
Abstract
Hypertension is associated with cerebral small vessel disease (SVD) and with diffuse white matter hyperintensities (WMH) on T2-weighted magnetic resonance imaging (MRI). We tested whether stroke-prone spontaneously hypertensive rats (SHRSP), a model of chronic hypertension, exhibit WMH. Male SHRSP (age 10 months) without stroke symptoms were compared with age-matched male WKY rats. Stroke-prone spontaneously hypertensive rats exhibited no WMH on MRI scans (T2, T2∗, diffusion tensor imaging) and no neuropathological lesions. While leptomeningeal arteries exhibited fibrohyaline wall thickening, with decreased smooth muscle actin relative to WKY, deep penetrating arterioles within the caudate nuclei had no vasculopathy. We conclude that WMH are not an obligate feature of stroke-free SHRSP aged up to 10 months.
Keywords
INTRODUCTION
Diffuse white matter hyperintensities (WMH) are a frequent finding on T2-weighted magnetic resonance imaging (MRI) scans, especially in elderly patients.1,2 White matter hyperintensities are linked to cerebrovascular pathology such as cerebral small vessel disease (SVD), but the pathogenic mechanisms are not fully known.1,3 Age and hypertension are risk factors for both WMH and SVD.2,4
Stroke-prone spontaneously hypertensive rats (SHRSP) develop chronic, severe hypertension from 9 to 10 weeks of age5–7 with subsequent vascular pathology, reduction in cerebral perfusion, and a spectrum of spontaneous stroke lesions.5,8–11
Here, we tested the hypothesis that chronically hypertensive SHRSP develop WMH, using MRI and subsequent histopathology. We also examined leptomeningeal arteries and deep penetrating arterioles for SVD-like vasculopathy.8,10 Most prior MRI studies have used young adult SHRSP, often fed a sodium-rich diet to precipitate stroke events. 8 There are few studies of older, non-salt loaded SHRSP before stroke onset, with conflicting results with regard to white matter pathology. 8 Here, we studied male SHRSP (to avoid confounding effects of female reproductive hormones) with normal diet, and without stroke symptoms. Rats were studied at age 10 months, as above this age stroke incidence and mortality increase markedly.6,7,12
MATERIALS AND METHODS
Male SHRSP aged 10 months (range 45 to 48 weeks; n = 9) and male WKY rats (44 to 49 weeks; n = 6) underwent MRI (T2, T2*, and DTI (diffusion tensor imaging)) on a Bruker Biospec 7 T/30 cm system (Wikingerstrasse, Karlsruhe, Germany) with gradient coil (121 mm ID, 400 mT/m) and 72 mm birdcage resonator. Diffusion tensor imaging was carried out with a four shot spin echo planar imaging sequence for assessment of white matter. Mean diffusivity (MD) and fractional anisotropy (FA) in corpus callosum and the caudate nuclei were computed, as described in the Supplementary File.
All animals included in this study had no stroke symptoms (defined here as: inactivity and lethargy; hunched appearance; piloerection; uncoordinated movements; loss of weight, and appetite). Rats were anesthetized with isoflurane in a mixture of N2O/O2 (70/30). All procedures were approved by the University of Glasgow Ethical Review Panel and complied with the Animals (Scientific Procedures) Act 1986. This report was prepared following consideration of the ARRIVE guidelines (http://www.nc3rs.org.uk/arrive).
While still anesthetized, rats were transcardially perfused with heparinized saline followed by 4% paraformaldehyde. Adjacent coronal sections (10 μm) underwent histological staining (n = 9 SHRSP; n = 6 WKY) with hematoxylin and eosin (H&E), or with Luxol fast blue counterstained with cresyl violet (LFB-CV), or elastic Van Gieson (EVG) stain, or immunohistochemical labeling for smooth muscle α-actin (SMA), myelin basic protein (MBP), or the oligodendrocyte marker Olig2. Immunolabeling was visualized using diaminobenzidine chromagen (Envision kit, Dako, Ely, UK), counterstained with hematoxylin.
Further details on all Materials and methods are given in the Supplementary appendix.
