
Abstract
Carotid occlusions are associated with
Keywords
INTRODUCTION
Perfusion requirements of the brain demand precise maintenance of cerebral blood flow by the basilar artery (BA) and the common carotid arteries. 1 The immediate consequences of cerebral blood flow interruption, including cerebral ischemia and stroke, are widely known. 1 Disturbances in flow often result from carotid artery occlusion caused by moderate or severe atherosclerotic carotid stenosis, which are estimated to be present in 7.5% and 3.1% of the general population, respectively. 2 Additionally, spontaneous or traumatic arterial dissections and thromboembolic events may lead to carotid occlusion. 3
Carotid occlusion can also be artificially induced (e.g. via ligation) as a deconstructive, interventional, or surgical option for treating complex intracranial aneurysms (IAs) that are fusiform, cavernous or giant; carotid dissections, ruptures or cavernous fistulas; or skull base tumors before resection.4, 5, 6 Furthermore, carotid ligation may be necessary after traumatic vascular injury or inadvertent damage to the artery during endoscopic sinus surgery. 7
Carotid occlusion also has lesser-known consequences such as pathologic vascular remodeling within the circle of Willis (CoW). An increasing number of case reports have described
Experimentally, we have performed unilateral and bilateral CCA ligation (BCCA-L) in rabbits and observed a drastic flow increase in the BA
19
and
In this exploratory study, we hypothesized that carotid occlusion causes widespread pathologic changes in the CoW that are not limited to the BT. To test this hypothesis, we adapted our existing BCCA-L rabbit model and investigated the characteristics and extent of flow-induced vascular remodeling in the entire CoW using vascular corrosion casting and scanning electron microscopy (SEM). Results from this preliminary work could shed light on the lesser-known aspects of carotid occlusion related to potential IA formation in the CoW.
MATERIALS AND METHODS
Bilateral Common Carotid Artery Ligation
Female New Zealand white rabbits (4 to 5 kg) underwent BCCA-L surgery (
Vascular Corrosion Casting
Vascular corrosion casting of the CoW was performed on all animals immediately after euthanasia using Batson's No. 17 Corrosion Casting Kit (Polysciences, Inc., Warrington, PA, USA), as described elsewhere. 26 After induction of anesthesia (previously described in refs. 20,22,24), the ligated CCA was accessed via a midline incision in the neck, and heparinized saline was flushed through the vasculature at 250 mm Hg for 10 minutes. After euthanasia and perfusion, approximately 10 mL of Batson's No. 17 Corrosion Cast mixture was injected into the cerebral vasculature via carotid stump. If the distal end of the ligated CCA had clotted, vascular corrosion casting was accomplished by guiding a 4- or 5-French guide catheter endovascularly from the femoral artery to the base of the vertebral artery, at which point the animal was euthanized, perfused, and injected with the casting mixture.
After injection of the casting mixture, whole specimens were kept at 4°C overnight to allow for polymerization of the mixture to occur and to mitigate heat released during the exothermic reaction. The brain, containing the vascular endocast, was excised from the skull and placed in a beaker of 20% potassium hydroxide for 2 days on a rocking platform, with intermittent changes of solution. After the brain tissue dissolved, the cast was isolated and rinsed with distilled water.
Scanning Electron Microscopy Imaging and Mosaic Image Creation
