
Abstract
Although treatment of stroke patients with mild hypothermia is a promising therapeutic approach, chemicals inducing prompt and safe reduction of body temperature are an unmet need. We measured the effects of the transient receptor potential vanilloid-1 (TRPV1) agonist rinvanil on thermoregulation and ischemic brain injury in mice. Intraperitoneal or intracerebroventricular injection of rinvanil induces mild hypothermia that is prevented by the receptor antagonist capsazepine. Both intraischemic and postischemic treatments provide permanent neuroprotection in animals subjected to transient middle cerebral artery occlusion (MCAo), an effect lost in mice artificially kept normothermic. Data indicate that TRPV1 receptor agonists are promising candidates for hypothermic treatment of stroke.
Introduction
Hypothermia is among the most powerful neuroprotective strategies identified so far (Diller and Zhu, 2009). Intraischemic hypothermia reduces infarct volumes and improves neurologic outcome in different models of brain ischemia. Delayed (2–3 hours) hypothermia also reduces ischemic brain injury provided that the duration of cooling lasts up to several hours. On the clinical side, induction of hypothermia in stroke patients proved safe, although its efficacy is unclear and needs confirmation by additional clinical trials (Yenari and Hemmen, 2010). Uncertainties also exist about depth, time to treatment and duration of hypothermia, as well as efficacious methods of cooling (van der Worp et al, 2010). Because few molecules are able to reduce body temperature (Tb) to an extend consistent with neuroprotective hypothermia (such as neurotensin, 3-iodithyronamine, and hydrogen sulfide), there is enormous interest in identifying drugs able to readily and safely reduce Tb (Yenari and Hemmen, 2010; van der Worp et al, 2010). Interestingly, transient receptor potential vanilloid-1 (TRPV1) activation, besides transducing sensory stimuli, also negatively regulates Tb (Gavva, 2008; Fosgerau et al, 2010). Given that no studies exploited this hypothermic activity for neuroprotection, here we studied the effects of rinvanil, a potent TRPV1 agonist (Appendino et al, 2005), on Tb and ischemic brain injury in mice.
Materials and methods
All the experiments conducted were performed according to the Italian guidelines for animal care (DL 116/92) in application of the European Communities Council Directive (86/609/EEC) and were formally approved by the Animal Care Committee of the Department of Pharmacology of the University of Florence. C57Bl/6 male mice (Harlan, Udine, Italy) were used. Rinvanil (synthesized as reported; Appendino et al, 2005) or capsazepine (Tocris, Minneapolis, MN, USA) was dissolved in dimethyl sulfoxide (DMSO) and injected intraperitoneally at the indicated doses. Tb and skin temperature was measured by means of a rectal or skin probe (Harvard Apparatus, Holliston, MA, USA). Because pilot experiments showed that rectal and temporalis muscle temperature similarly decreased on rinvanil treatment, the rectal probe was routinely used to measure Tb in mice. O2 consumption rate was obtained by means of a closed respirometer (Columbus Instruments, Columbus, OH, USA). Middle cerebral artery occlusion (MCAo) was conducted as reported (Eliasson et al, 1997) and the filament withdrawn after 60 or 90 minutes. Mice (
Results
Effects of Rinvanil on Body Temperature Regulation
Given the effects of various capsacinoids on thermoregulation (Gavva, 2008), we first investigated whether the TRPV1 receptor agonist rinvanil also affects Tb. At 25 mg/kg, animals reached a Tb of 33.4±0.6°C 30 minutes after the injection (Figure 1A), and returned to control values after 2.2±0.3 hours. Higher doses prompted similar hypothermia after 30 minutes (33.2±3°C at 50 mg/kg and 32.5±5°C at 100 mg/kg) but for longer time lengths (4.4±0.3 and 4.9±0.5 hours at 50 or 100 mg/kg, respectively). Prior work suggests that hypothermia induced by capsaicin analogs is due to activation of peripheral TRPV1 receptor (Gavva, 2008; Fosgerau et al, 2010). However, we found that intracerebroventricular injections of rinvanil also reduced Tb dose dependently (Figure 1B). Notably, hypothermia induced by 25 mg/kg rinvanil intraperitoneally was reduced by a concomitant intracerebroventricular injection of the TRPV1 antagonist capsazepine (50 μg; Figure 1C). The inhibiting effects of capsazepine were surmountable by increasing the dose of rinvanil (Figure 1D), indicating competitive inhibition. To gather information on the mechanisms through which rinvanil alters thermoregulation, we analyzed O2 consumption and skin temperature as indexes of basal metabolism and vascular tone, respectively. We found that rinvanil reduced both O2 consumption and skin temperature (Figures 1E and 1F).
