
Abstract
To elucidate the dynamic effects of deep brain stimulation (DBS) in the subthalamic nucleus (STN) during activity on the dopaminergic system, 12 PD patients who had STN-DBS operations at least 1 month prior, underwent two positron emission tomography scans during right-foot movement in DBS-off and DBS-on conditions. To quantify motor performance changes, the motion speed and mobility angle of the foot at the ankle were measured twice. Estimations of the binding potential of [11C]raclopride (BPND) were based on the Logan plot method. Significant motor recovery was found in the DBS-on condition. The STN-DBS during exercise significantly reduced the [11C]raclopride BPND in the caudate and the nucleus accumbens (NA), but not in the dorsal or ventral putamen. The magnitude of dopamine release in the NA correlated negatively with the magnitude of motor load, indicating that STN-DBS facilitated motor behavior more smoothly and at less expense to dopamine neurons in the region. The lack of dopamine release in the putamen and the significant dopamine release in the ventromedial striatum by STN-DBS during exercise indicated dopaminergic activation occurring in the motivational circuit during action, suggesting a compensatory functional activation of the motor loop from the nonmotor to the motor loop system.
Keywords
INTRODUCTION
Deep brain stimulation (DBS) of the subthalamic nucleus (STN) is effective in ameliorating the motor symptoms of patients with Parkinson's disease (PD), 1 but the neurophysiologic mechanisms of STN-DBS are still unclear. Previous studies have shown that STN stimulation causes negligible amounts of dopamine release in the striatum in resting conditions in humans.2,3 Empirically, however, STN-DBS is suitable to PD patients who have motor impairments that are characterized by fluctuating periods of immobility (off) and good motor function (on) and that are responsive to dopaminergic agents. 4 In addition, it can reduce the required dosages of dopaminergic medication. While a major role of STN-DBS is thought to be a suppression of the overactivation of STN neurons and a facilitation of excitatory signals to the cerebral cortex, 5 findings in dopaminergic studies have suggested that STN-DBS exerts a facilitatory effect on the dopamine system by boosting motor recovery after treatment.
Dopaminergic pathways consist of motor, cognitive, and limbic loops. In the nonmotor (cognitive and limbic) loops, the caudate, which belongs to the cognitive loop, is involved in motor learning and memory 6 and feedback processing, 7 and the ventral tegmental area (VTA) and nucleus accumbens (NA) are implicated in the limbic loop. Although there is no known direct anatomic connections between the VTA or NA and STN, dopaminergic axons originating from the substantia nigra compacta (SNc) and VTA run adjacent to the STN on their way to the caudate and NA. It was recently reported that the STN might be mechanistically important in motor processes linking motivation to improvement in motor performance. 8 Our previous positron emission tomography (PET) study showed that strenuous motor exercise enhanced dopamine release in mesolimbic dopaminergic regions in patients with PD, suggesting a contribution of the dopaminergic motivational system in motor execution in PD. 9 Hence, STN-DBS may have significant effects on these nonmotor dopaminergic loops.
The present study was designed to elucidate the mechanisms of dynamic STN-DBS effects on motor recovery by examining dopamine release in the basal ganglia, especially in the nonmotor loop regions, with PET and [ 11 C]raclopride in PD patients in DBS-off and DBS-on conditions while they were engaging in motor exercise.
MATERIALS AND METHODS
Patient Selection
Twelve PD patients (mean age ± s.d.: 64.9 ± 7.8, 6 men and 6 women) with bilateral STN-DBS devices that had been implanted for >1 month participated in this study. The mean duration of disease was 12.3 years, and several different anti-parkinsonian drugs were prescribed. In the stereotactic surgery, a quadripolar DBS lead (No. 3389; Japan Medtronic, Inc., Tokyo, Japan) was implanted after physiologic refinement of the target. Implantable Pulse Generators (Soletra; Japan Medtronic, Inc.) were placed bilaterally in the frontal chest under general anesthesia on the same day. No patient showed mood changes or psychiatric disorders after STN-DBS. Written informed consents for the present study were obtained before PET scanning, which was approved by the local ethics committee of Hamamatsu Medical Center. The demographic and neurobehavioral features are described in detail in Table 1.