Scanning electron microscopy was used to investigate gross morphologic, macroscopic, and microscopic features of the vascular endocasts. Branching arteries were cut ∼5 mm from the CoW and perforating arteries were removed. For SEM, casts were mounted on a stand with clay, electrically coupled to the stand with graphite paint, and scatter coated with molecular carbon under vacuum. The CoW was imaged at × 50, 5.0 mV with a Hitachi SU-70 scanning electron microscope (Hitachi High Technologies America, Inc., Roslyn Heights, NY, USA). Areas of interest were imaged at higher magnification. Mosaic images covering the entire CoW were created at × 50 using Adobe Photoshop software (Adobe Systems, Inc., San Jose, CA, USA).
Cerebral Vessel Diameter, Length, and Tortuosity Measurement
To assess the gross morphology of the CoW, diameters, and lengths of arteries were measured on mosaic images using ImageJ software (National Institutes of Health, Bethesda, MD, USA). The diameter of each vessel was recorded at three locations and averaged. The lengths of the proximal and distal P1 segments of the posterior cerebral artery (PCA) and the posterior communicating artery (PCom) were measured at the midline from the beginning to the end of each vessel segment. Only the lengths of these posterior arteries were measured, as other vessels in the CoW did not have defined beginnings or endings, thereby making length measurement impossible. Average vessel diameters and lengths were compared between each group using a Student's
For tortuosity quantification, we used the tortuosity index,
19
which normalizes the difference between the vessel arc length (L) and the straight-line chord distance (C) by the straight-line chord distance:
Quantification of Macroscopic and Microscopic Vascular Damage After Flow Increase
To quantify vascular damage throughout the CoW, we divided the mosaic SEM images into nine arterial regions comprising either branch-point regions (defined by a 500
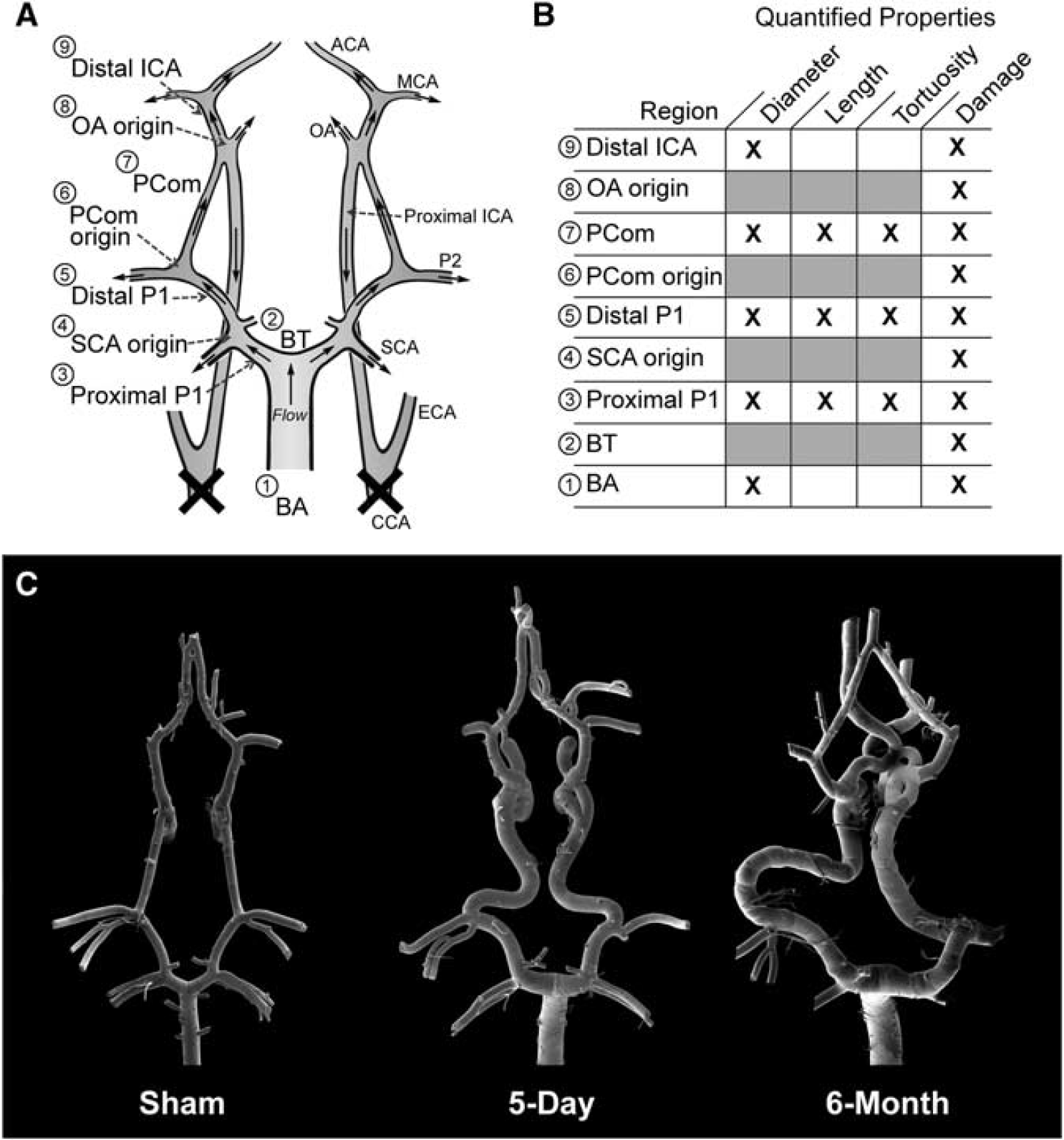
Overview of morphologic changes that developed in the rabbit circle of Willis (CoW) after bilateral carotid ligation. (
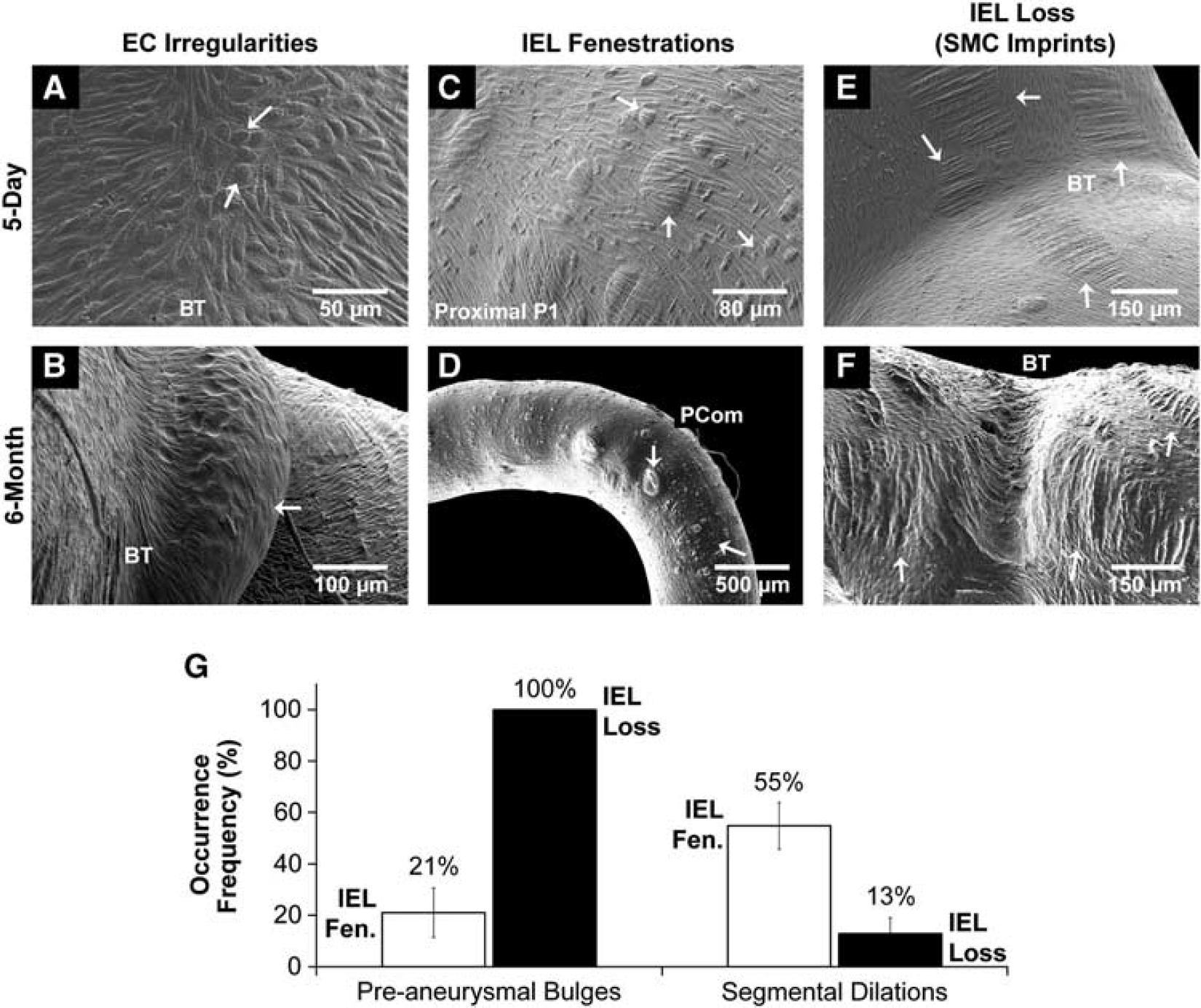
Five types of vascular damage were observed and stratified based on the increasing severity of aneurysmal remodeling: endothelial cell (EC) irregularities—deviations from healthy, spindle-shaped, flow-aligned ECs. The presentation of a rough and irregular endothelial surface has conventionally been interpreted as a sign of EC dysfunction.26, 27, 28 Internal elastic lamina (IEL) fenestrations—raised circular lesions on the cast surface with defined boarders, representing indentations in the vessel lumen due to focal weakening of the IEL 29 or luminal matrix degradation. 21 Smooth muscle cell (SMC) imprints—striations perpendicular to the direction of flow that are indicative of massive IEL loss, which places the endothelial layer directly onto the medial layer such that imprints of the SMC structures are visible on the cast surface. 30 These SMC imprints are distinctly different than the presentation of IEL fenestrations, which are smaller, slightly raised, and lack visible SMC structures; fenestrations indicate that the IEL is degraded but not massively, as in the case of SMC imprints. Segmental dilations—localized arterial expansions involving the entire circumference of a short vessel segment. Preaneurysmal bulges—localized outpouchings of the artery on one side of the affected vessel. This structure does not have a neck and is not a full-blown aneurysm.
