
Abstract
Previous studies have highlighted the enormous potential of cell-based therapies for stroke not only to prevent ischemic brain damage, but also to amplify endogenous repair processes. Considering its widespread availability and low immunogenicity human umbilical cord blood (HUCB) is a particularly attractive stem cell source. Our goal was to investigate the neurorestorative potential of cryopreserved HUCB mononuclear cells (MNC) after permanent middle cerebral artery occlusion (MCAO) in spontaneously hypertensive rats (SHR). Human umbilical cord blood MNC or vehicle solution was administered intravenously 24 hours after MCAO. Experimental groups were as follows: (1) quantitative polymerase chain reaction (PCR) of host-derived growth factors up to 48 hours after stroke; (2) immunohistochemical analysis of astroglial scarring; (3) magnetic resonance imaging (MRI) and weekly behavioral tests for 2 months after stroke. Long-term functional outcome and lesion development on MRI were not beneficially influenced by HUCB MNC therapy. Furthermore, HUCB MNC treatment did not change local growth factor levels and glial scarring extent. In summary, we could not demonstrate neurorestorative properties of HUCB MNC after stroke in SHR. Our results advise caution regarding a prompt translation of cord blood therapy into clinical stroke trials as long as deepened knowledge about its precise modes of action is missing.
Keywords
INTRODUCTION
Cerebral ischemia is one of the leading causes for death and disability in industrialized countries. The most crucial limitation of stroke treatment is the narrow time window for effective clot lysis that has often elapsed when stroke patients arrive at hospital. Much effort has thus been made to explore novel therapeutic concepts that permit successful treatment even days after stroke onset. Amongst others, cell-based therapies are considered a promising approach, especially for those patients being ineligible for thrombolysis or missing the thrombolysis time window. Human umbilical cord blood (HUCB) mononuclear cells (MNC) constitute a particularly attractive stem cell source because of little ethical concerns on the use in humans, long-term cryostorage eligibility, and widespread availability.
1
Another advantage relates to the immaturity of HUCB MNC and their immune naivete limiting the incidence and severity of graft–versus-host diseases compared with bone marrow transplants.
2
There is ample experimental evidence for functional improvement after intravenous HUCB MNC transplantation in animal models of stroke from our group3, 4 (using spontaneously hypertensive rats, SHR) and others.5, 6, 7 However, underlying mechanisms are not yet fully understood. Human umbilical cord blood MNC are able to adopt a neuronal phenotype in cell culture, but integration and neuronal differentiation of grafted HUCB MNC in the recipient's central nervous system, if occurring at all, is a rare event.
8
Thus, the common understanding is that HUCB MNC exert their beneficial properties via bystander effects rather than cell replacement. A widely discussed mode of action is that HUCB MNC might increase local growth factor levels thereby contributing to a regenerative microenvironment.
9
In fact, a recent study revealed that transplanted HUCB MNC enhance local messenger RNA (mRNA) levels of vascular endothelial growth factor and brain-derived neurotrophic factor (BDNF) after perinatal hypoxic–ischemic brain injury
Some well-designed studies were not able to fully reproduce the aforementioned beneficial effects of HUCB MNC after experimental stroke.13, 14 It is conceivable that differences in cell storage and processing may contribute to these controversial results. In fact, there is an ongoing debate whether either the composition or the functionality of cord blood cells or both is altered by the process of cryopreservation. 15 This applies all the more, as HUCB consists of many cell types and it is currently unclear which cell subset (or combination of subsets) exactly determines the efficacy of HUCB MNC in ischemic stroke. Although many preclinical studies that reported beneficial effects of HUCB MNC after central nervous system injury used freshly donated cord blood, this approach will not be feasible in the clinical routine. Moreover, long-term assessment of functional endpoints as especially relevant for the human target group was only performed in a minority of studies reporting positive impact of HUCB MNC treatment on stroke recovery. 3
Hence, the primary aim of the present study was to assess whether intravenous transplantation of cryopreserved HUCB MNC induces sustained functional benefits after ischemic stroke in SHR, a strain exhibiting comorbidities such as hypertension and hypercholesterolemia representing common stroke risk factors. The potential therapeutic impact was also evaluated by sequential magnetic resonance imaging (MRI) assessing lesion development and secondary hemispheric atrophy. As additional endpoints, transcriptional modulation of endogenous growth expression by HUCB MNC treatment and its influence on postischemic astrogliosis as possible mediators of functional recovery were assessed.
MATERIALS AND METHODS
Sample Size Calculation
Functional recovery was defined as the primary endpoint of this study. Group sizes were intended to detect an effect size of 25% in the area under the curve analysis of the respective behavioral tests and were calculated via
Preparation of Human Umbilical Cord Blood Mononuclear Cells
Human cord blood was obtained from healthy full-term pregnancies after informed consent according to the principles outlined in the Declaration of Helsinki. The mononuclear fraction was separated from the cord blood by density gradient centrifugation. Subsequently, the obtained MNC population was frozen to −80°C in 10% dimethyl sulfoxide and fetal calf serum using a Nalgene cooling box. Before use, vials were thawed in a water bath (37°C). Then, vials were rapidly transferred to 15 mL Falcon tubes with 1 mL of DNAse-containing buffer (75 U/mL DNAse/0.5 mol/L Mg2Cl2). 10 mL of RPMI medium (PAA, Linz, Austria) were added to dilute dimethyl sulfoxide. After centrifugation, the cell pellet was washed three times in RPMI and 10% fetal calf serum. Finally, the number of live and dead cells was determined by trypan blue staining. Viability data and information regarding the content of CD34+ cells among HUCB MNC are provided by Supplementary Table 1 in the Supplementary Information.
