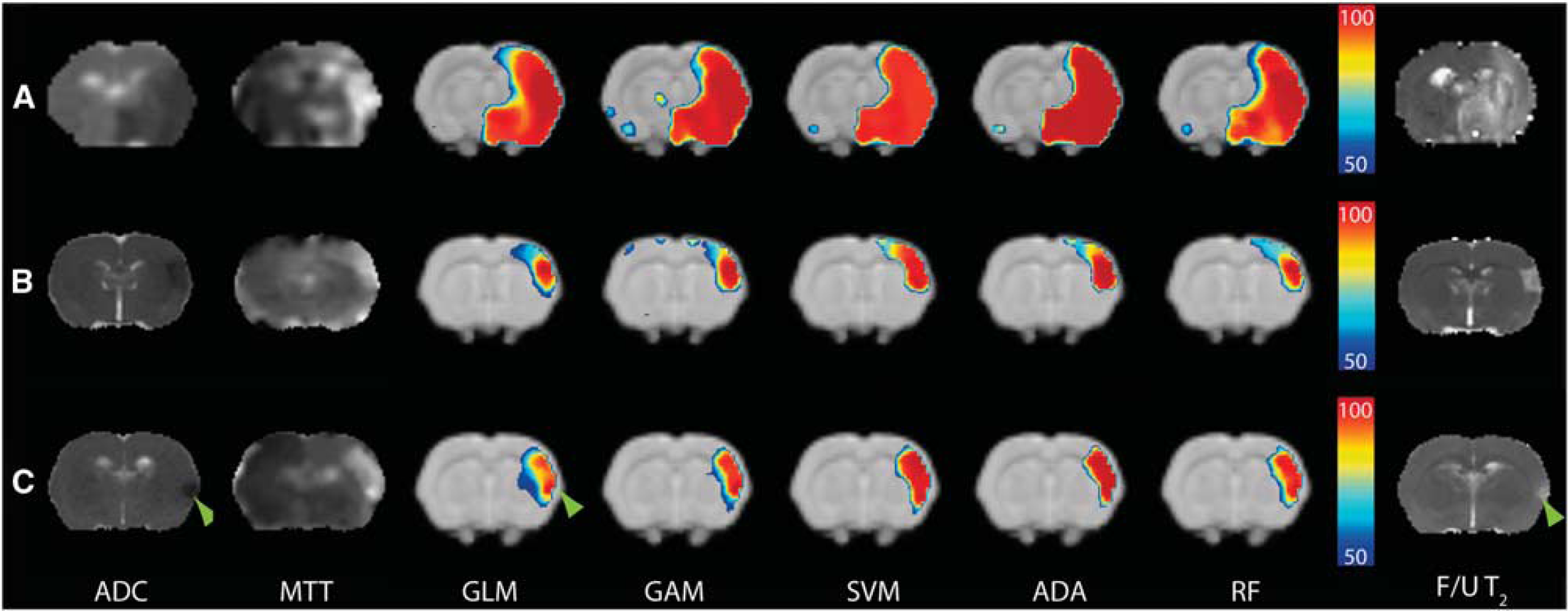
Coronal rat brain slices with acute diffusion (apparent diffusion coefficient (ADC) map; hypointensity) and perfusion abnormalities (mean transit time (MTT) map; hyperintensity) after permanent filament MCA occlusion (MCAo) (Group I) (
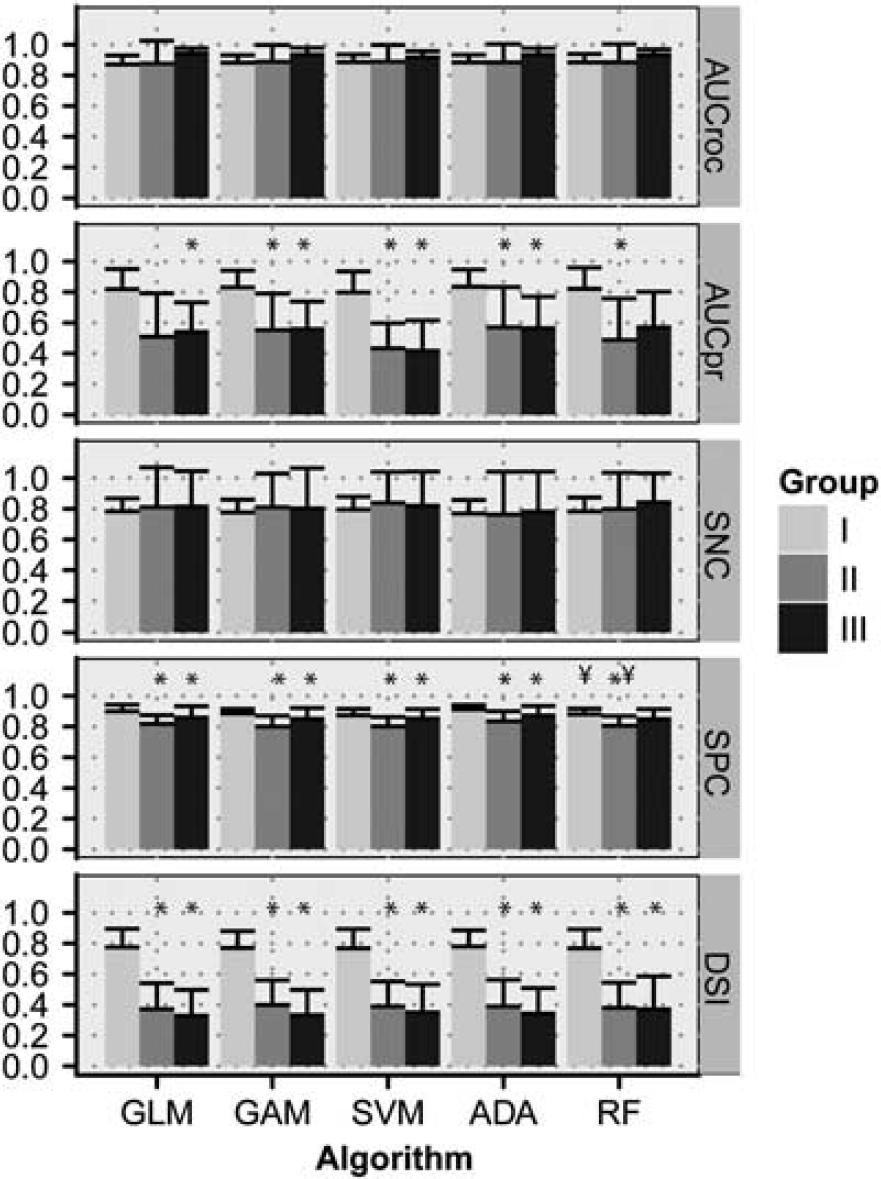
Performance measures of the predictive algorithms for Groups I, II, and III (mean + s.d.). AUCroc, area under the receiver operator characteristic (ROC) curve; AUCpr, area under the precision-recall (PR) curve; SNC, sensitivity; SpC, specificity; DSI, Dice's similarity index at a risk threshold of 50%; GLM, generalized linear model; GAM, generalized additive model; SVM, support vector machine; ADA, adaptive boosting; RF, random forest. *
Prediction accuracy in Groups II and III was similar for all algorithms. In contrast to Group I, however, the volumes of increased risk of infarction were significantly larger than follow-up infarct volumes in Groups II and III. This was reflected by significantly lower model specificity, AUCpr, and DSI in Groups II and III as compared with Group I (Figure 3).