The damage in each arterial region was evaluated by 3 masked observers using a progressive graded scoring method (Table 1). Our scoring system improved upon previous methods28, 31 by accounting for the presence of both macroscopic and microscopic vascular damage. This comprehensive score, termed the vascular damage score (VDS), ranged from 0 (no damage) to 30 (maximum damage). The average VDS of every region was compared between groups with a Student's
The VDS grading system accounting for five types of vascular damage
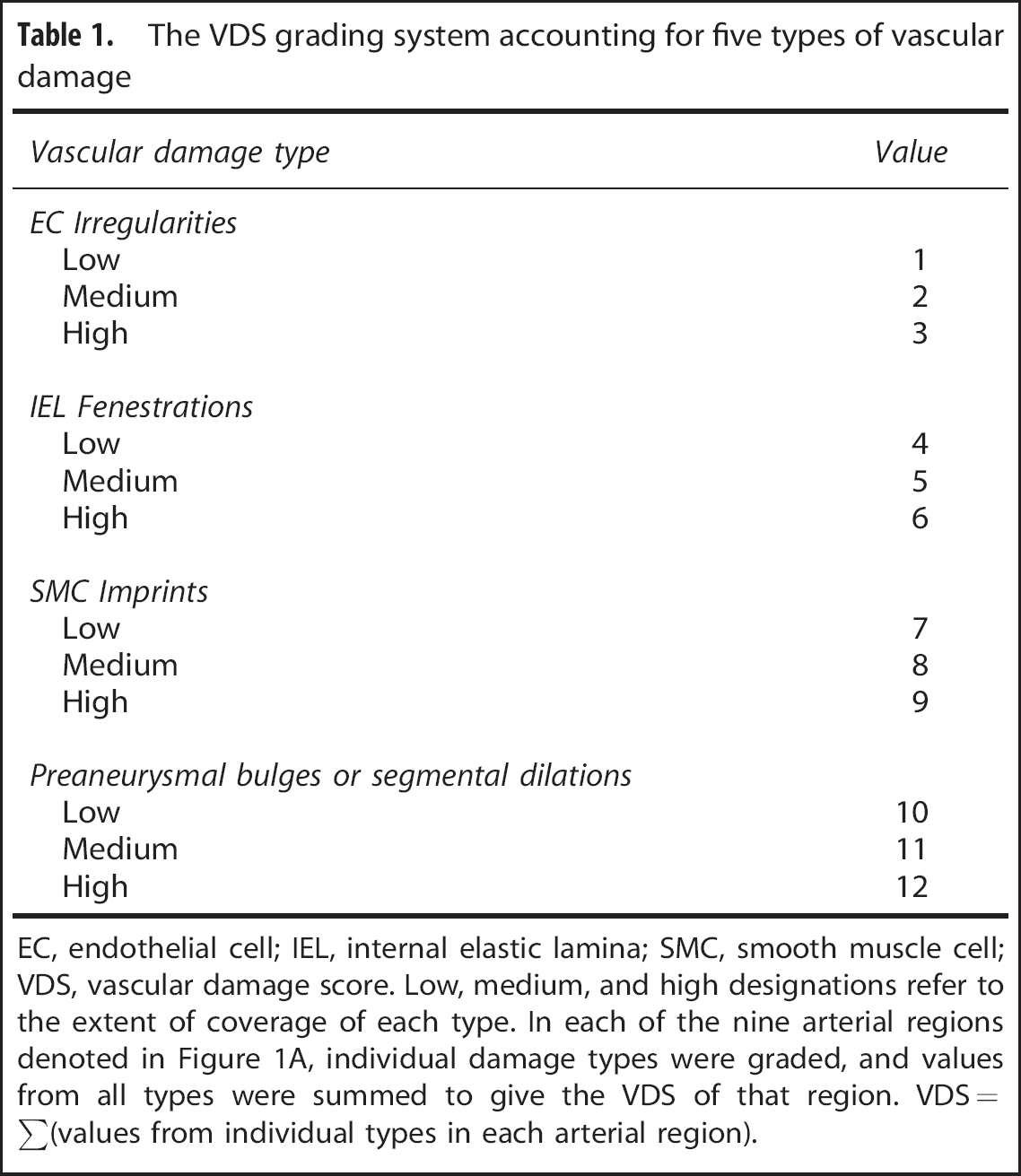
EC, endothelial cell; IEL, internal elastic lamina; SMC, smooth muscle cell; VDS, vascular damage score.
Low, medium, and high designations refer to the extent of coverage of each type. In each of the nine arterial regions denoted in Figure 1A, individual damage types were graded, and values from all types were summed to give the VDS of that region.
VDS=∑(values from individual types in each arterial region).