RESULTS
Magnetic Resonance Imaging Data
Magnetic resonance imaging scans confirmed the absence of stroke lesions in SHRSP (n = 9). On T2-weighted scans, no WMH were seen in white matter areas (corpus callosum, internal capsule, and external capsule) in SHRSP (Figure 1; Supplementary Figure S1) or WKY (not shown). Analysis of FA and MD on DTI scans revealed no evidence for white matter damage in SHRSP (Table 1). Stroke-prone spontaneously hypertensive rats displayed modest reduction in MD within the corpus callosum (14%) and the caudate nuclei (4%) and increase in FA in the corpus callosum (6%) relative to WKY (Table 1). Strokeprone spontaneously hypertensive rats (Figure 1; Supplementary Figure S1) and WKY (not shown) demonstrated no evidence of hemorrhage on gradient-echo T2* scans or T2-weighted images. For the T2* sequence the in-plane resolution is 0.260 mm, so the area of one voxel is 0.26 × 0.26 = 0.0676 mm2, with a slice thickness of 1.5 mm. The smallest detectable hemorrhage would be ~4 voxels, that is, 0.5 × 0.5 × 1.5 mm3.
Diffusion tensor imaging and morphometric data for SHRSP and WKY
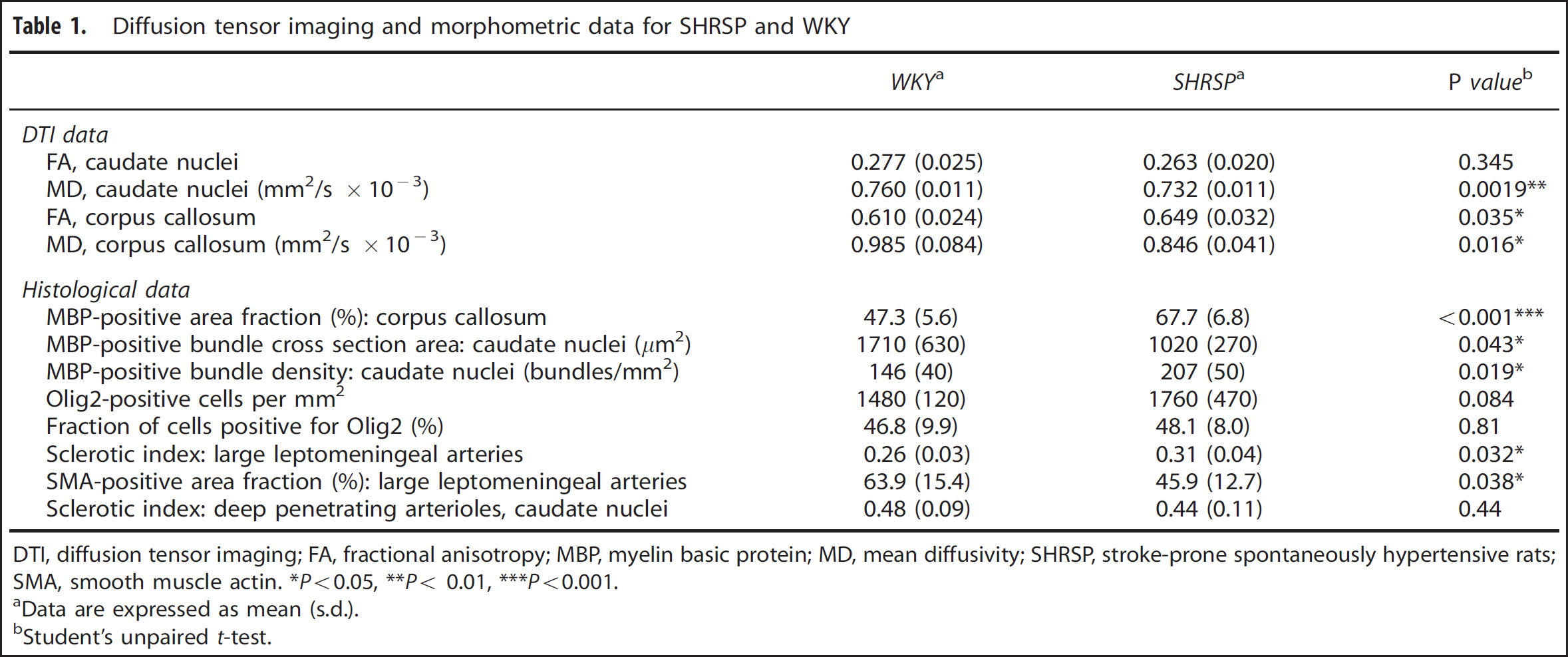
DTI, diffusion tensor imaging; FA, fractional anisotropy; MBP, myelin basic protein; MD, mean diffusivity; SHRSP, stroke-prone spontaneously hypertensive rats; SMA, smooth muscle actin.
P<0.05,
P< 0.01,
P<0.001.