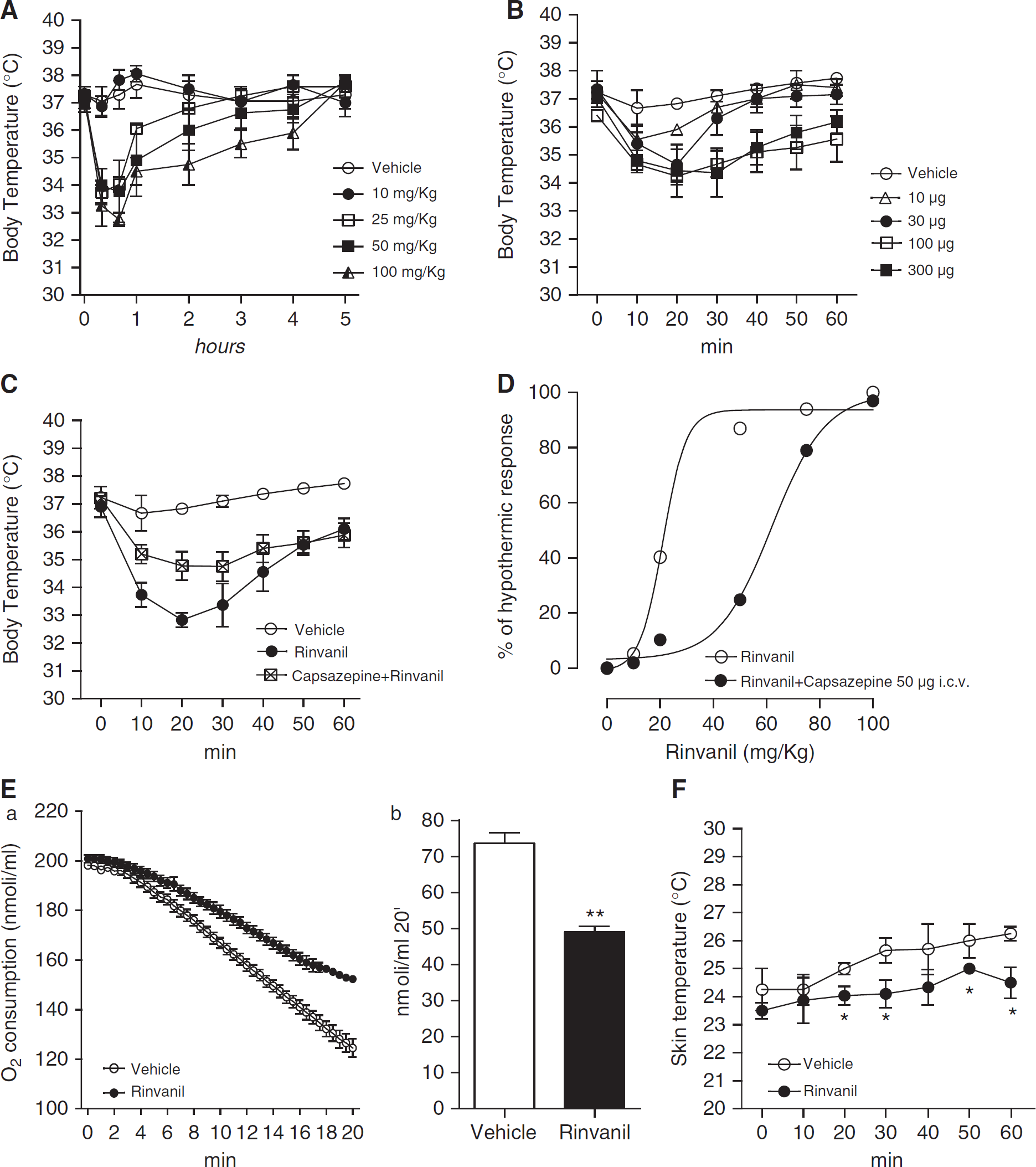
Effect of rinvanil on thermoregulation. Effect of intraperitoneal (
Effects of Rinvanil on Brain Ischemia-Reperfusion Injury
To evaluate whether rinvanil-dependent TRPV1 receptor activation prompts neuroprotective hypothermia during brain ischemia, we assessed compound's effects in mice subjected to transient MCAo. As shown in Figure 2A, hypothermia induced by rinvanil (25 mg/kg) in mice subjected to 1 hour MCAo was similar to that induced in sham-operated mice but lasted longer (6.5±0.8 and 2.5±0.2 hours; respectively. Figure 2A and not shown), indicating that brain ischemia sensitizes animals to TRPV1 receptor-induced hypothermia. However, rinvanil injections did not alter physiological parameters such as blood pressure, Pa
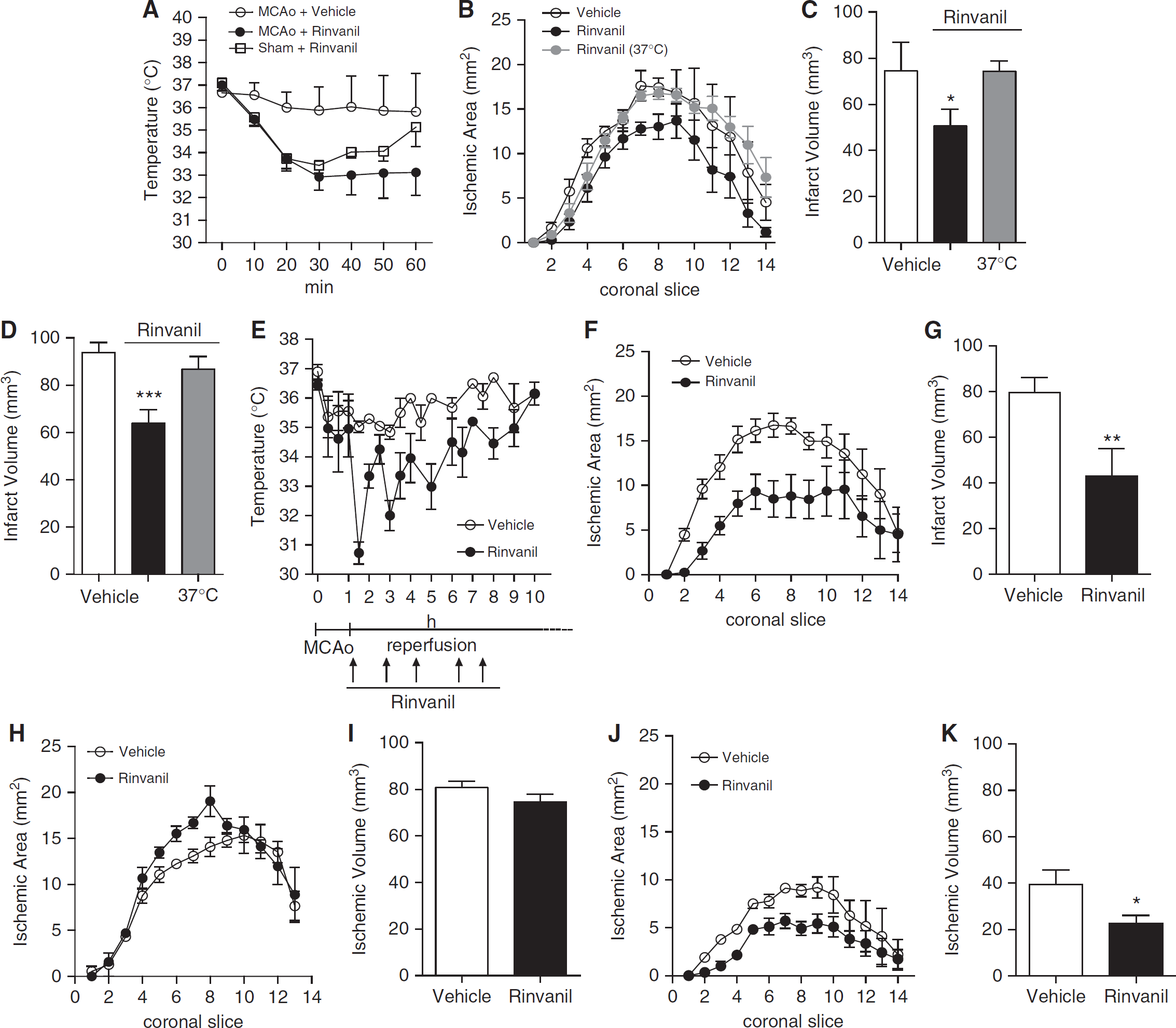
Effects of rinvanil on ischemic brain injury in mice. (
In keeping with ischemic neuroprotection by hypothermia, infarct volumes of mice subjected to 1 hour MCAo/24 hours reperfusion were significantly reduced by 25 mg/kg rinvanil (74±12 in DMSO-treated mice and 49±8 mm3 in rinvanil-treated mice;
It is well appreciated that activation of TRPV1 receptors causes large increases of intracellular Ca2+ concentrations in neurons. Consistently, massive receptor activation prompts neuronal death
Discussion