To determine the localization of vascular damage, the presence or absence of each type of vascular damage, regardless of degree, was analyzed at every arterial region and recorded as an occurrence frequency. The average occurrence frequency of preaneurysmal bulges and segmental dilations in every region was compared between 5-day and 6-month animals with a Student's
Correlation between Vascular Tortuosity and Segmental Lesions
We examined the relationship between PCom tortuosity index and the presence of segmental dilations on the PCom. The tortuosity indices of PComs containing an equal number of segmental dilations were averaged, and the number of PCom dilations was plotted against the average tortuosity index. Power regression analysis was used to assess correlation. The average VDS for each group of PComs was also computed.
Scanning Electron Microscopy Image Comparison with Histology at the Basilar Terminus
Vascular corrosion casting prohibited any biologic investigation of vascular tissue, as all organic structures were degraded in the process of isolating the endocasts. In order to gain additional insight into structures observed on the cast surfaces, we compared our cast data with available histologic sections at the BT in rabbits that underwent BCCA-L from our previous studies. 22 We spatially matched SEM images of the endocasts at the BT with representative sections stained with van Gieson's stain for each experimental group.
RESULTS
Carotid Ligation Increased Vessel Caliber and Length at 5 days and 6 Months
Bilateral CCA ligation caused vascular remodeling in gross morphology, as shown in the representative mosaic images of vascular endocasts in Figure 1C. The vessel calibers in the 5-day BCCA-L group were significantly augment compared with sham at the BA (54±9%,
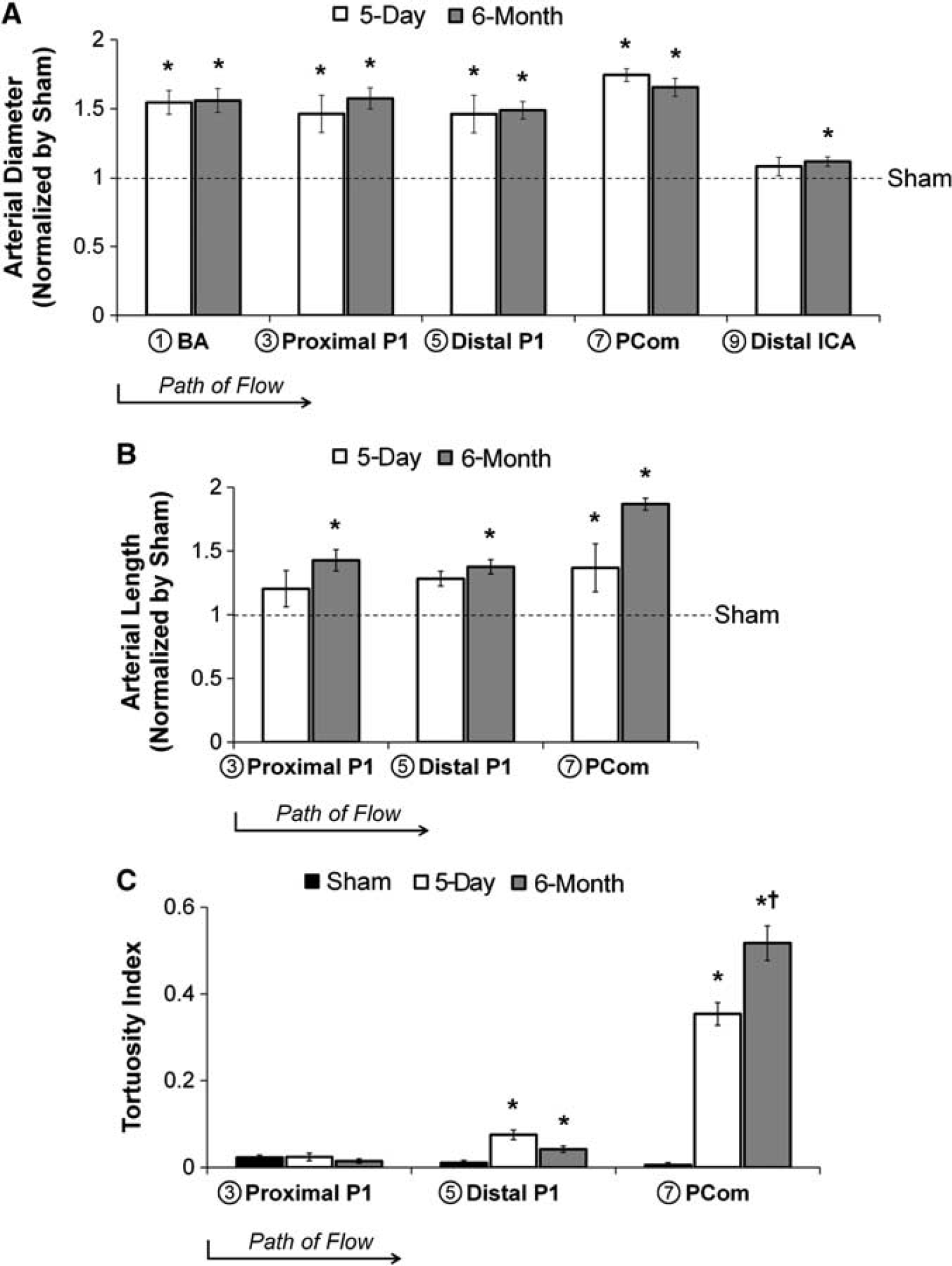
Arterial diameter, length, and tortuosity index at multiple locations in the circle of Willis 5 days and 6 months after bilateral carotid ligation. (
The lengths of the proximal P1, distal P1, and PCom were measured on the endocasts. In the 5-day BCCA-L group, the length of the PCom, but not that of the proximal P1 or the distal P1, was significantly increased when compared with sham (37±19%,
Carotid Ligation Increased Tortuosity in the Posterior Communicating Artery Progressively
Vessels of the posterior circulation were more tortuous in the experimental group than in the sham group, as shown in Figure 1C. To quantify tortuosity, we used a previously described index based on the vessel arc-to-chord ratio. As shown in Figure 2C, the tortuosity index on the proximal P1 was unchanged across all groups, whereas on the distal P1, it was increased significantly in both experimental groups, compared with sham. Yet, by far, the largest increase in tortuosity index was on the PCom: 0.35±0.03 for the 5-day ligated group (
Gross Aneurysmal Changes after Flow Increase
Besides vessel caliber, length and tortuosity increase, carotid ligation also resulted in aneurysmal changes within the CoW. At the macroscopic level, we observed two types of aneurysmal remodeling: bulges and segmental dilations. Overall, the most noticeable preaneurysmal bulges were found at the BT and at the OA origin, whereas most segmental dilations were found on the PCom. The presentation of these structures was as follows:
Preaneurysmal bulges
In the 5-day ligated group, 60% of the casts presented preaneurysmal bulges exclusively at the OA origin (Figures 3A and 3C). In the 6-month ligated group, these lesions presented at other branch points in the CoW. Preaneurysmal bulges varied in size, ranging from small blips to large lesions. Most distinctive were the preaneurysmal bulges that presented at the BT (50% of the casts) and the OA origin (55% of the casts) (Figures 3B and 3C). Such development was not observed in sham casts.