Data are expressed as mean (s.d.).
Student's unpaired t-test.
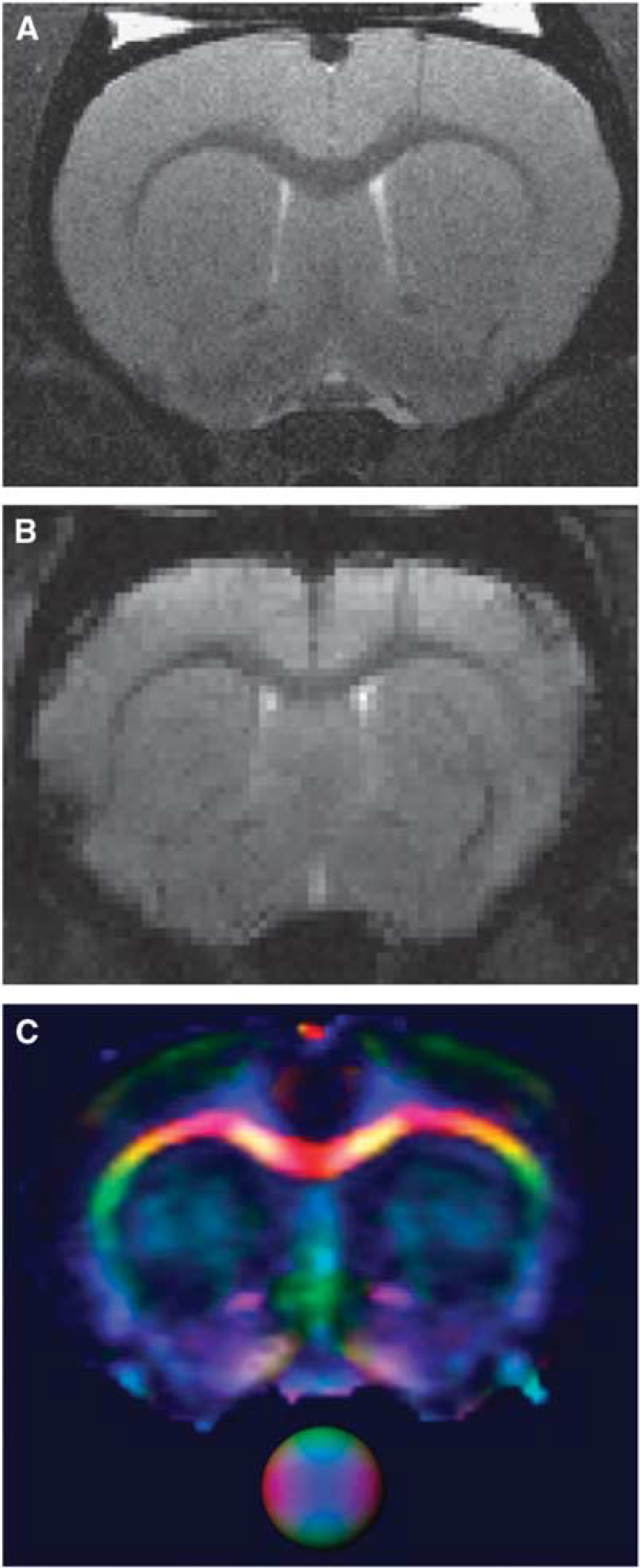
Magnetic resonance imaging (MRI) scans of stroke-free stroke-prone spontaneously hypertensive rats (SHRSP) brain. MRI scans (coronal section) from a representative male SHRSP aged 48 weeks. T2-weighted (
Histopathology and Morphometry
Blinded examination of H-E and LFB-CV-stained histological sections by a registered neuropathologist (LRB) revealed no evidence of the following in SHRSP (n = 9): vacuolation in corpus callosum or caudate white matter bundles; astrocytosis; microinfarcts; fibrinoid necrosis of vessel walls; microhemorrhage; macrophage invasion. Robust, uniform MBP immunolabeling was seen in corpus callosum and in caudate white matter bundles of SHRSP (Figure 2).
