
Abstract
Ambient particulate matter (PM) pollution is estimated to be responsible for 3.2 million deaths annually worldwide. Although many studies have demonstrated PM as a serious risk factor for cardiovascular diseases, less is known on its association with cerebrovascular events. Over the last decade, however, an increasing number of studies have provided data showing a relationship between PM exposure and ischemic stroke (IS). In this article, we will report on existing epidemiologic findings for an association between PM exposure and IS based on a systemic literature search. Thus, despite inconsistencies in the results, currently available data suggest that PM exposure is a risk factor for IS, especially in patients with preexisting illnesses. With regards to the mechanisms leading to PM-dependent vascular damage, in particular proinflammatory, prooxidative, as well as proatherogenic pathways have been suggested to be involved. Notably, to date there is only one study published, which demonstrates the influence of PM exposure on cerebrovascular function. We will discuss reasonable approaches for future neurovascular research in this field.
INTRODUCTION
Air pollution is a heterogeneous mixture of gases, liquids, and solid particles, which all may be hazardous to health. Its main constituents, along with particulate matter (PM), are nitric oxides (NOx), sulfur oxides (SO2), carbon monoxide (CO), and ozone (O3). However, many epidemiologic studies have shown that in particular, PM exposure is a risk factor for cardiorespiratory diseases and lung cancer.
1
The Global Burden of Disease Study estimates ambient PM to be responsible for 3.2 million deaths per year and 76 million years of healthy life lost.
2
Inhalable PM is classified according to the aerodynamic diameter of its particles: coarse (<10
Particulate matter (PM) is divided in three fractions according to the median diameter of the particles
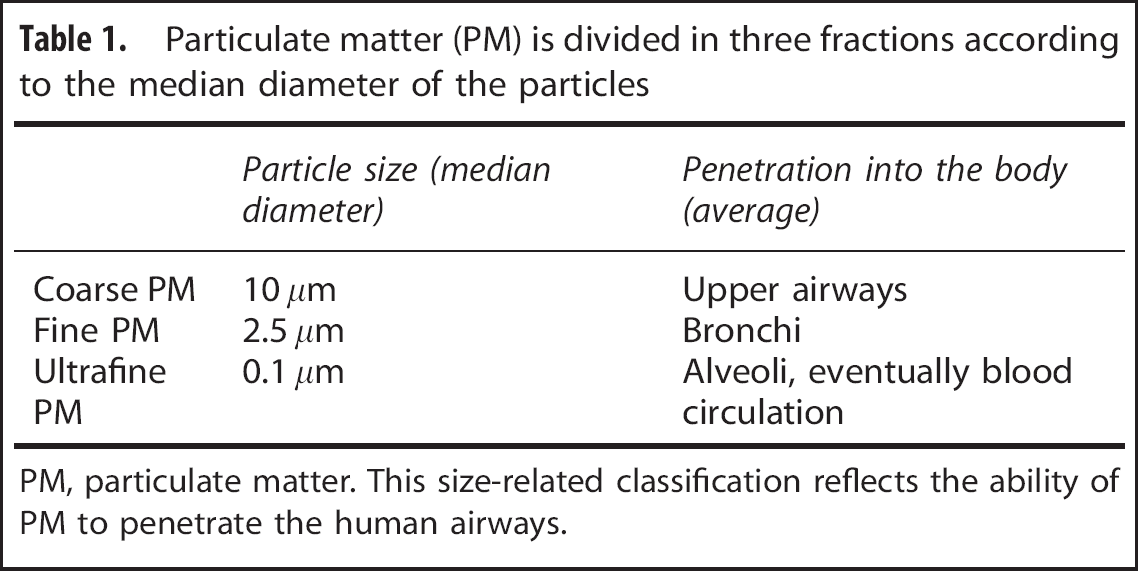
PM, particulate matter.
This size-related classification reflects the ability of PM to penetrate the human airways.