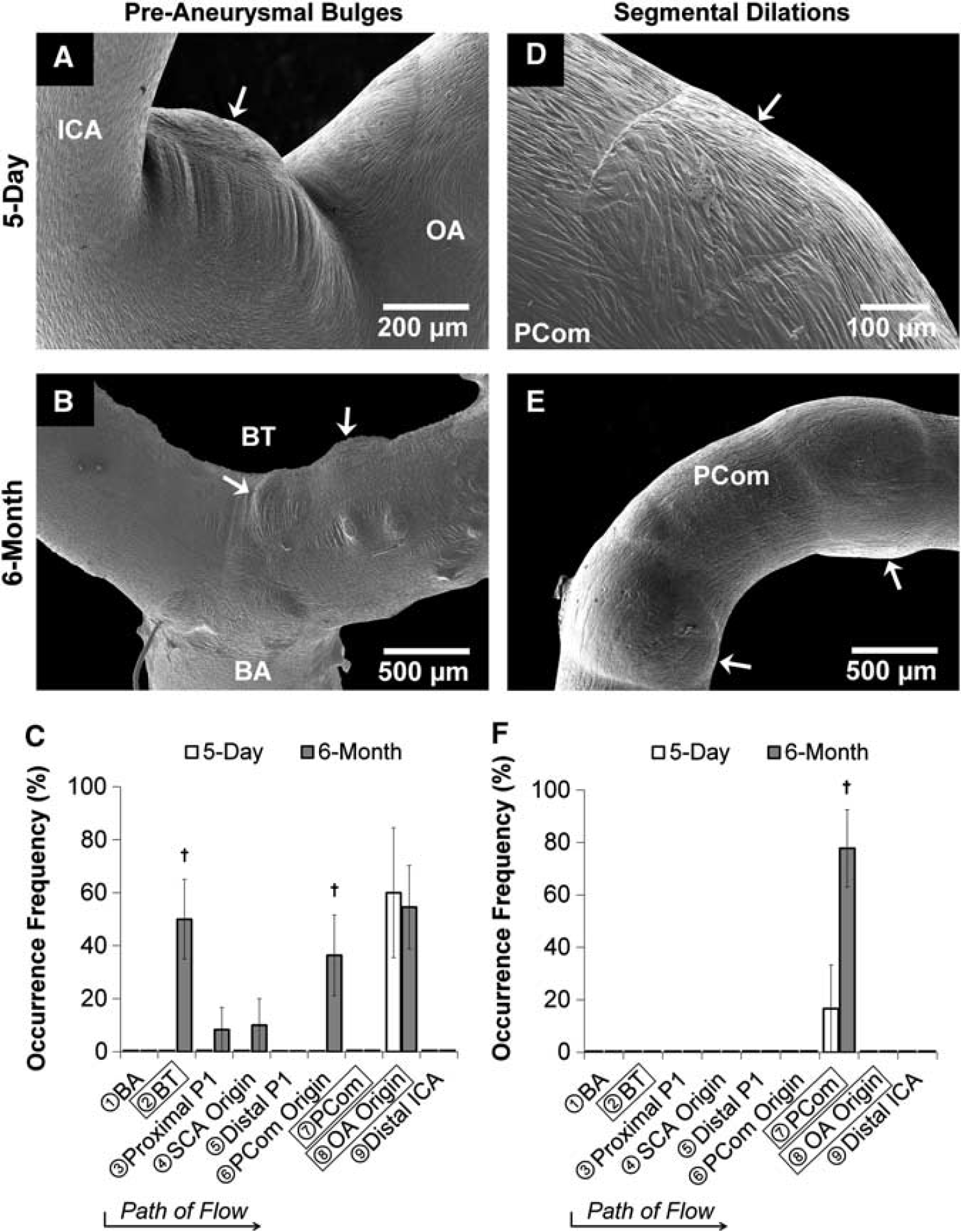
Gross aneurysmal remodeling in the circle of Willis after bilateral carotid ligation evident from scanning electron microscopy images of vascular casts (
Segmental dilations
In the 5-day ligated group, 17% of the casts presented minor segmental dilatations on the PCom, which were observed as slight dilations around the vessel (Figures 3D and 3F). In the 6-month ligated group, 78% of the casts presented large segmental dilatations exclusively on the PCom. On average, these segmental dilatations increased vessel diameter 13±2%,
Microscopic Pathologic Changes after Flow Increase
In addition to preaneurysmal bulges and segmental dilations, damage at the microscopic level, including EC irregularities, IEL fenestrations, and SMC imprints, was also observed on the endocasts of the experimental groups. The presentation of these structures was as follows:
EC irregularities
As expected, ECs aligned parallel to the flow in straight vessel segments. Irregular EC morphology presented at the saddles of bifurcations in the 5-day and 6-month BCCA-L groups (Figure 4A). Furthermore, in the 6-month ligated group, some casts were devoid of ECs at preaneurysmal bulges, indicating the presence of an acellular environment (Figure 4B). Only sparse EC irregularities were observed in bifurcation saddles on sham casts.