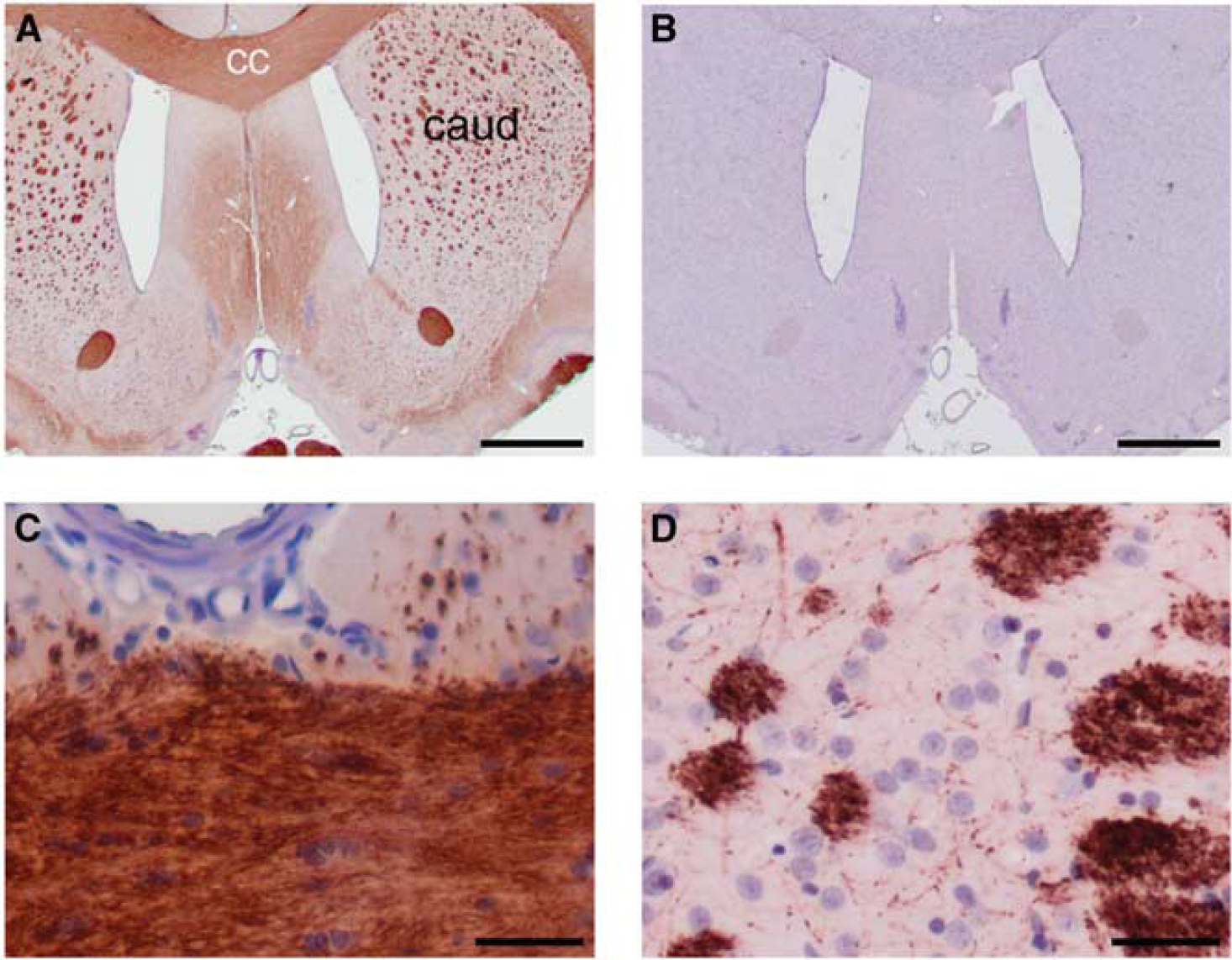
Histological examination of white matter. Immunohistochemical labeling of myelin basic protein (MBP) in brain sections from a representative stroke-prone spontaneously hypertensive rat (SHRSP), aged 47 weeks. (
Morphometric analysis of MBP and Olig2 labeling showed no white matter damage in corpus callosum or in caudate white matter bundles of SHRSP (n = 9, Figure 2; Supplementary Figure S2) or WKY (n = 6; Table 1). Stroke-prone spontaneously hypertensive rats had somewhat greater MBP-positive area density (1.4-fold) in the corpus callosum relative to WKY (Table 1). In the caudate nuclei, SHRSP had greater density of MBP-positive bundles (1.4-fold) and lower bundle density (0.59-fold; Table 1). Within corpus callosum, the area density and cell fraction of Olig2-positive cells did not differ between SHRSP and WKY (Table 1; Supplementary Figure S2).