Experimental Stroke and Group Allocation
Investigations conformed to the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85-23, revised 1996) and were performed according to the ARRIVE guidelines (http://www.nc3rs.org/ARRIVE). All animal procedures were approved by the appropriate federal agency (protocol number TVV18/07). In total, 108 male SHR at the age of 14 weeks were subjected to permanent distal middle cerebral artery occlusion (MCAO) according to the Tamura model.
17
After surgery, animals were randomly assigned to cell therapy or a control group (
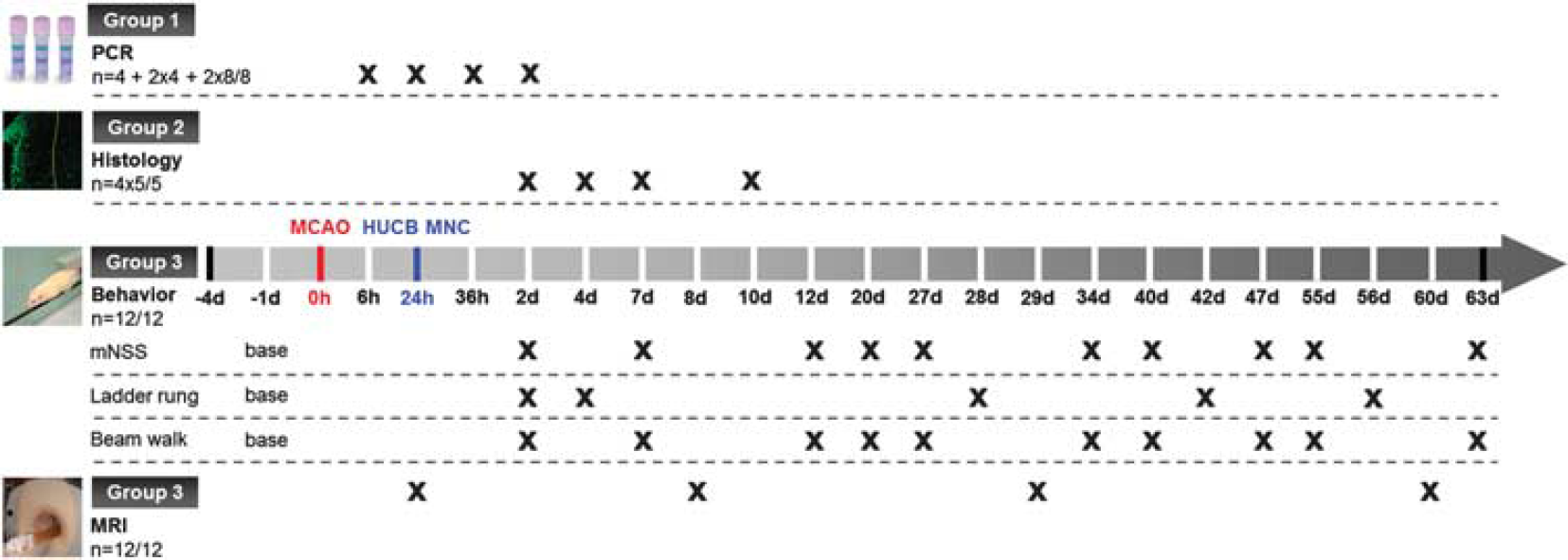
Study design. MCAO: middle cerebral artery occlusion; human umbilical cord blood (HUCB) mononuclear cells (MNC): systemic cord blood therapy; polymerase chain reaction (PCR): quantitative real-time PCR; histology: immunofluorescence analysis of astroglial scarring; MRI: magnetic resonance imaging.
Exclusion Criteria
The exclusion criteria were as follows: (i) death within 24 hours after MCAO (ii) lack of an ischemic lesion in the distal supply territory of the MCA in T2-weighted (T2-w) MRI 1 day after stroke induction. To compensate for dropouts, five additional animals were enrolled to the study population, resulting in an overall study population of 113 rats.
Brain Tissue Sampling
Animals were killed according to survival periods. For analysis of mRNA expression (group 1), rats were transcardially perfused with ice-cold PBS. Removed brains were cut into 2 mm thick coronal slices and samples of approximately 8 mm3 were taken from the upper and lower infarct border zone. The infarct border zone could be differentiated from intact brain tissue by slight changes of opacity and color. All specimens were transferred into RNAlater RNA stabilization reagent (Qiagen, Hilden, Germany) and stored at −20°C until further use. Animals randomized to immunofluorescence analysis of astroglial scarring (group 2) were perfused with body-warm PBS and ice-cold formalin solution (4%). Thereafter, brains were removed, vitrified in 30% sucrose, and cryopreserved at −80°C. Further staining procedures were performed on coronal cryosections (20
Quantitative Real-Time Polymerase Chain Reaction
Gene expression profiles of rodent nerve growth factor, BDNF, basic fibroblast growth factor, insulin-like growth factor 1 (IGF-1), glial fibrillary acidic protein (GFAP), Nestin, and the housekeeping gene YWHAZ were evaluated 6 (
Immunofluorescence Analysis of Reactive Astrogliosis
The density of GFAP and Nestin-positive structures within the ischemic lesion border was determined 2, 4, 7 and 10 days after stroke onset (
Neurofunctional Tests
Animals allocated to group 3 (
After a training period of 3 days, the performance 1 day before MCAO was taken as baseline value. The ladder rung test was performed 2, 4, 28, 42, and 56 days after experimental stroke while mNSS and beam walk test were carried out 2, 7, 12, 20, 27, 34, 40, 47, 55, and 63 days post MCAO. All behavioral tests were conducted at the same time (6 pm) and location by an investigator masked to group allocation.