Characteristics of patients with Parkinson's disease
DD, disease duration; H&Y, Hoehn and Yahr disability score; UPDRS, unified Parkinson's disease rating scale after the PET study; ZSDS, the Zung Self-Rating Depression Scale after the PET study; MMSE, Mini-Mental State Examination; DBS, deep brain stimulation.
Task Performance and Clinical Evaluation
As described in a previous study, 10 patients were instructed to perform right-foot sequential extension/flexion movements at their own pace (close to 0.5 Hz). All patients studied were right-footed and experienced bilateral parkinsonism rated as Hoehn and Yahr stage 3 or above, indicating that the laterality of the motion side was of little significance in the present study. The task was started at the time of [ 11 C]raclopride injection and continued throughout the scan. During the performance, time-course physiologic changes of pulse rate were monitored. To quantify the changes in the motor task, the motion speed and mobility angle of the foot at the ankle were measured twice (30 and 60 minutes after task start) during each PET scan. We made video recording, and measured the motion speed and mobility angle of the foot after the scanning. In our preliminary study, no significant correlations were found between single factors (motion speed or motion angle of the foot) and raclopride binding potentials. To quantify the load of task, therefore, the score of the foot motion product was calculated using the following formula: motion speed (Hz) × angle of the foot at the ankle. To evaluate the changes in motor functions and mental states by STN-DBS, the Unified Parkinson's Disease Rating Scale (UPDRS) and the Zung Self-Rating Depression Scale (ZSDS) were measured in DBS-on and DBS-off conditions.
Imaging Procedures
All participants underwent three-dimensional magnetic resonance imaging (0.3 T MRP7000AD; Hitachi Medical Corporation, Tokyo, Japan) just before the PET measurements. The PET scans were conducted with a high-resolution brain-purpose camera (SHR12000, Hamamatsu Photonics K.K., Hamamatsu, Japan) with a serial scan protocol (time frames: 4 × 30 seconds, 20 × 60 seconds, 14 × 300 seconds) after a slow bolus injection of 300 MBq [ 11 C]raclopride without arterial sampling. In-plane spatial resolution is 2.7 mm at full width at half maximum. The standard spatial normalization using a T1-weighted magnetic resonance was used to normalize binding potential (BPND) maps to Montreal Neuroimaging Institute (MNI) space. The details of the procedure were described elsewhere. 11 All medications were suspended for at least 12 hours before the PET measurements. All patients underwent two scans consecutively with an interval of 3 hours in the stimulation-off and stimulation-on conditions. The order of the two PET scans (off and on) was counterbalanced among patients to minimize any order effects of stimulation. During DBS-off scans, the stimulator was turned off 1 hour before the scan. During DBS-on scans, it was switched on 1 hour before the scan. As described above, all participants performed sequential foot movements during both scans. The details of the PET procedures with foot movement were described elsewhere. 10
Image Data Analyses
Magnetic resonance imaging regions of interest (ROIs) were set bilaterally over the caudate, NA, ventral putamen, and dorsal putamen11,12 and transferred onto the corresponding [
11
C]raclopride PET images with imageprocessing software (Dr View; Asahi Kasei Corporation, Tokyo, Japan) on a workstation (Hyperspara ss-20; Oracle Corporation, Redwood Shores, CA, USA).
11
As described previously,10,13 the cerebellum was selected as the reference region for [
11
C]raclopride. Using time-activity curves of target and reference regions, the BPND in each region was estimated with a noninvasive Logan plot analysis.