Leptomeningeal arteries in SHRSP exhibited thickened, hyalinized walls with abnormal SMA labeling in myocytes (Supplementary Figure S3), while WKY rats had uniform medial SMA labeling in equivalent vessels, without hyalinosis (Supplementary Figure S3). Leptomeningeal arteries in SHRSP exhibited elevated sclerotic index (SI) relative to WKY (1.2-fold; Table 1) and reduced SMA-positive area fraction (0.72-fold; Table 1) relative to WKY. The SI of penetrating SMA-labeled vessels (assumed to be deep penetrating arterioles) in the caudate nuclei did not differ between groups (Table 1; Supplementary Figure S3).
DISCUSSION
White matter hyperintensities are commonly seen on clinical T2-weighted MRI scans and their prevalence and extent increase with advancing age and cardiovascular risk factors, particularly hypertension.2,4 More confluent WMH, especially those in deep white matter sites, are associated with SVD. 2 In DTI scans of human subjects, WMH exhibit elevated MD and reduced FA, interpreted as loss of axons and myelin structure.2,13,14 Neuropathological features of WMH are demyelination, cell and axonal atrophy, and gliosis, accompanied by fibrinohyalinotic changes and vessel wall thickening in deep penetrating arteries.1–3
Our MRI data suggest that WMH do not accompany chronic hypertension in stroke-free SHRSP at age 10 months. Our histological data supported these findings, with no depletion of MBP or loss of oligodendrocytes. Previous MRI studies of SHRSP have used high salt diet to augment hypertension and stroke likelihood.8,15,16 In agreement with our findings, other groups found no changes on T2-weighted scans of stroke-free SHRSP on normal diet at 5–8 months of age.11,16 Some prior MRI studies included stroke-free SHRSP above this age and, in agreement with our data, these showed no WMH.9,15 Some previous histological studies reported white matter lesions in non-salt loaded SHRSP 17 while others, including ourselves, found no white matter damage.16,18
Contrary to our hypothesis, SHRSP exhibited reduced MD in the corpus callosum and caudate nuclei relative to WKY, and the corpus callosum displayed elevated FA (Table 1), indicative of increased white matter structure. This was corroborated by increased MBP in the corpus callosum (Table 1). These paradoxical findings may be a response to chronic hypoperfusion in the white matter of SHRSP. 9 Changes in myelination occur more rapidly in rodent brain than in humans.19–21
Leptomeningeal arteries of SHRSP exhibited fibrohyaline thickening and loss of cellularity, confirmed by increased SI and decreased SMA-positive area (Table 1), in accord with the chronic hypertensive phenotype of SHRSP.6,8 As with our findings, earlier morphometric analyses observed arterial thickening in large leptomeningeal vessels of SHRSP relative to WKY.22,23 We saw no wall thickening in deep penetrating arterioles, and no erythrocyte accumulation in deep brain vessels. 11
There are several limitations of our study. First, the SI parameter does not encompass all aspects of SVD arteriopathy. It is an approximate measure of arterial or arteriolar stenosis at single-vessel level, for neuropathological reporting of SVD.24,25 Second, the Glasgow SHRSP colony used here may have undergone some genotypic shift from the Japanese founder colony. 7 However, they exhibited characteristic coat coloration associated with SHRSP, and leptomeningeal arterial thickening indicative of chronic hypertension. Third, our data do not exclude WMH in SHRSP that survive beyond 10 months. Notch3R169C transgenic mice accumulate arterial collagen from age 5 months, but white matter lesions only at age 18–20 months. 26 These Notch3R169C mice are not hypertensive or stroke-prone. 26
It should be emphasized that the SHRSP studied here are a selected population, free from stroke symptoms. Incidence of stroke in the Glasgow SHRSP colony is ~70% at 9 months of age, which accords with incidence in other groups.6,9,11,12 In detailed studies of lifespan by another group, survival of untreated male SHRSP was 100% at 9 months of age, 50% at 13 months, with mortality complete at 15 months.6,12 Stroke and mortality were seen considerably earlier in original reports from the Kyoto founder colony, with average lifespan of 276 days (~9 months) and 89% stroke incidence (n = 60/67).5,7 It seems likely that there are some differences in pathology and stroke incidence between the founder colony and the other colonies that have been established. There may also be an effect of different husbandry regimes and different criteria for selection of breeding pairs.
In conclusion, SHRSP which were stroke-free at age 10 months exhibited fibrohyaline changes in leptomeningeal arteries, but no vasculopathy in deep penetrating arterioles, and no WMH. Our data do not support the hypothesis that stroke-free SHRSP develop WMH, and suggest that WMH do not necessarily accompany chronic hypertension over the timescale studied.
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.