PARTICULATE MATTER AND HUMAN HEALTH
Particulate Matter is a Risk Factor for Cardiovascular and Respiratory Diseases
Particulate matter exposure is thought to induce harmful biologic pathways, both acutely within days and chronically when exposure persists for years or a lifetime. Large time series analyses have been conducted in North America and Europe to estimate the acute health risk of PM exposure.4, 5 It was found that coarse PM levels measured on a daily basis were significantly associated with short-term increases in mortality on individual days, particularly with cardiopulmonary mortality (Table 2). However, risk increases were relatively small and did not exceed beyond 1%. In contrast, cohort studies focusing on chronic PM exposure and longer term cardiovascular endpoints showed a clear relationship (Table 3).6, 7, 8 The Harvard Six Cities study for example found that cardiopulmonary mortality in Steubenville, a US city with high ambient air pollution concentrations over a study period of 14 to 16 years, was increased by 37%.
6
This corresponds to around one fourth of the mortality risk elevation estimated for chronic smokers.
6
Brook
Synopsis of studies investigating PM exposure and acute cardiovascular risk

0.95 CI, 95% confidence interval.
Risk elevations per 10
Synopsis of studies investigating PM exposure and long-term cardiopulmonary risk

0.95 CI, 95% confidence interval.
Risk elevations per 10
Given the accumulating evidence for a clear association of PM exposure with increased cardiovascular morbidity and mortality, safety limits for coarse and fine PM have been introduced in the US and in Europe. Notably however, no study was able to define a threshold below which PM exposure would be harmless. 9
PARTICULATE MATTER AND ISCHEMIC STROKE RISK
The associations between PM and all-type strokes are less clear. Studies from 15 cities in Europe, New Zealand, and Australia failed to find an association between PM exposure and risk of all-type stroke.11, 12 In this section, we will focus on a possible link between PM exposure and IS. We identified all epidemiologic studies, which provided data for the correlation between PM exposure and IS risk, comprising mortality, hospitalization, or stroke survey data. For this, we performed a World Wide Web-based internet search using Medline and PubMed. Our key search terms were any combinations of ‘air pollution’, ‘PM’, ‘stroke’, and ‘Is'. We included all studies, which provided data for an association of PM and IS and which were published in English before 30 July 2013. We have identified 18 studies, which fulfilled these criteria (Table 4).13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31