14
Because the PET distribution image that was used for ROI setting was composed of two consecutive images that covered 6.8-mm-thick slices in the
Statistical Analyses
Foot motion products that were measured during the two stimulation conditions (30 and 60 minutes after the task start) were compared using Wilcoxon signed-ranks tests. In the ROI analysis, paired
In the SPM analysis, paired
RESULTS
Changes in Physiology and Behavior
There were no significant changes in physiologic parameters (mean blood pressure) at the end of the scans between the two PET measurements (DBS-on: 92.3 ± 8.5; DBS-off: 89.0 ± 9.2). The magnitudes of foot motion products 30 and 60 minutes after the task start were higher during the DBS-on condition than during the DBS-off condition (
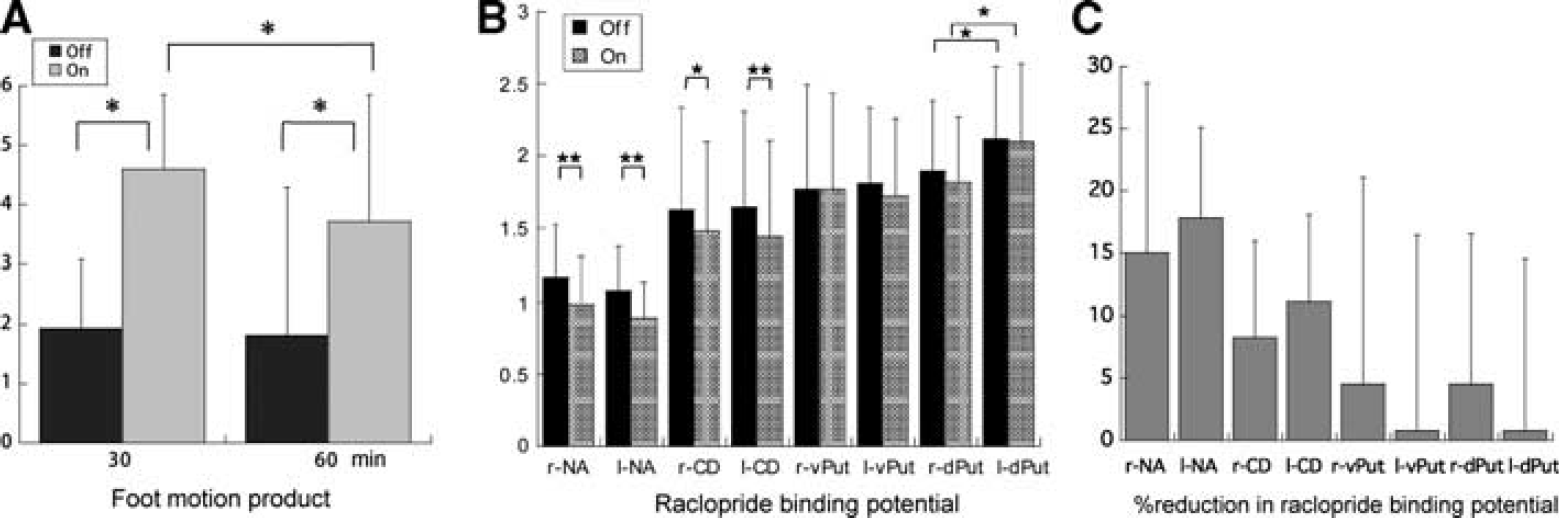
Changes in motor performance and [
11
C]raclopride binding. (
Changes in [ 11 C]raclopride Binding
Paired
Levels of binding potentials for [11C]raclopride in subthalamic nucleus deep brain stimulation-off and -on stimulation conditions
Values are expressed as mean±s.d. %reduction: the mean value of reduction (percentage) in [11C]raclopride binding during On stimulation compared with Off stimulation.