Infarction probability values within the predicted infarction volume were significantly different between algorithms (Table 1), despite similarity in size of the predicted infarction (
Predicted hemispheric infarction fractions and infarction probability
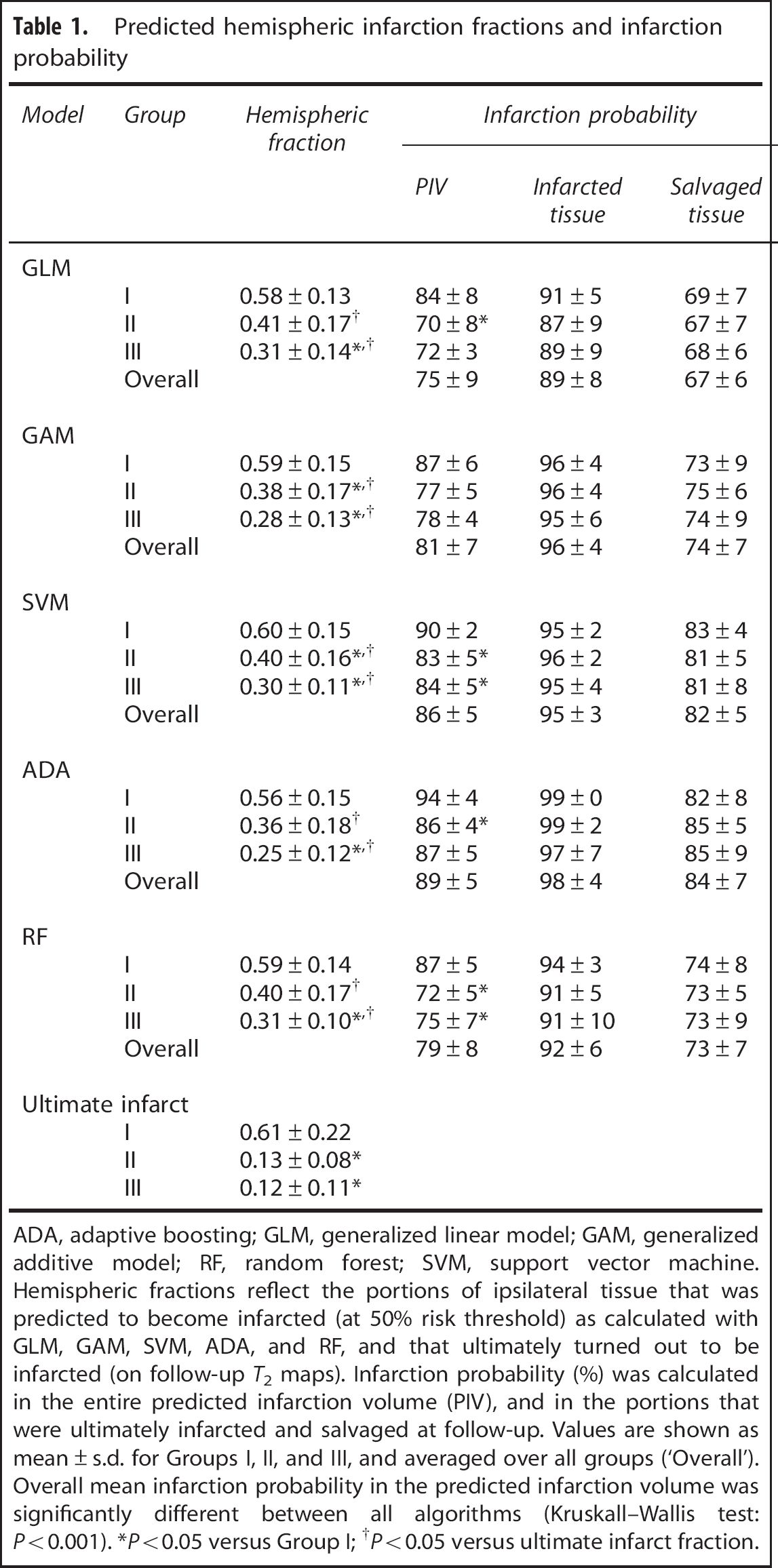
ADA, adaptive boosting; GLM, generalized linear model; GAM, generalized additive model; RF, random forest; SVM, support vector machine. Hemispheric fractions reflect the portions of ipsilateral tissue that was predicted to become infarcted (at 50% risk threshold) as calculated with GLM, GAM, SVM, ADA, and RF, and that ultimately turned out to be infarcted (on follow-up
Differentiation Between Irreversibly Damaged and Potentially Salvageable Tissue