Hypothermia is a robust protectant against experimental ischemic brain injury, even though its clinical relevance needs additional trial to establish efficacy. Pilot studies have clearly indicated that, among the various parameters and variables to be considered, fast cooling of patients is a key for clinical efficacy (Yenari and Hemmen, 2010; van der Worp et al, 2010). In this light, there is ample agreement that drugs able to readily and safely reduce Tb are an unmet need. In the present paper, we show that the potent TRPV1 receptor agonist rinvanil readily induces hypothermia dose dependently acting within the CNS in a capsazepine-sensitive manner. Evidence that the hypothermic effect correlates with ischemic neuroprotection suggests that TRPV1 targeting can be exploited for hypothermic treatment of stroke.
Data are in line with hyperthermia induced by drugs blocking tonic activation of TRPV1 receptors (Gavva, 2008). In this regard, it has been reported that TRPV1-dependent thermoregulation is due to modulation of receptors outside the blood–brain barrier, more precisely those tonically activated in the viscera (Gavva et al, 2007). Our results on the effect of intracerebroventricular injection of rinvanil, however, indicate that central agonism on TRPV1 receptors suffices to induce hypothermia. Of note, although this is in keeping with the complex effects of capsaicin on hypothalamic thermosensitive neurons (Hori, 1984; Hori et al, 1988), the exact localization of TRPV1 receptors within the rodent and human hypothalamus is still debated (Menigoz and Boudes, 2011). Reportedly, peripheral TRPV1 receptors tonically suppress cold defenses by inhibiting thermogenesis and skin vasoconstriction (Gavva, 2008). Although we