Synopsis of studies investigating PM exposure and risk of ischemic stroke
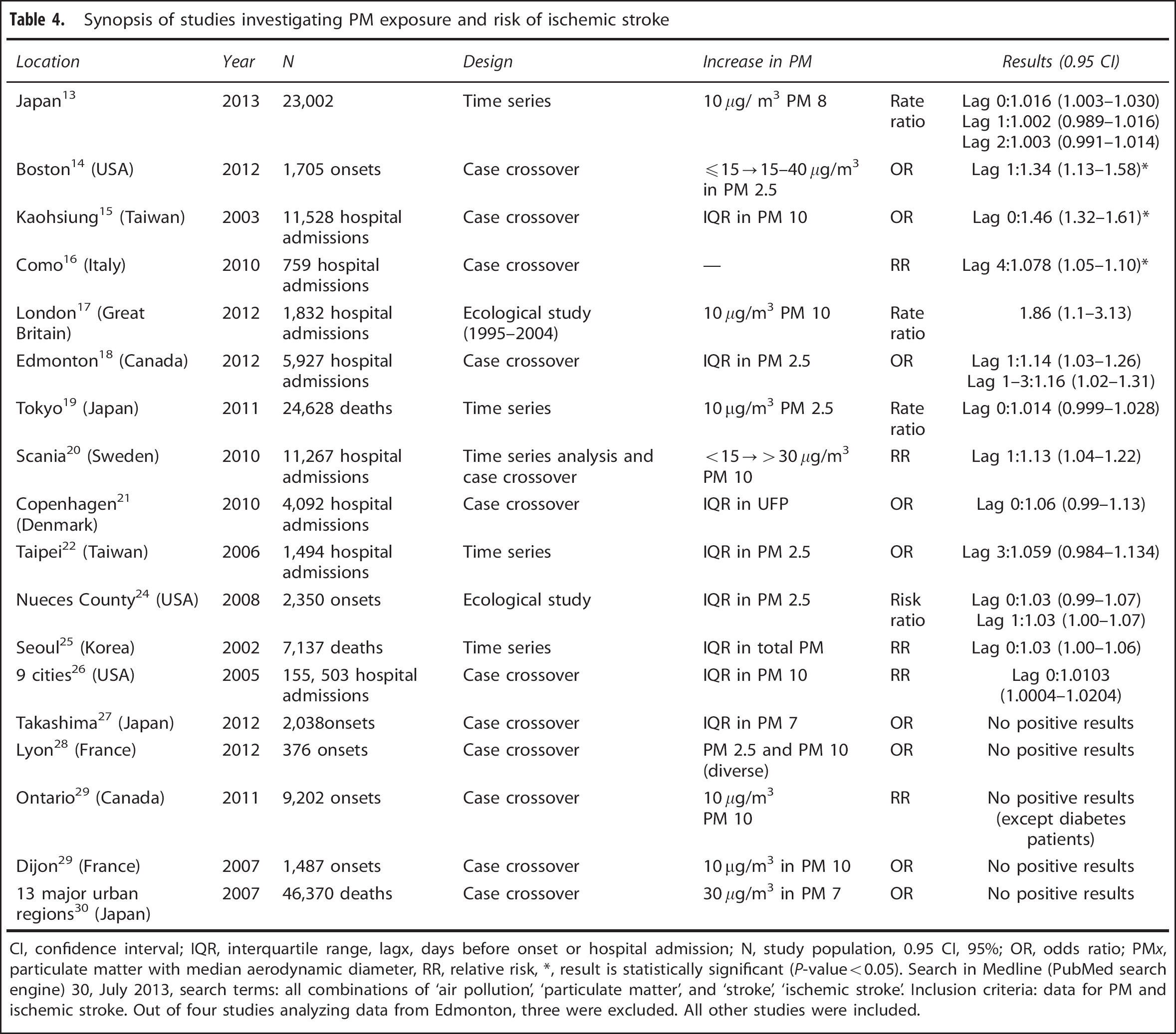
CI, confidence interval; IQR, interquartile range, lagx, days before onset or hospital admission; N, study population, 0.95 CI, 95%; OR, odds ratio; PM
Search in Medline (PubMed search engine) 30, July 2013, search terms: all combinations of ‘air pollution’, ‘particulate matter’, and ‘stroke’, ‘ischemic stroke’. Inclusion criteria: data for PM and ischemic stroke. Out of four studies analyzing data from Edmonton, three were excluded. All other studies were included.
ACUTE EFFECTS OF PARTICULATE MATTER EXPOSURE
Although most studies on PM and cardiovascular diseases have been conducted in developed western countries, first impulses for epidemiologic research on IS came from South Korea and Taiwan.15, 22, 25 An increase in PM by an interquartile range in Seoul was associated with a 3% higher IS mortality. 25 Furthermore, the same increase in PM exposure resulted in a statistically significant increase in the hospitalization rate due to IS in Kaohsiung (Taiwan) of 46%.15, 25 Subsequent studies on a link between IS and PM were conducted in the United States, Japan, and Europe. These are countries in which PM levels are 3 to 5 times lower than in the megacities of emerging nations. The largest of these studies investigated 150,000 IS hospital admissions of people aged 65 or older in nine US cities. 26 An interquartile range increase in coarse PM led to a 1% increase in hospitalizations. 26 Findings of higher IS risks even in areas with absolutely low PM burden, such as in southern Sweden, have further substantiated PM exposure as worldwide risk factor for IS. 20
However, a considerable number of studies did not find a correlation between PM levels and cerebrovascular diseases.20, 27, 28 Only three results reached the level of significance.14, 16, 25 This reveals limitations of comparing air pollution and its influence on health outcomes globally. The composition of PM varies dramatically dependent on pollution sources like car traffic or industry. A recent study from Japan showed that also geographically specific sources of PM, in this case Asian desert dust, are related to IS risk. 32 In addition, most of the risk factors for cerebrovascular diseases on the individual level (especially, coexisting heart disease, hypertension, and also ethnical differences) are not specified in most of the studies.