Microscopic changes in the circle of Willis after bilateral carotid ligation. (
IEL fenestrations
In the 5-day BCCA-L group, IEL fenestrations (Figure 4C) were present throughout the CoW. They were most densely populated on the proximal P1, distal P1, and PCom, and were less frequently present on the BT. They varied in size from 5 to 50
SMC imprints
In the 5-day group, there were a large amount of SMC imprints at the OA origin, the BT, the PCA, and PCom (Figure 4E). In the 6-month group, large regions of SMC imprints (IEL loss) at these regions were more numerous when compared with 5-day casts. At bifurcations, SMC imprints often existed on top of preaneurysmal bulges, and on straight vessels, they existed independently of segmental dilations (Figure 4F). This structure was not observed in sham casts.
Internal Elastic Lamina Loss Colocalizes with Preaneurysmal Bulges, whereas Internal Elastic Lamina Fenestrations Colocalize with Segmental Dilations
To investigate the possible role of IEL damage in the pathogenesis of macroscopic damage, we analyzed the localization of IEL fenestrations and SMC imprints (IEL loss) to preaneurysmal bulges and segmental dilations. All (100%) of preaneurysmal bulges were colocalized with IEL loss, whereas only few (21±9.6%) had IEL fenestrations (Figure 4G). However, segmental dilations principally colocalized with regions of IEL fenestrations (55±9.1%) and not SMC imprints (13±6.1%) (Figure 4G). This is consistent with the widely accepted observation that IEL loss is a hallmark of saccular IA.
Vascular Damage was Progressive with Time
We used the VDS (see Table 1) to quantify vascular damage in the CoW. In the 5-day group, the VDS was significantly increased in six arterial regions: the BT, proximal P1, distal P1, PCom, and OA origin (Figure 5A). Microscopic damage contributed primarily to the increase in VDS at these regions compared with sham, except the OA origin, which developed preaneurysmal bulges. In the 6-month group, the VDS was significantly increased in all regions except the distal ICA when compared with sham (Figure 5A). When compared with the 5-day group, the 6-month group had significantly increased VDS at the BT, proximal P1, PCom origin, and PCom, primarily because of increased preaneurysmal bulges and segmental dilations.
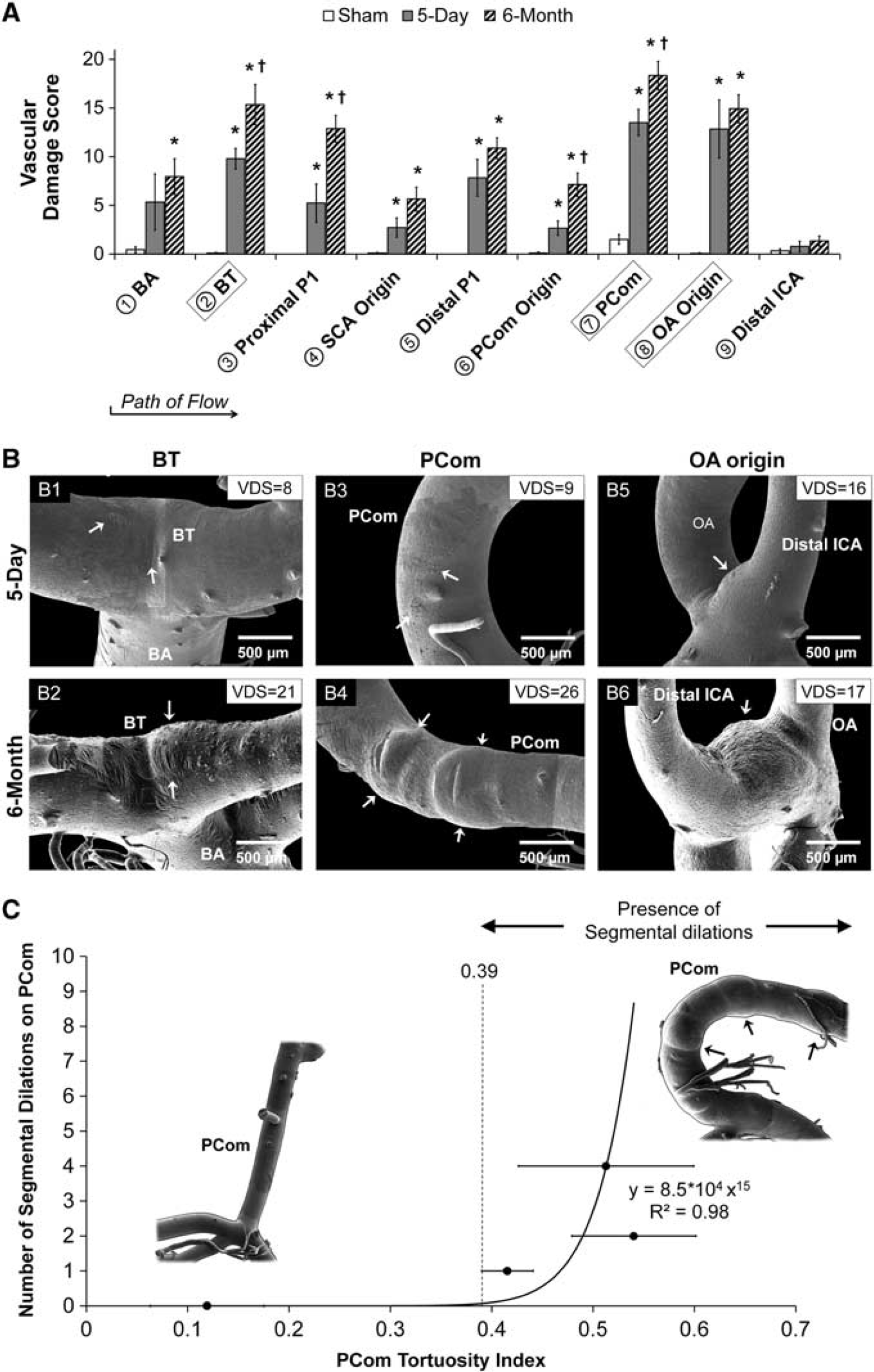
Quantification of aneurysmal changes in the circle of Willis (CoW) after bilateral carotid ligation. (
Of the three arterial regions that had the highest VDS (the BT, PCom, and OA origin), we noticed striking differences between 5-day and 6-month groups. After the flow direction, the BT presented SMC striations at 5 days and preaneurysmal bulges at 6 months (Figures 5B1 and 5B2), the PCom was populated with IEL fenestrations at 5 days and then presented segmental dilations at 6 months (Figures 5B3 and 5B4), and the OA origin presented preaneurysmal bulges at both time points (Figures 5B5 and 5B6). These changes were reflected in the VDS at both time points.