confirmed that TRPV1 receptor activation reduces O2 consumption (an index of thermogenesis), we found that, rather than vasodilatation, TRPV1 agonism causes skin vasoconstriction. The latter might be a cold defense response due to hypothermia. Alternatively, hypothermia due to central TRPV1 receptor activation might activate autonomic responses partially different from those set into motion by blocking tonically active peripheral TRPV1 receptors. Regardless, the present study qualifies TRPV1 receptor agonists as promising drugs for hypothermic neuroprotection. The finding that reduction of ischemic brain injury also occurs when rinvanil is used in a postischemic treatment paradigm further emphasizes its therapeutic potential. The latter, however, might be reduced because of TRPV1 receptor desensitization after repetitive injections (Figure 2E), or because of the neurotoxic effects originating from excessive activation of TRPV1 receptors and ensuing massive intracellular Ca2+ entrance (Kim et al, 2005; Shirakawa et al, 2008).
In conclusion, in light of the urgent need of hypothermic drugs for clinical trial in stroke patients, our findings suggest that hypothermia due to TRPV1 receptor activation can be exploited for innovative stroke treatments. Also, because of the relevance of hypothermia to cardiac arrest or neonatal hypoxia, the cooling affects of rinvanil-like drugs might be harnessed for additional therapeutic strategies.
Footnotes
Disclosure/conflict of interest
The authors declare no conflict of interest.