Although this ecological bias cannot be denied, the design of individual studies has notably been improved during the last years. First
Taken together, there is accumulating evidence for a considerable relationship between PM exposure and IS risk even in moderately polluted regions, in particular for people with preexisting illnesses. However,
BIOLOGIC EFFECTS OF PARTICULATE MATTER ON THE VASCULATURE
Biologic mechanisms leading to harmful PM-dependent effects on health have been examined in several experimental
Exposure to ambient PM initiates typical pathophysiological alterations in men within hours or days.35, 36, 37, 38, 39 Systemic markers of inflammation such as interleukin 6, C-reactive protein, and white blood cell count are increased.35, 36, 37, 38, 39 Furthermore, prothrombotic activity is enhanced and arterial blood pressure is elevated.35, 36, 37, 38, 39 These general findings suggest that exposure to PM triggers a complex systemic signaling cascade. It involves activation of proinflammatory and immune pathways as well as activation of the autonomic nervous system. 9
PARTICULATE MATTER CAUSES SYSTEMIC INFLAMMATION
The most likely gateway for PM into the body is through the alveoli.40, 41 Despite a functioning airway defense such as mucociliary clearance, large fractions of fine and ultrafine PMs are capable of reaching the respiratory zone of the lungs.40, 41
In a recent study, it was demonstrated that PM-induced oxidative stress and inflammation are mediated through activation of the local intrapulmonary innate immune system, i.e. via toll-like receptors and scavenger receptors. 41 Alveolar macrophages and dendritic cells recognize pathogenic patterns via toll-like receptor-4 and scavenger receptor-A. 41 Subsequently, ROS-releasing enzymes such as nicotinamide adenine dinucleotide phosphate-oxidase oxidase are activated, and proinflammatory cytokines such as interleukin 6 are released.41, 42, 43 Large fractions of PM, e.g. transition metals, oxidize phospholipids (surfactants) in the lungs.41, 42, 43 Oxidized surfactants in turn are ligands for toll-like receptor and scavenger receptor.41, 42, 43 This activation of the local pulmonary innate immune system leads to a powerful burst of ROS and proinflammatory markers within the lung parenchyma. In addition, up to 80% of PM, predominantly the coarse fraction, is able to enter pulmonary parenchyma by transcytosis through macrophages and alveolar epithelium cells. 44 These particles can access the pulmonary circulatory system and are subsequently adducted by plasma proteins. 44 As a consequence, the occurrence of these PM–protein complexes in pulmonary and systemic circulations can induce systemic immune responses, particularly in adipose tissue.43, 44
In summary, PM exposure is capable of triggering a complex immune response, which is initiated locally in the lung parenchyma and which subsequently activates systemic proinflammatory cascades (Figure 1). Both mechanisms, the proinflammatory reaction of the lungs and the translocation of particles to other organs, are thought to be responsible for the endothelial dysfunction after PM exposure. 45