Segmental Dilations Correlated with Elevated Tortuosity
We discovered that distinctive segmental dilations were present exclusively on PComs of the 6-month group, which also presented the highest tortuosity index. To test whether there was a correlation between tortuosity and segmental dilation presentation, we grouped PComs by the number of segmental dilations, calculated the average tortuosity index for each group, and then plotted the number of dilations against average tortuosity index. This plot displayed a power trend with the equation
Aneurysmal Damage Observed at the Basilar Terminus Mirrored Histologic Findings
Mosaic SEM cast images at the BT were compared with representative BT histologic sections from rabbits that underwent BCCA-L. Figure 6 shows two sets of rabbit BTs (5-day and 6-month BCCA-L) with similar geometry and dimensions. We qualitatively matched the local environment around the bifurcation apex and found equivalent pathologic damage levels on the two types of data (Figure 6A): quasi-continuous IEL that was minimally disrupted in histology corresponded to small isolated IEL fenestrations on the endocasts, large segments of IEL loss corresponded to large areas of SMC imprints, and medial thinning due to SMC loss corresponded to acellular preaneurysmal bulges. Five-day BCCA-L BTs presented a central region of IEL loss surrounded by a region of uninterrupted IEL where small isolated IEL fenestrations presented (Figure 6B, left panel), whereas 6-month BCCA-L BTs presented an acellular bulge flanked by IEL loss and intermittent IEL fenestrations (Figure 6B, right panel).
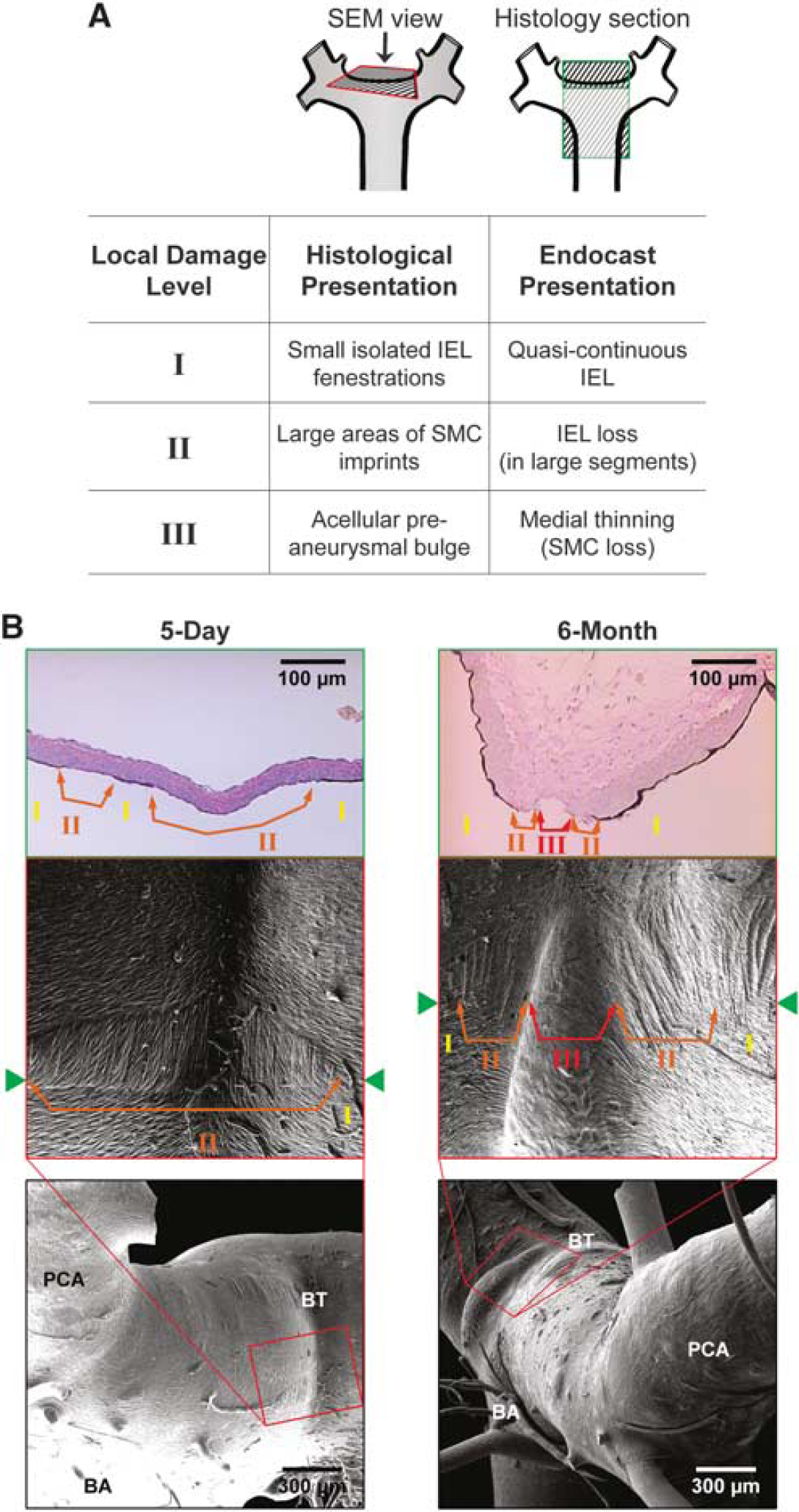
Comparison of aneurysmal damage presentation on scanning electron microscopy (SEM) images with presentation on histology of the basilar terminus (BT). (
DISCUSSION
Our data demonstrate that flow increase after carotid ligation elicits not only compensatory adaptive arterial enlargement in the CoW, but also pathologic remodeling such as tortuosity and aneurysm development. Five days after carotid ligation, we observed a significant increase in vessel calibers of the CoW as well as in the length and tortuosity of the PCom, and preaneurysmal bulge presentation at the OA origin. Although there was no additional increase in vessel diameters at 6 months post ligation versus 5 days, the PCom further increased in tortuosity and presented segmental dilations, and the OA origin and BT presented preaneurysmal bulges.