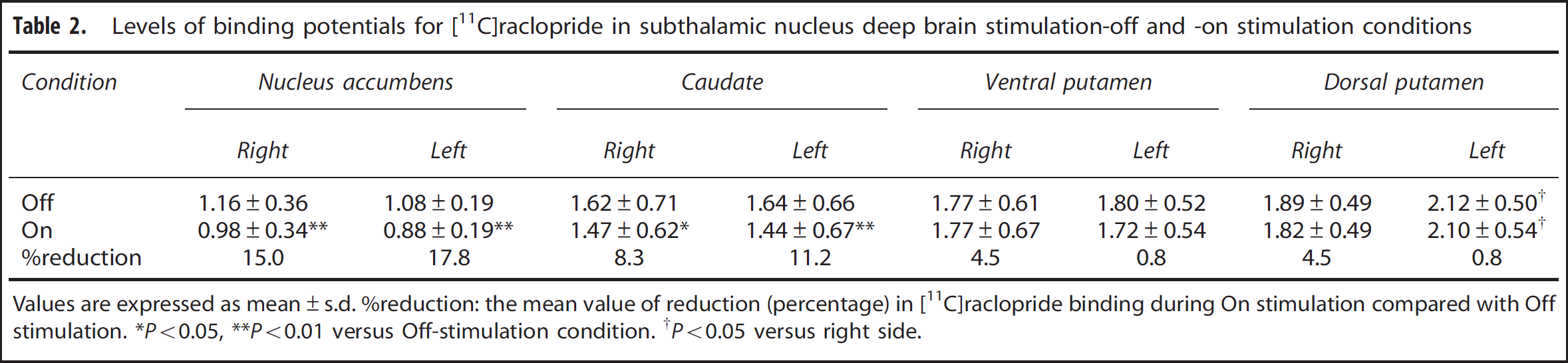
Brain regions superimposed on magnetic resonances images showing significant reductions in [
11
C]raclopride binding in the on-stimulation condition compared with the off-stimulation condition (nucleus accumbens: (left:
In the patients with bilateral parkinsonism that was rated as Yahr 2 and above, there were hemispheric differences in left dorsal putamen binding irrespective of stimulation condition. This indicated that regional differences in pathophysiology were present in the patients with bilateral parkinsonism (Table 2; Figure 1B).
Correlation Between Motion Product and [ 11 C]raclopride Binding
A Pearson's correlation coefficient test showed that the degree of %increase in foot motion product was inversely correlated with the %reduction in [
11
C]raclopride binding in the bilateral NA during the DBS-on condition (right:
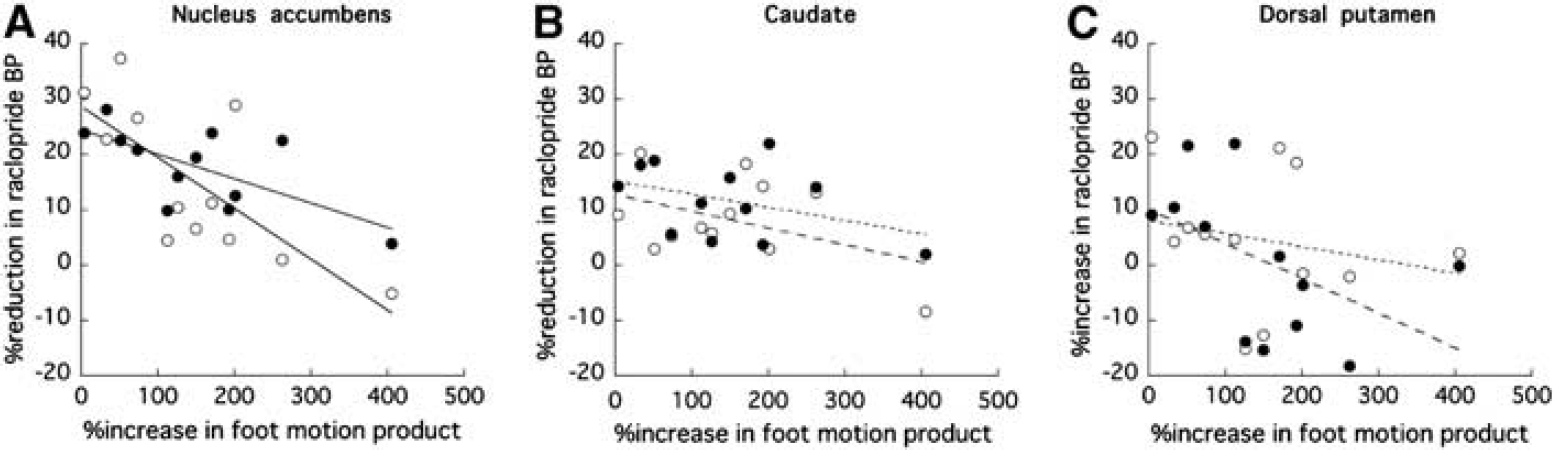
Correlation between changes in [
11
C]raclopride binding (BP) and motor recovery. Pearson's correlation coefficient test showed a significant correlation between the magnitude of %reduction in [
11
C]raclopride binding and the %increase in foot motion product in the bilateral nucleus accumbens (