Magnetic Resonance Imaging
Magnetic resonance imaging measurements of the ischemic lesion were performed at a clinical 1.5 T scanner (Gyroscan Intera human whole-body spectrometer equipped with a 47 mm loop RF-Coil, Philips, Hamburg, Germany) 1, 8, 29, and 60 days post MCAO in all animals assigned to group 3 (
Statistical Analysis
All data are shown as mean±s.d. SigmaPlot 11.0 (Systat Software, San Jose, CA, USA) was used for statistical analysis. To address the response to HUCB MNC treatment over the entire observation period data from behavioral tests was summarized as area under the curve analysis integrating all times points from day 2. Area under the curve data were analyzed for normality by Shapiro Wilk test. Afterwards, an unpaired
RESULTS
Mortality and Group Heterogeneity
Three animals died during the induction of the MCAO and two rats were later excluded because of the absence of an ischemic lesion on MRI. These animals were immediately replaced by new subjects that were randomly allocated to the experimental groups, but have not been part of the initial study population.
Treatment with Human Umbilical Cord Blood Mononuclear Cells Does Not Induce a Growth-Promoting Milieu in Spontaneously Hypertensive Rats up to 48 hours after Stroke
In order to investigate whether HUCB MNC transplantation influences the expression of endogenous growth factors in the ischemic border zone, mRNA levels of four trophic factors were compared with vehicle-treated rats at 36 hours and 48 hours after stroke injury. Earlier time points were additionally examined to determine the intrinsic neurotrophic activity after cerebral ischemia.