Adaptive and Pathologic Remodeling After Carotid Occlusion
Early compensatory caliber increase throughout the CoW at 5 days is an adaptive response of the cerebral arteries to the sustained elevation of blood flow, with the purpose of returning WSS to physiologic baselines.1, 32 Our results are consistent with previous studies using the BCCA-L model, where we showed that BA caliber increased immediately after carotid ligation whereas WSS in the BA decreased sharply and returned to baseline within 4 to 5 weeks. 20 After this WSS normalization, there was no further increase in BA diameter. 20 Thus, it is not surprising that in our experiments vessel calibers at 6 months were not further increased from those at 5 days.
In addition to adaptive vessel enlargement, we have shown that pathologic remodeling such as preaneurysmal bulges and segmental dilations also developed in response to carotid ligation. This is consistent with reports of IA initiation at the BT after both BCCA-L20, 21, 22, 24 and unilateral CCA ligation.20, 23 Specifically, Meng
Besides aneurysmal development, PCom tortuosity increased with time after carotid ligation. Development of tortuosity on the PCom in response to flow increase is consistent with our previous observations of tortuosity on the BA after BCCA-L. 19 The IEL fenestrations present on tortuous PComs in this study parallel focally fragmented IEL on histologic slides of tortuous BAs, suggesting that tortuosity development is facilitated by localized IEL damage. 19 (Owing to the vascular cast isolation procedure, BAs were not completely preserved; therefore, we were unable to quantify BA tortuosity in the current study)
Complex Hemodynamics in Pathological Remodeling after Carotid Occlusion
This study provides preliminary evidence that flow change subsequent to carotid ligation alone can induce pathologic remodeling and vascular damage in the CoW. Our previous studies of BT aneurysm formation in the same model (rabbit BCCA-L) have demonstrated that aneurysmal remodeling is a maladaptive response to elevated hemodynamic stresses.22, 24 Through detailed hemodynamics–histology mapping, we found that IA initiation at the BT (defined by regions of IEL loss) was associated with high WSS combined with positive WSS gradient above a threshold.24, 33 This hemodynamic condition, often associated with bifurcation apices,
34
has been recognized to independently cause
Our data also show that flow-induced segmental dilations are accompanied by progressive tortuosity increase. Although little is known about it, abnormal cerebral vascular tortuosity could be an adaptive response to increased flow burden, which manifests mechanical instability in the arterial walls. 37 In tortuous vessels, flow impinges on the outer wall of bends. To make the turn of a bend, flow along the outer curve has to travel at a higher velocity than flow along the inner curve, and has to accelerate. This creates a local hemodynamic environment with high WSS and positive WSS gradient, not dissimilar to that of bifurcation apices. 35 Based on the observed aneurysmal changes present in tortuous PComs, we speculate that high WSS and positive WSS gradient at outer curves may have triggered IEL damage 24 and aneurysmal remodeling, 19 contributing to the progressive development of tortuosity as well as segmental dilation. The relationship between tortuosity and segmental dilation and their respective etiologies should be further elucidated.
Clinical Implications
The aneurysmal development after carotid ligation in our preliminary experiments mirrors clinical case reports of
Clinically, acute or chronic carotid occlusions are frequently diagnosed, sometimes with acute catastrophic consequences because of immediate flow limitation, but more commonly with few apparent effects.
38
Our study demonstrates that bilateral carotid occlusion could lead to significant pathologic remodeling, specifically aneurysm initiation and vascular tortuosity in the CoW.
Current management algorithms for carotid occlusion rely mostly on the presence of ischemic symptoms and the extent of collateral circulation.39, 40 Presently, there is no consideration for ongoing or new pathologic vascular remodeling of the neurovasculature, which could go undetected for years. Perhaps more aggressive consideration should be placed on reconstituting acute occlusion, particularly in the younger patients, as they may be exposed to a longer duration of abnormal hemodynamic insult after occlusion. In addition, routine screening and protracted follow-up vascular imaging for those with complete carotid occlusion, regardless of etiology may be warranted.
Limitations
First, we recognize that we examined only a few experimental and control replicates in this study. As no previous data was available for power analysis for these experiments, we performed
Second, even though three-dimensional digital subtraction angiography was available for each animal, we did not perform computational fluid dynamics (CFD) analyses for the CoW to obtain hemodynamics at the pathologic sites. Unlike CFD modeling of a regional vascular segment that involves only one inlet (e.g. the BA) and two outlets (e.g. the PCAs), the vascular regions to be mapped in the current study would have to involve the entire CoW. In this case, CFD would be inaccurate because of multiple unknown inlet boundary conditions and especially owing to the unknown outlet velocity boundary conditions, which involve the distal vascular beds. Modeling the distal microvasculature would require many assumptions.
Third, we recognize that the flow manipulation used in this study was acute. While some carotid occlusions do occur rapidly, e.g. traumatic or iatrogenic occlusion, most of them develop over time. However, acute flow increase in the absence of other risk factors performed in this study accentuates the potential damage that hemodynamic insult could produce. When a patient harbors other risk factors and comorbidities, the resulting vascular damage could well occur even in a less acute situation, as these factors may increase susceptibility to flow-induced damage.
CONCLUSION
Although carotid occlusions have been associated with
Footnotes
VMT—None. MM—None. HC—None. LCP—None. AS—Co-investigator of the National Institutes of Health grant (R01NS064592). Financial interests in Hotspur, Intratech Medical, StimSox, and Valor Medical. Consultant/advisory roles for Codman & Shurtleff, Concentric Medical, ev3/Covidien Vascular Therapies, GuidePoint Global Consulting, and Penumbra. Received honoraria from Abbott Vascular, Codman & Shurtleff, Genentech, and Neocure Group LLC. JK—Co-investigator of the National Institutes of Health grant (R01NS064592). HM—Principal investigator of the National Institutes of Health grant (R01NS064592).
ACKNOWLEDGMENTS
This material is based upon work supported by the National Institutes of Health under grant number (R01NS064592) (HM). We gratefully acknowledge Peter Bush for SEM instrumentation assistance, Akira Takahashi at Tohoku University for guidance on corrosion casting, and Christopher Martensen, Jessica Utzig, and Kaitlynn Olczak for help with mosaic SEM image grading.