Correlation Between Clinical Parameters and [ 11 C]raclopride Binding
Comparisons of changes in clinical parameters (UPDRS and ZSDS) with DBS plus exercise-induced changes in [
11
C]raclopride binding showed that the magnitude of the percentage of reduction in the motor scores of the UPDRS (improvement of parkinsonism) was significantly and inversely correlated with the %reduction in the binding in the left caudate (left caudate:
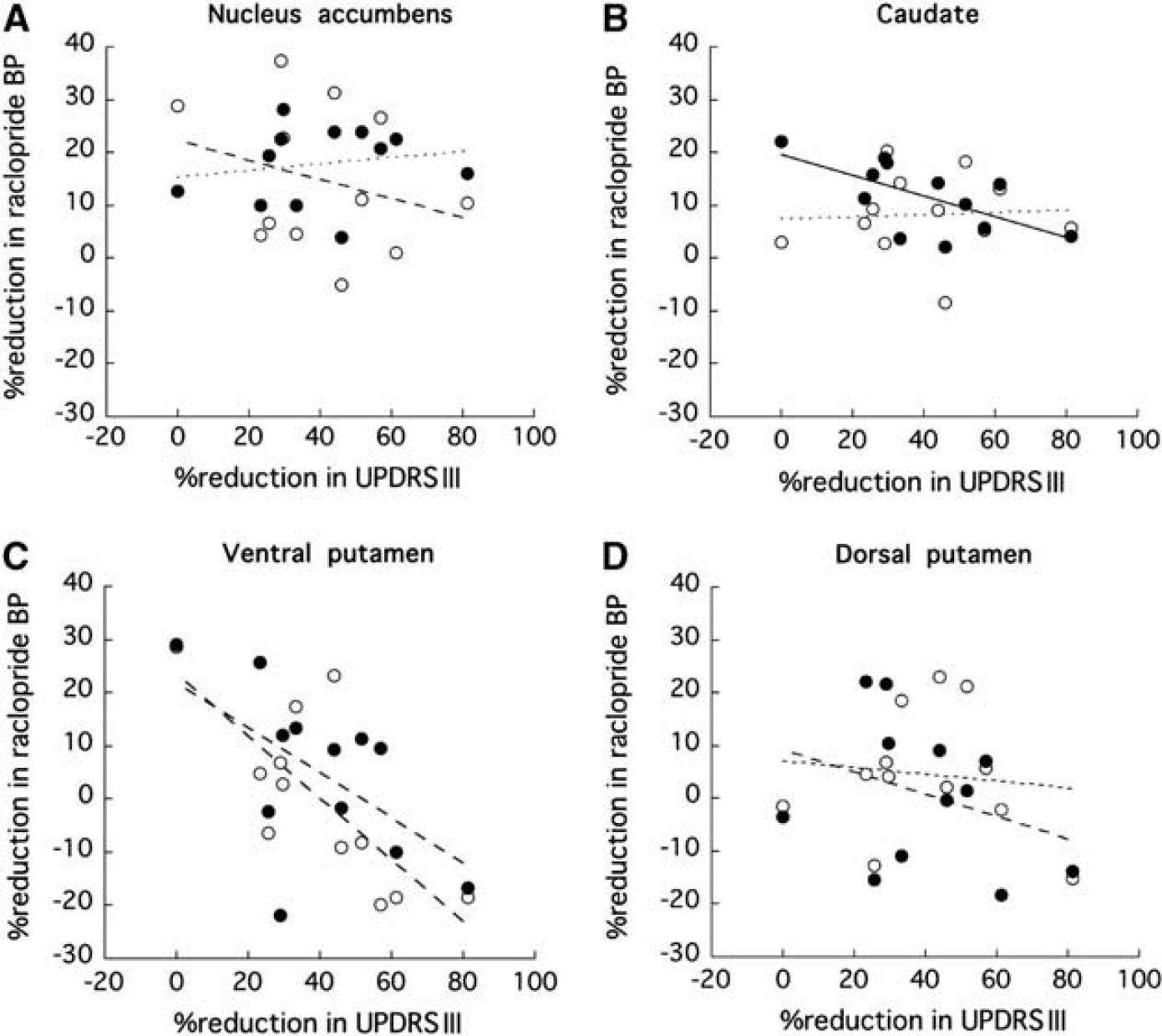
Correlation between changes in [
11
C]raclopride binding (BP) and parkinsonian symptoms. The magnitude of the %reduction in [
11
C]raclopride binding was significantly and inversely correlated with the Unified Parkinson's Disease Rating Scale (UPDRS) score in the left caudate (
DISCUSSION
The present study is the first to show dopamine release in the mesolimbocortical projection region during exercise in response to STN-DBS in patients with PD. This indicates that the motor recovery of parkinsonism by STN-DBS may coincide with dopaminergic activation in the nonmotor dopamine system. The theory of nonmotor motivational activation-based motor recovery by STN-DBS may be accepted considering in the clinical setting that lesser amount of dopaminergic drugs is need after STN-DBS. Because no dopamine release was seen with STN-DBS at rest,2,3 STN-DBS itself may not be sufficient to activate dopamine neurons directly or indirectly without concomitant voluntary movement. The present results may partly explain the mechanisms of STN-DBS in the amelioration of motor parkinsonian symptoms.
Anatomical View Point
Dopaminergic pathways are functionally divided into three major projections: nigrostriatal, mesocortical, and mesolimbic. 16 Specifically, the mesolimbic and mesocortical dopamine systems are engaged in the reward system. 17 Because there was no change in [ 11 C]raclopride binding in the putamen but there was change in the NA and caudate in the present study, STN-DBS may be preferably associated with activation of the reward system.
The STN is important in the motor cortico-basal gangliathalamocortical circuit.
18
In primates, STN neurons in the dorsolateral two-thirds of the region connect to the putamen and the globus pallidus (GP) externa, while the neurons in the ventromedial third of the nucleus project to the caudate nucleus and GP interna/substantia nigra pars reticulata (SNr). The medial tip of the STN mainly sends axons to the GP ventralis.