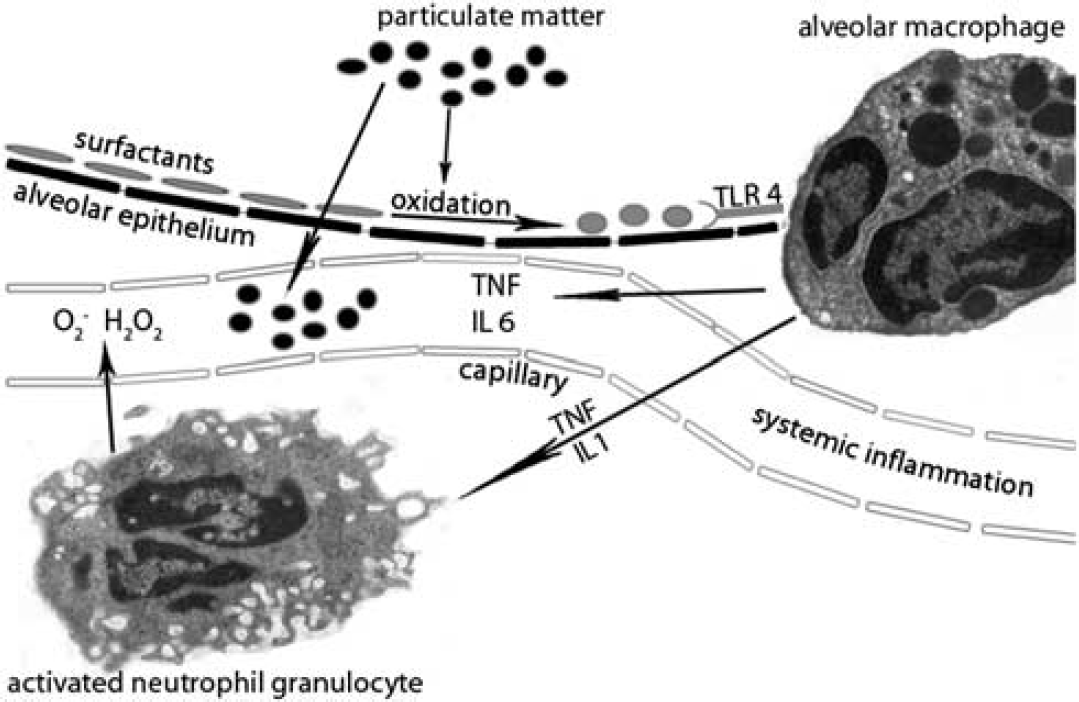
Proinflammatory pathways activated by particulate matter (PM). (Electron microscopy images with kind permission of Dr Kristin Ladell and Dr Gerhard Kolde: http://www.edoc.hu-berlin.de/dissertationen/ladell-kristin-2001-05-25/HTML/). Particulate matter oxidizes surface active agents (surfactants) in the alveoli of the lung. Oxidized surfactants activate toll-like receptor 4 (TLR-4), which stimulates the release of proinflammatory cytokines from alveolar macrophages. This activates the production of reactive oxygen species by local neutrophil granulocytes. In addition, large fractions of PM reach pulmonary circulation via transcytosis through alveolar epithelium cells. These proinflammatory mediators enter pulmonary capillaries and arrive in the circulatory system where they cause systemic inflammation. H2O2, hydrogen peroxide; IL, interleukin, O2−, superoxide radical; TNF, tumor necrosis factor.
PARTICULATE MATTER POTENTIATES RISK FACTORS—ATHEROSCLEROSIS AND THE CRUCIAL ROLE OF PREEXISTING ILLNESS
Systemic inflammatory processes are closely linked to the pathogenesis of atherosclerosis. 46 Even the first stages of vascular dysfunction are characterized by invasion of circulating macrophages into the arterial wall. 46 Later on, during manifest atherosclerosis, both cellularity inside the plaques as well as systemic inflammatory status determine the risk of a plaque rupture. 46 In this context, PM may accelerate systemic and local proinflammatory processes and thereby critically contribute to the progression of the atherogenic cascade.42, 47
Several animal studies investigated the influence of PM exposure on the development of cardiovascular diseases, particularly atherosclerosis and related cardiovascular events. Most of them failed to find significant changes in young and healthy animals. 48 In contrast, atherosclerosis and vascular inflammation significantly exacerbated when transgenic animals with comorbidities were assessed, for example mice with metabolic disorders (apolipoprotein E-knockout mice on a high-fat diet) or rabbits with preexisting atherosclerotic lesions.48, 49 These findings underline the proinflammatory and prooxidative theory of PM-induced vascular damage. It can be hypothesized that PM-derived systemic and vascular proinflammatory processes have a critical additional impact on plaque vulnerability, which, in general, depends on the plaque burden and the systemic inflammatory status (Figure 2). 46 Correspondingly, in clinical studies, individuals with diabetes, obesity, and hypertension have shown greater physiologic responses to PM exposure (including significantly increased blood pressure and white blood cell count).38, 39
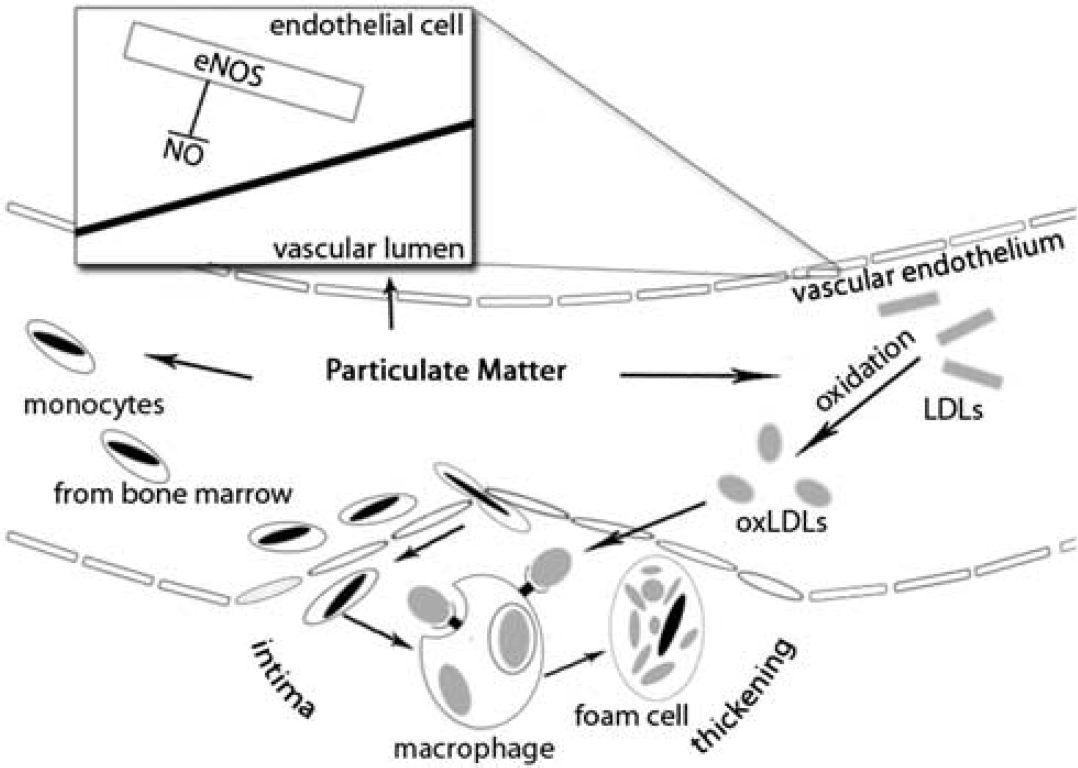