The ischemic stimulus led to an early increase of BDNF mRNA expression in the ischemic border zone with the highest level 6 hours after stroke, followed by a rapid decline (Figure 2A, one-way ANOVA,
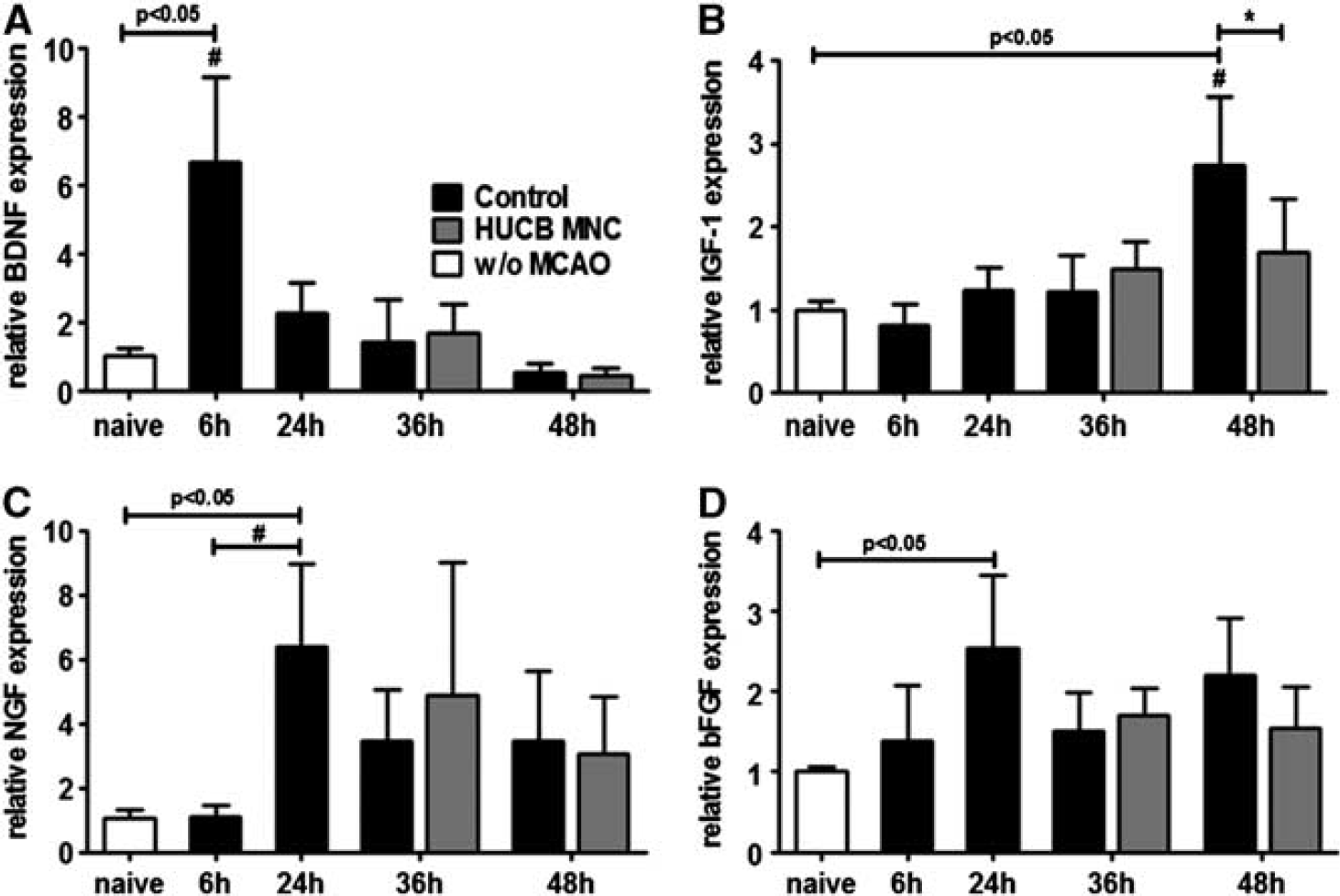
Growth factor expression after middle cerebral artery occlusion (MCAO) is not beneficially altered by human umbilical cord blood (HUCB) mononuclear cells (MNC) treatment. Growth factor expression was investigated in the infarct border zone of control and HUCB MNC-treated rats. While brain-derived neurotrophic factor (BDNF) expression increased 6 hours after MCAO in the control group (
Treatment with Human Umbilical Cord Blood Mononuclear Cells Does Not Influence Reactive astrogliosis in Spontaneously Hypertensive Rats
To evaluate the effects of HUCB MNC transplantation on reactive astrogliosis, brain samples were analyzed for mRNA expression of GFAP and Nestin. Levels of GFAP mRNA in the infarct border zone successively increased within the first 48 hours after stroke induction (Figure 3A, one-way ANOVA,
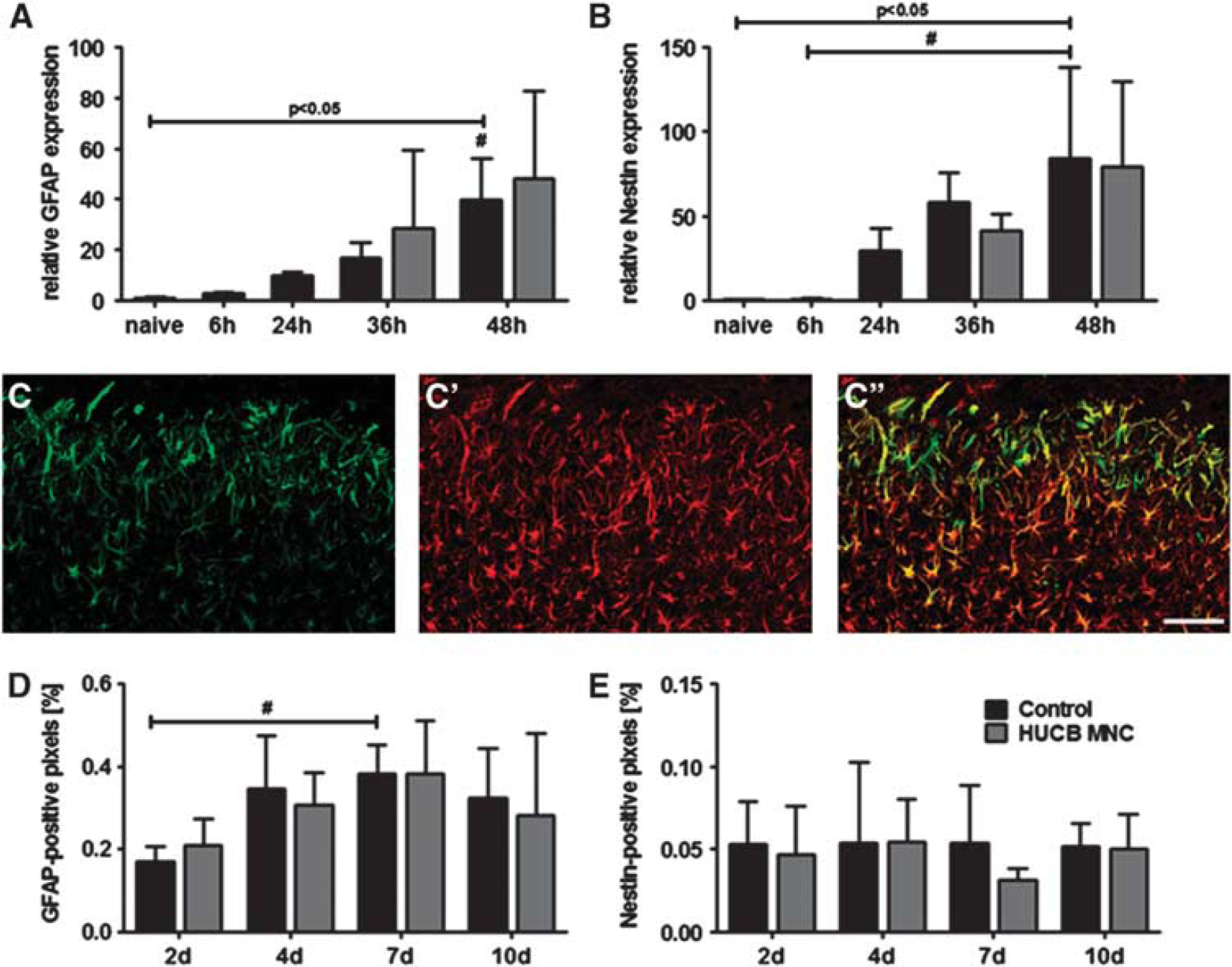
Human umbilical cord blood (HUCB) mononuclear cells (MNC) treatment does not influence glial scar development after stroke in spontaneously hypertensive rats. Relative messenger RNA expression of glial fibrillary acidic protein (GFAP) (
Likewise, no differences were found at GFAP and Nestin protein levels among both experimental groups. Morphologically, a dense meshwork of GFAP and Nestin-positive cells was present in the ischemic hemisphere already 2 days after MCAO (Figure 3C′′). The distribution of the GFAP signal differed from that of Nestin-positive cells. Whereas Nestin immunoreactivity was predominantly located in the ischemic border zone (Figure 3C), GFAP expression was more evenly distributed among the ischemic