19
The presence of this anatomic segregation in the STN indicates that the activation of the projections depends on the location of the stimulator in the STN. Anterograde tract-tracing studies with
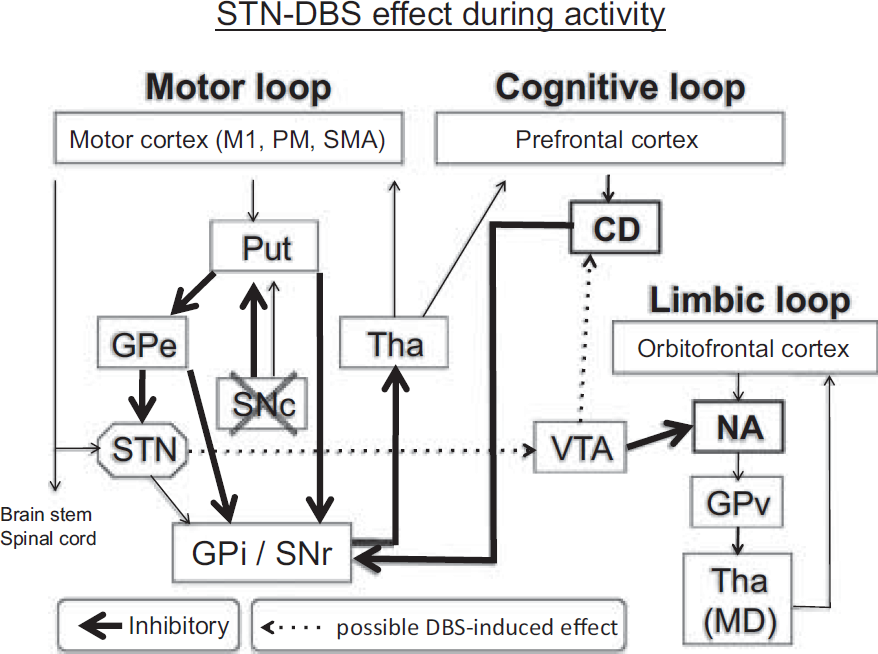
With STN deep brain stimulation (DBS) during activity, dopaminergic activation that occurs in the CD results in stimulation of the PMC, SMA, and prefrontal cortex, and dopaminergic activation in the nucleus accumbens (NA) stimulates the orbitofrontal cortex. Activation in these nonmotor loop systems through DBS may exert positive effects on the motor system and ameliorate parkinsonian symptoms. Put, putamen; CD, caudate; NA, nucleus accumbens; GPe, globus pallidus externa; GPi, globus pallidus interna; Tha, Thalamus; STN, subthalamic nucleus; SNc, substantia nigra pars compacta; SNr, substantia nigra pars reticulata; VTA, ventral tegmental area; MD, mediodorsal thalamic nucleus; GPv, ventral globus pallidus; M1, motor cortex; PMC, premotor cortex; SMA, supplementary motor area.
Role of the Mesolimbocortical Dopaminergic Pathway
In the present study, increased dopamine release was found in the caudate and NA during motor performance with STN-DBS. The caudate provides evaluative signals and reward-driven biases to influence associative learning and reward-modulated behaviors, 22 and the NA is involved in the regulation of adaptive, goal-directed activity,23,24 and appetite. 25 In monkeys, the NA shell is more sensitive to novel circumstances and more involved in visceral and motivational mechanisms26,27 than the NA core, which is involved specifically in motor control and the learning of appetitive behavioral responses.28,29 Considering these functional roles in the caudate and NA, neuronal activation of these nuclei likely affects motor performance.
At early stages of PD (Hoehn and Yahr I–II), degeneration occurs in nigral neurons innervating the dorsal putamen, 30 and mild changes in dopaminergic presynaptic terminals are found in the caudate and NA. 31 Even with the disease progression that occurs before Hoehn and Yahr stage III–IV, the caudate and NA remain relatively lightly affected. 32 This heterogeneous progression of PD may benefit from the therapeutic intervention of STN-DBS. Indeed, dopaminergic treatment increased striato-frontal connectivity between the caudate and the prefrontal cortex during motor timing in PD. 33 Activation (dopamine release) in the ventral striatum and mesocortical projection region (orbitofrontal cortex) was observed during long-distance walking exercises in patients with PD of Hoehn and Yahr stage II–III, which was in contrast to the finding that the putamen (motor striatum) was activated in healthy normal subjects. 9 The orbitofrontal cortex is involved in sensory and affective integration, decision-making, and expectation, 34 and it subserves the planning of behavior according to the level of awareness to reward and punishment. 35 Thus, in PD patients, there might be greater changes in dopaminergic activation in the mesocortical region (caudate and NA) than in the nigrostriatal region (putamen) for the execution of purposeful behavior, such as the completion of stressful gait.