Table 1 shows that infarction probabilities in the predicted infarction volume were lower in subsequently salvaged tissue as compared with ultimately infarcted tissue, which was most evident for GLM. Infarction probability profiles within the predicted infarction volumes were further categorized based on the smallest intraclass and largest interclass variance of areas that corresponded with eventually salvaged (FP) and eventually infarcted tissue (TP). Optimization yielded the lowest threshold for GLM (74 ± 1.0%,
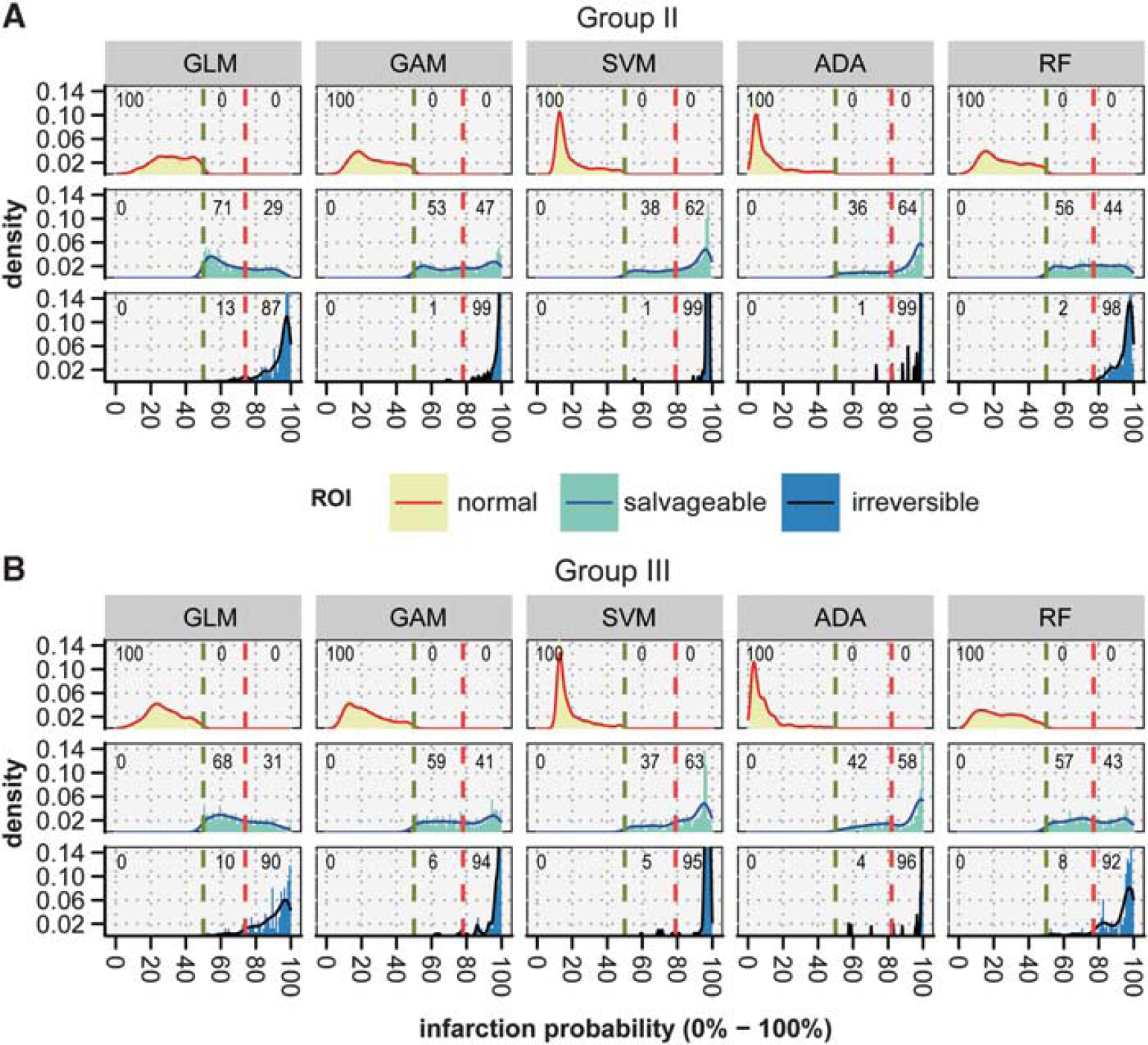
Density plots of acute infarction probabilities calculated with generalized linear model (GLM), generalized additive model (GAM), support vector machine (SVM), adaptive boosting (ADA), and random forest (RF) in Groups II (
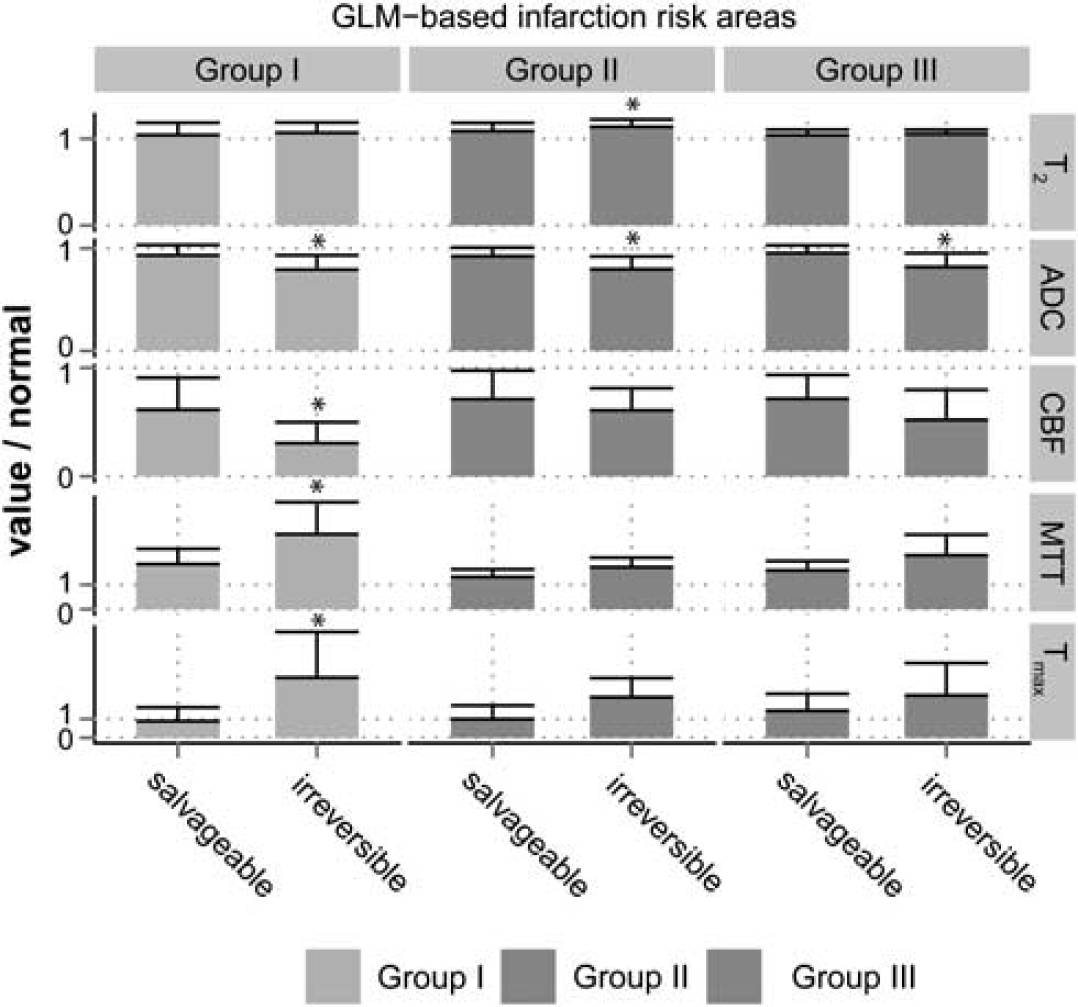
Relative
Figure 5 shows that in all groups, acute CBF, MTT, and
The overlap (expressed as DSI and depicted in Figure 6) between acutely predicted infarction volume and actual infarct volume at follow-up revealed that GLM and RF recognized potentially salvageable tissue best with highest overlap of predicted salvageable and actually salvaged tissue (TN), and lowest overlap of acutely predicted irreversibly damaged tissue but salvaged tissue at follow-up (FP). The TN DSI values for GLM and RF corresponded with the degree of overlap between the acute perfusion-diffusion mismatch volume and noninfarcted tissue at follow-up (DSI = 0.82 ± 0.12). The FN DSI values for GLM and RF were also comparable to DSI between the perfusion-diffusion mismatch and subsequently infarcted tissue (DSI = 0.05 ± 0.08).