lesion (Figure 3C′). Quantitative analysis of marker expression revealed that the GFAP immunoreactive volume significantly increased over time in the infarct border zone. However, the GFAP volume did not change time-dependently as a consequence of treatment (Figure 3D, two-way ANOVA, factor ‘time’
Treatment with Human Umbilical Cord Blood Mononuclear Cells Does Not influence Motor Recovery and Infarct Volume in Spontaneously Hypertensive Rats
To investigate the therapeutic effects of HUCB MNC on stroke recovery in SH rats, a long-term experiment combining serial behavioral phenotyping by three tests and repeated measurement of the infarct volume as well as the space-occupying effect by MRI was performed (group 3). Compared with baseline values the ladder rung test showed a 2.1-fold increase of gait errors 2 days after induction of MCAO in the control group versus a 2.5-fold rise in the HUCB MNC-treated group (Figure 4A). The frequency of gait errors returned to basic values after 4 weeks in both experimental groups and then remained stable until the end of the experiment (day 56: HUCB MNC 0.052±0.031 versus control 0.056±0.036). The cumulated error rate over time did not significantly differ between the HUCB MNC-treated rats and the control group (Figure 4B,
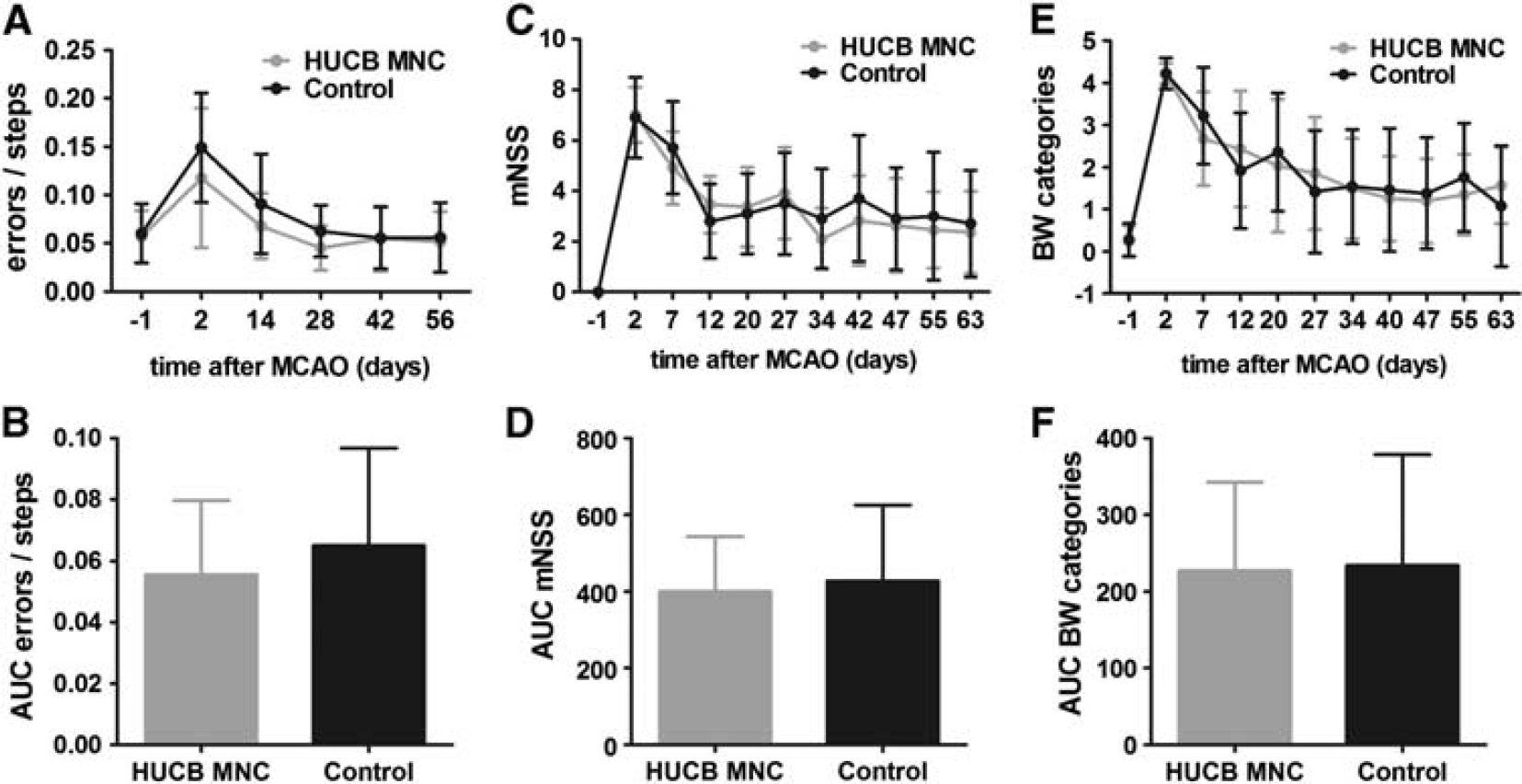
Human umbilical cord blood (HUCB) mononuclear cells (MNC) transplantation does not exert amelioration of functional deficits after ischemic stroke. Development of functional deficits measured by ladder rung test (