Implication of the STN-DBS Effects in Parkinson's Disease
Previous reports that showed no significant striatal dopamine release by STN-DBS at rest2,3 indicate that STN-DBS does not act on dopaminergic activation in the striatum without voluntary movement. It is thought that the main effect of STN-DBS is to suppress the neuronal hyperactivation of the STN that results in increased inhibitory signal inputs to the thalamus through the GABAergic system in patients with PD. Thus, primarily, there might be no specific relevance of STN-DBS to dopaminergic enhancement. As mentioned above, however, a reduction in the dosages of dopaminergic treatments and the amelioration of the frequency of motor fluctuations or involuntary movement after STN-DBS therapy suggest considerable effects of dopaminergic neuronal stimulation in patients with PD. The present findings showed effects on the caudate and NA during motor voluntary movement with STN-DBS. As described above, histologic evidence that STN neurons project to the caudate and VTA, which then send axons to the NA, suggests that STN stimulation affect these regions only to stimulate dopamine release during motor performance. Because the basic idea is that DBS inhibits overexcited neurons, these connections might be inhibitory, which is similar to the STN-GP projection. A recent study showed that different locations of the stimulator electrode in and around the STN generated different amounts of dopamine release in the dorsomedial caudate in awake monkeys. 36 In this study, the maximal increase in dopamine release was shown when the electrode was placed in the zona incerta, which is located dorsal to the STN. Tyrosine hydroxylase immunohistochemistry stains catecholaminergic axons, which originate from the substantia nigra (SNc and SNr) and VTA and run dorsally through the STN to the caudate. 36 Therefore, in practical settings, electrodes focused on the STN can yield different degrees of influence on the NA and caudate dopaminergic regions, where degeneration is much slower than in the putamen. 31
STN-DBS induced Dopamine Changes and Clinical Scores
In the present study, the magnitude of %reduction in [ 11 C]raclopride binding in the bilateral NA correlated inversely with the %increase in foot motion product during the DBS-on condition (Figure 4A). In addition, a similar tendency was found in the bilateral caudate and bilateral dorsal putamen. This suggested that PD patients with a greater capacity for motor exercise would need less dopaminergic activation (dopamine release) in the mesolimbocortical projection area, possibly because of effective STN stimulation. In contrast, patients with greater difficulties in motor execution may require more dopamine release in the area during performance, possibly because of less responsiveness of the stimulation. Indeed, this contention might be supported by our additional finding that there was an inverse correlation between DBS on-off changes (greater differences in scores) in the evaluation of parkinsonism UPDRS-part 3 (motor function) and the %reduction in [ 11 C]raclopride binding in the caudate (Figure 4B). If DBS is able to improve motor performance, then a greater production of endogenous dopamine in the mesocortical region may not be necessary anymore. The present findings may reflect the pathophysiology of the dopamine system with regard to the facilitatory effects of STN-DBS. Because it has been reported that unilateral DBS improves bilateral symptoms 37 and that unilateral foot sequential movement itself increases dopamine release in the ipsilateral striatum, 10 bilateral STN-DBS during unilateral foot exercise should have significant effects on both sides. A larger sample size may be necessary to test this, but a series of studies including ours suggest that, regardless of the side of voluntary movement or stimulation, bilateral STN-DBS would be beneficial in stimulation of the entire striatal dopamine system.
Conclusion
The effects of STN-DBS during motion on motor recovery may be because of compensatory activation of the motor loop through the stimulation of the mesolimbocortical dopaminergic system in patients with PD. Effective stimulation by STN-DBS may feature less dopamine release in the region in conjunction with sufficient amounts of exercise.
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest.
Footnotes
ACKNOWLEDGEMENTS
The authors would like to thank Messrs. Kenichi Sato and Akihito Oda (Hamamatsu Photonics KK) for their support.