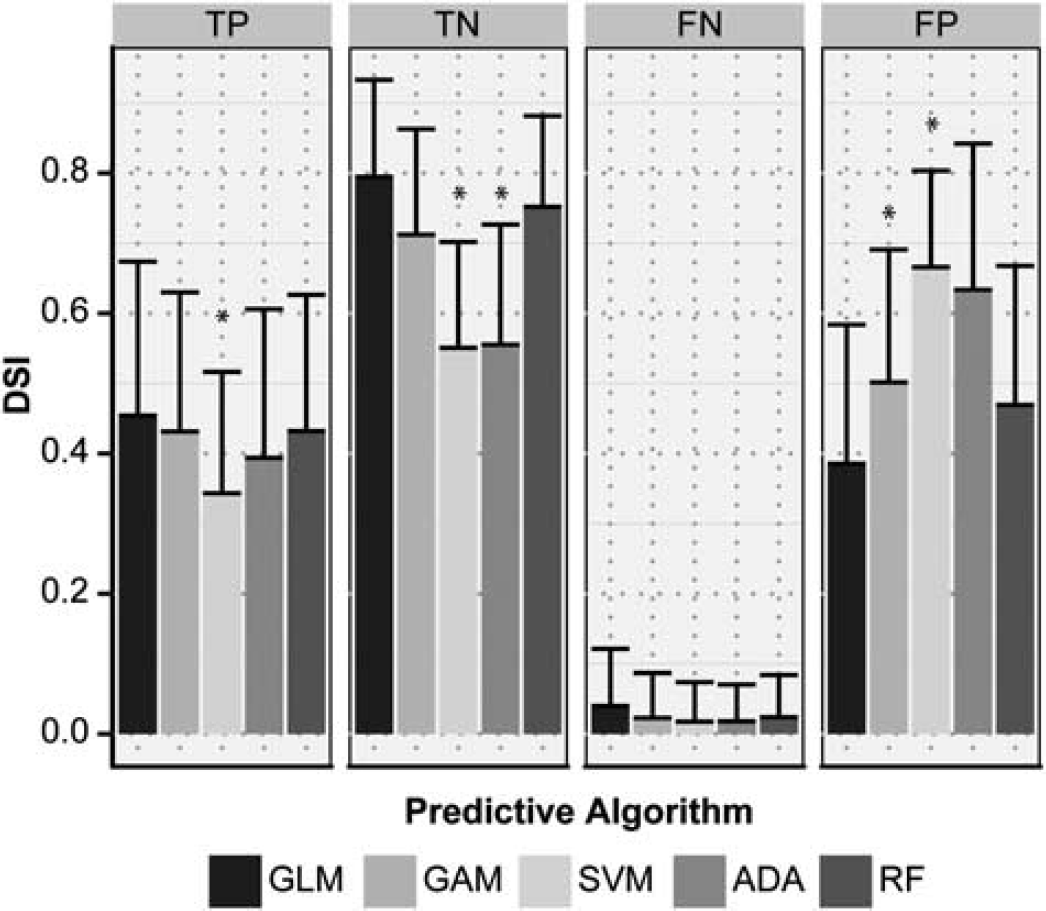
Overlap, expressed as Dice's similarity index (DSI), between volumes of acutely predicted tissue fate—i.e., irreversibly damaged or potentially salvageable—from the five predictive algorithms (generalized linear model (GLM), generalized additive model (GAM), support vector machine (SVM), adaptive boosting (ADA), random forest (RF)), and eventual outcome—i.e., infarction or salvaged—on follow-up scans. TP, true positive; FN, false negative; TN, true negative; FP, false positive. *
Support vector machine performed worst with lowest overlap for TN, and highest overlap of FP. Additionally, overlap of predicted irreversibly damaged and ultimate infarction at outcome (TP) was also lowest for SVM.
DISCUSSION
This study tested five different algorithms for early prediction of poststroke tissue outcome, by evaluating accuracy in predicting brain infarction, and efficacy in differentiating potentially salvageable tissue from irreversibly damaged tissue. All algorithms performed equally well in acutely predicting the extent of tissue that infarcted chronically after permanent filament MCAo in rats. In a rat model of embolic stroke with subsequent spontaneous or rt-PA-induced reperfusion, it was shown that differences in the distribution of acutely predicted infarction risk values, particularly with GLM and RF algorithms, could be exploited to differentiate salvageable tissue from irreversibly damaged tissue.
Previous predictive modeling studies have speculated on the use of differences in spatial distribution of calculated infarction probabilities as a tool for selecting stroke patients eligible for therapeutic intervention 12 and for estimating potential treatment responsiveness. 30 It has, for instance, been suggested that the level of predicted infarction risk provides insight in the likelihood of reperfusion. 30 Our data show that tissue salvageability on reperfusion is associated with the degree of infarction risk, which depends on the level of acute ischemic injury.