A typical depiction of the ischemic lesion and its development were seen in all animals subjected to MCAO. Exemplary examples are given in Figure 5A. The mean infarct volume as percentage of the ipsilateral hemisphere corrected for edema (%HLVe) did not significantly differ among both groups up to 60 days after stroke corroborating the absent therapeutic effect of HUCB MNC transplantation (two-way ANOVA-RM, time × treatment
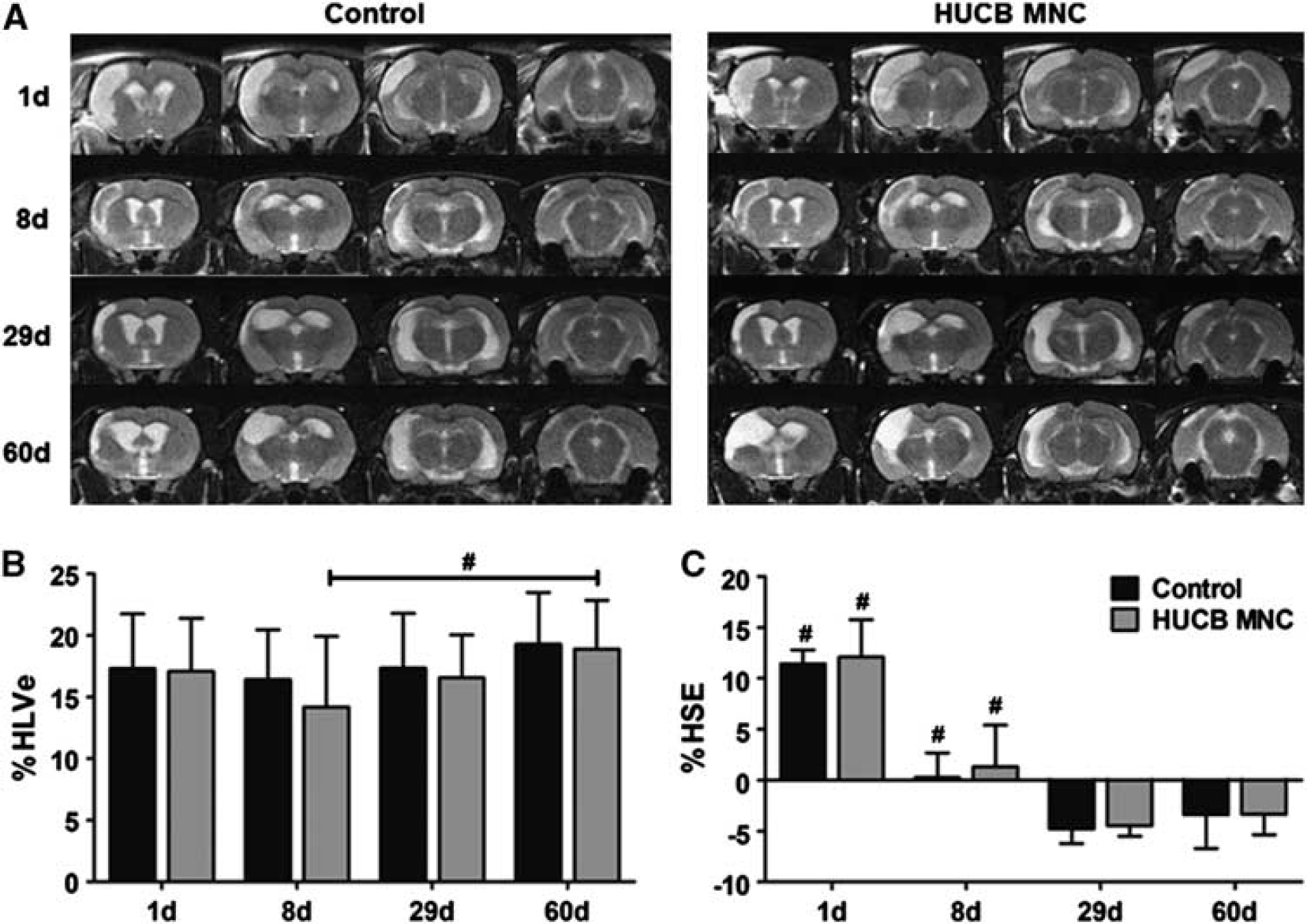
Development of ischemic lesion volume and space-occupying effect on T2-w magnetic resonance imaging (MRI) in the control and human umbilical cord blood (HUCB) mononuclear cells (MNC)-treated group. (
The space-occupying effect of the ischemic lesion expressed as volume change of the affected hemisphere (%HSE) expectedly was most pronounced at the first day after MCAO and almost vanished until day 8 in both experimental groups (Figure 5C, HUCB MNC 1.3%±4.1% versus control 0.3%±2.4%). At later time points, %HSE attained negative values (Figure 5C; day 60 HUCB MNC −3.4%±2.0% versus control −3.4%±3.3%), indicative of secondary atrophy of the ischemic hemisphere. Volume changes of the ischemic hemisphere either provoked by brain edema in the early phase or by shrinkage in the late stage were not significantly influenced by HUCB MNC treatment (two-way repeated measures ANOVA, time × treatment
DISCUSSION
In this study, we aimed to investigate whether cryopreserved HUCB MNC transplantation 24 hours after focal cerebral ischemia has sustained impact on recovery in SHR. Long-term functional outcome as assessed by three behavioral tests as well as lesion development and hemispheric atrophy on MRI were not beneficially influenced by cord blood cell therapy. Furthermore, HUCB MNC treatment neither did relevantly change host-derived mRNA levels of various growth factors in the infarct border zone early after stroke nor did it affect the extent of glial scarring.