Putative particulate matter (PM)-dependent pathomechanisms leading to potentiation of atherosclerosis. Particulate matter itself and PM-related inflammation oxidize low-density lipoproteins (LDLs). Oxidized LDLs (oxLDLs) are more susceptible to uptake by macrophages in the vessel wall. In addition, inflammation leads to egress of monocytes from the bone marrow, which invade into the atherosclerotic lesions and differentiate to macrophages. Taken together, PM causes plaque growth and increases plaque vulnerability. Particulate matter-related reactive oxygen species also impair nitrogen monoxide (NO) production in the endothelium cells of the vessels. This causes vasoconstriction and breaks down antioxidative protection.
In addition, mechanisms of plaque growth could be linked to PM exposure via lipoprotein metabolism. Particularly, low-density lipoproteins (LDLs), which transfer cholesterol to peripheral tissues, contribute to the number and volume of atherosclerotic lesions. 46 It has been demonstrated that enhanced ROS production results in increasing oxidation of LDLs. 46 These oxidized LDLs have a high affinity to phagocyting macrophages located in subendothelial connective tissue. 46 Consequently, PM exposure could actively accelerate the plaque burden resulting from ROS formation and circulating PM–protein adducts. 47
PERSPECTIVES ON NEUROVASCULAR RESEARCH
The acute impact of PM exposure on ROS formation and the systemic inflammatory status may explain the increased acute IS risk within days as shown in the epidemiologic studies. Wellenius
Importantly, there are two known characteristics, which distinguish the cardiovascular from the presumed cerebrovascular responses to PM exposure. First, a few studies suggested that PM can be translocated directly into the rhinal cortex via olfactory tract and bulb through the cribriform plate. 52 This alternative lung-independent gateway for PM could result in direct damage to the brain parenchyma and vasculature. It has been shown that chronic exposure to urban air pollution can lead to disruption of the blood–brain barrier, endothelial activation, and enhanced inflammatory status of the brain. 53 Second, high LDL levels have not been shown as an independent risk factor for IS in contrast to their high impact on cardiovascular outcomes. 54 However, the PM-driven acceleration of arterial plaque burden is maintained by LDL. 47 Therefore, the proinflammatory and oxidative effects of PM could involve blood levels of LDL in the interaction of risk factors leading to atherosclerosis of the cerebral vessels. Both of these mechanisms provide PM exposure with a particular link to cerebral ischemia.
Taken together, experimental short- and long-term studies
CONCLUSION
There is accumulating evidence for an association of ambient PM exposure and IS risk. Further epidemiologic and experimental studies are necessary to clarify the impact of chronic PM exposure on ischemic brain injury. One crucial aspect in this connection is to decipher the influence of preexisting illnesses and the hazard potential of specific PM sources. Finally, experimental research is warranted to elucidate the deleterious mechanisms of PM exposure on cerebral vasculature.