Algorithms were first trained in a model of permanent MCAo (Group I) to predict infarction when cerebral ischemia is sustained, i.e., without reperfusion that could reverse the progression of ischemic tissue injury. Animals in Groups II and III benefited from early spontaneous or rt-PA-induced reperfusion, which prevented lesion growth. Consequently, in contrast to Group I, follow-up infarctions were significantly smaller than the volume of acute perfusion loss. This allowed us to retrospectively identify potentially salvageable tissue from the acute MRI data set, which we compared against the calculated probability of infarction modeled in Group I, i.e., if reperfusion would have been absent. Although algorithms were not perfect in predicting the final infarct (DSI <1.0), for each algorithm the calculated infarction probability of tissue that indeed became infarcted, which was not significantly different between the three groups (Table 1), showing the sensitivity and specificity of infarction probability calculation on underlying tissue status, with relative independence on differences in stroke models (e.g., filament versus embolic MCAo), anesthesia (e.g., fentanyl citrate and fluanisone versus isoflurane), and MRI settings (e.g., small variations in imaging parameters). In all groups infarction probability values reflected the degree of acute ischemic injury, expressed by perfusion reduction (high probability of infarction was associated with lowered CBF, and prolonged MTT and
In earlier studies, the findings of different correlations between acute brain tissue ADC 37 or perfusion, 5 and subsequent infarction—reflective of the complex, heterogeneous and dynamic nature of stroke pathophysiology—have raised the question whether nonlinear relations of acute tissue status and eventual outcome can be sufficiently captured with linear algorithms like GLM.12,15,25 To that end, SVM and GAM have previously been introduced, and the current study adds ADA and RF, as potentially more effective models for nonlinear relationships.15,16
Our study shows that the level and distribution of calculated infarction probability values can differ significantly between these types of predictive algorithms. Where SVM and ADA provided relatively smooth infarction probability maps, the distribution of risk values was more heterogeneous with GLM, GAM, and RF. These differences may be related to the underlying method for discriminating infarcting from noninfarcting tissue. Regression models (GLM and GAM) and RF define a more direct relation of the training samples to the corresponding outcome. In ADA, and particularly in SVM, however, this relation is more indirect and aimed at iteratively optimizing the margin (dividing plane) that optimally separates infarcted from noninfarcted tissue in the training samples. 27 Furthermore, SVM, originally a binary classifier, requires an additional conversion step to obtain probabilistic values, which may impose less accurate approximation of probability. 27
Nevertheless, the lack of significant differences between linear and nonlinear algorithms in predicting the extent of infarction at follow-up, which is in line with previous studies in experimental settings 16 and in human patients, 38 challenges the advantage of complex (nonlinear) predictive algorithms for improved stroke outcome prediction. Our study suggests that the use of such algorithms may impose loss of additional information that could be of importance for further differentiation of heterogeneous tissue conditions. The distribution of infarction probabilities calculated with GLM, GAM, or RF was better linked to different tissue outcome, i.e., irreversibly damaged or salvaged. Nevertheless, it remains questionable whether any of these algorithms can fully capture the complexity of poststroke tissue dynamics within a single algorithm, particularly when timings of stroke onset and reperfusion vary. We speculate that multiple or hierarchically arranged algorithms, each describing a different aspect of tissue outcome, might provide improved prediction estimates.25,27 Careful selection of training data, 17 and incorporation of additional imaging or nonimaging biomarkers, such as tissue pH, 39 oxygen extraction fraction, 40 artery occlusion site, 41 or time after stroke onset may further contribute to voxel-based stroke outcome predictions without increasing diagnostic complexity. 25
In conclusion, we observed that different predictive algorithms are similarly effective in depicting tissue at risk of infarction. However, these algorithms had varying efficacy in differentiating between areas that were irreversibly damaged versus areas that could be salvaged after reperfusion. Our experimental stroke study allowed direct comparison between acute infarction predictions and ultimate tissue outcomes, and showed that multiparametric MRI-based predictive modeling—with GAM, RF, and particularly GLM algorithms—enables discrimination between irreversibly damaged and potentially salvageable tissue. These predictive models performed equally well in identifying tissue amenable to reperfusion as compared with the perfusion-diffusion mismatch model. Added value of the statistical algorithms is provided by the quantitative information on infarction probability on a voxelwise basis. Where assessment of tissue viability based on single indices and a single threshold is challenging (particularly in heterogeneous clinical settings), predictive algorithms give a quantitative likelihood of infarction or salvageability based on multiple parameters where each parameter describes a different aspect of the pathophysiologic condition. This may contribute to more confident treatment decision making and subsequent monitoring in the early stages of ischemic stroke. These predictive algorithms, which are readily applicable in preclinical and clinical settings, therefore provide promising means for treatment decision making and treatment efficacy monitoring after acute ischemic stroke.
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.