As delayed administration was shown to be efficient in several preclinical trials, 22 HUCB MNC are assumed not only to prevent damage, but also to promote neurorestorative effects after stroke injury. From a mechanistic perspective, cell-based therapies might amplify endogenous processes of brain plasticity as well as vascular regeneration and recruitment of progenitor cells. 23 While the regulation of ischemia-induced neurogenesis is poorly understood, various growth factors are known to be implicated in precursor cell proliferation in the subventricular zone as well as in chemotaxis toward the sites of injury and survival of neuroblasts in the ischemic border zone. 24 In this context, the ability of HUCB MNC to increase local growth factor levels after stroke, either by direct secretion or by inducing host expression, 9 is supposed to be a major mediator of the reported beneficial effects. In this study, we found a rapid increase of endogenous BDNF, nerve growth factor, and basic fibroblast growth factor mRNA after the ischemic injury; however, HUCB MNC treatment did not further augment these levels within 48 hours after stroke. To our surprise, local IGF-1 mRNA expression was yet decreased in HUCB MNC-treated rats early after stroke. Considering the previously described neuroprotective properties of IGF-1, 25 this finding implies a rather detrimental, although functionally irrelevant effect of HUCB MNC transplantation. Insulin-like growth factor 1 expression after stroke is largely ascribed to subpopulation of infiltrating macrophages. 26 As experimental evidence suggests that HUCB MNC treatment diminishes leukocyte migration to the ischemic brain, 7 one might speculate that lower IGF-1 mRNA levels in HUCB MNC-treated rats result from changes of the poststroke immune response. However, inflammatory mechanisms were clearly beyond the scope of the present study and thus not further investigated.
In the time frame analyzed here (up to 10 days after the onset of stroke), astrogliosis is considered a primarily protective process. First, the dense meshwork of GFAP and Nestin-positive reactive astrocytes in the infarct border zone prevents dispersion of deleterious processes to the surrounding tissue. Additionally, reactive astrocytes were shown to contribute to a regenerative microenvironment adjacent to the lesion, thereby promoting synapto- and neurogenesis as well as the repair of the blood–brain barrier. 11 However, in line with our primary and secondary endpoints, we did not observe a significant impact of HUCB MNC transplantation on astroglial scarring.
As a potential limitation of our study, primer pairs used for PCR analysis only recognized rodent mRNA. Thus, direct release of human neurotrophins by cord blood cells as shown in
Functional deficits after ischemic stroke are predominantly assessed by simple reflex tests during the early phase of infarction. In the present study, we applied a combination of three behavioral tests to provide a more comprehensive picture of the motor capacity of SHR after MCAO. Besides the modified neurologic severity score (mNSS) the beam walk test measuring hindlimb function as well as the ladder rung test for fore- and hindlimb stepping and interlimb coordination were used. Furthermore, we performed a long-term followup of functional recovery up to 2 months after stroke to discern sustained benefits from a mere delay in the appearance of deficits. Chronic behavioral testing, though rarely performed, is considered especially critical when brain plasticity is therapeutically addressed. 30 However, while there was a long-term recovery in both experimental groups neither its course nor the cumulative degree of impairment was substantially affected by HUCB MNC treatment.
In the present study, untreated SHR rapidly developed a stabilized ischemic lesion without relevant infarct expansion over 60 days. This was previously ascribed to the poor collateral flow in this model. 31 Interestingly, we found a delayed increase of the lesion volume from day 8 to day 60 in rats treated with HUCB MNC, possibly providing evidence for transient beneficial effects on the lesion size. However, cord blood therapy had no significant impact on lesion volume as well as on hemispheric atrophy 60 days after MCAO. This corroborates the functional data that failed to prove any sustained influence of HUCB MNC treatment on poststroke recovery. Only few studies addressed late-stage volume changes on MRI as outcome parameter despite the fact that cerebral atrophy is considered a common feature in the chronic phase of stroke. 32 Instead, most experimental stroke studies focus on changes of the infarct volume as a measure of treatment efficacy even though attempts to correlate behavioral tests and infarct volume often failed in the past. 33 Apart from the primary lesion, diffuse neuronal death in areas remote from the lesion, diaschisis, and metabolic changes might also contribute to poorer outcome in the chronic stage stroke, 34 underlining the need for more sophisticated structural MRI analysis.
The results of this study are in clear contrast with previously reported findings from our 3 and other groups6, 28 that indicated a noticeable benefit of experimental HUCB MNC transplantation after stroke. However, next to a considerable body of indications corroborating the therapeutic efficacy of HUCB MNC after stroke, some investigators were unable to reproduce therapeutic findings, especially when applying more demanding functional tests as in the present study. 13 Furthermore, differences in cell storage and processing may potentially impair the efficacy of the treatment. In fact, while we recently failed to detect neuroprotective effects of cryopreserved HUCB MNC early after MCAO, 17 previous studies reporting beneficial results were generally conducted with freshly isolated HUCB MNC.4, 6, 10
Human umbilical cord blood preservation techniques have originally been introduced to create a valuable source of hematopoietic stem and progenitor cells being capable of repopulating the hematopoietic system after treatment of devastating malignancies, but also to replenish bone marrow stocks. Consequently, studies assessing the effects of HUCB cryopreservation exclusively focused on the hematopoietic potential of the cells. Albeit this was found unaffected in most studies, the use of dimethyl sulfoxide as a cryoprotectant or non-automated, slow-cooling techniques, both being common in experimental studies, can cause a significant decrease in viable cell yields after thawing. 35 This effect is particularly prominent for CD34+ hematopoietic progenitor cells. 15 Loss of CD34+ cells was even reported when applying automated cooling techniques according to industrial good manufacturing practice standards. 36 Though not being the only effector cell population within HUCB MNC, CD34+ are supposed to exert neuroprotective as well as regenerative capabilities and are further discussed to have an important role during the early phase of HUCB MNC stroke therapy.3, 37 A higher number of circulating CD34+ cells was also associated with improved functional outcome in human stroke patients. 38 Given the supposed relevance of this population among the transplant, it is important to consider that most studies reporting a distinct therapeutic effect after application of cryopreserved HUCB MNC samples relied on preparations with increased CD34+ content of up to 70%. 6 Hence, a moderate loss of CD34+ cells during cryopreservation and subsequent thawing may have been compensated by the cell enrichment strategies applied. Given positive results from previous studies using freshly prepared or CD34+-enhanced HUCB MNC, the use of more informative control groups must be recommended for future studies. A direct comparison of cryopreserved HUCB MNC against these populations (positive controls) as well as freeze–thawed killed HUCB MNC rather than PBS (negative controls) is particularly rational.
Another possible and obvious explanation for the absent therapeutic impact may be the study design, which employed a xenotransplantation paradigm without an accompanying immunosuppression regime to prevent graft rejection. Immunosuppression in experimental transplantation studies is mainly achieved by application of cyclosporin A or tacrolimus, which are highly effective and widely used in common rodent models. However, both agents were shown to exert neuroprotective effects after ischemic brain injury. Moreover, cyclosporin A may also detrimentally affect poststroke recovery by enhancing the risk of convulsions in human patients and rodents. 39 We therefore decided to omit immunosuppression to prevent confounding effects on the chosen primary endpoints. However, long-term engraftment of HUCB MNC is not a prerequisite for functional improvement after MCAO 5 and sustained lesion size reduction as well as functional improvement have previously been observed after treatment with human HUCB cells in the absence of immunosuppression. 28 Hence, omission of immunosuppression alone may be considered unlikely to explain the observed lacking therapeutic impact.
The use of animals with risk factors that match the clinical stroke population such as in the present study is highly recommended for preclinical trials. 40 Although cell-based therapies using freshly prepared HUCB MNC have already been performed in SHR, pathologic hypertension and other genetically determined abnormalities in the strain may have confounded results obtained in primary and secondary endpoints, at least to some extent. For example, chronic cerebrovascular damage, 41 reduced expression of neurotrophic factors and impaired neuroneogenesis 42 as well as divergent neuroendocrine responses to distress stimuli have been reported in SHR as compared with normotensive controls. 43 The impact of these differences on poststroke functional recovery in SHR remains for further investigation.
Recent failure in translation has often been attributed to inadequate preclinical study design and severe methodological shortcomings. By contrast, this study strictly adhered to current recommendations for basic stroke trials,
40
which among others included randomization, rater-masked evaluation and full disclosure of dropout rates. Furthermore, to minimize the risk for false-negative interpretation of the results
Taken together, the results reported herein advise caution regarding a swift translation of HUCB MNC therapies for ischemic stroke into a clinical setting before achieving clarity about the precise modes of action of these cells and the possible impact of long-term cryopreservation on the neuroprotective or neurorestorative abilities of these cells. Future experimental studies should reveal the exact circumstances under which a HUCB MNC-based therapeutic approach can exert clinical benefit for human stroke patients before commencing clinical trials. Taking into account aspects of cell preparation and preservation, which have been mostly unconsidered so far, may be not only be expedient but mandatory when designing such experiments.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.