The high-affinity radioligand [18F]fallypride (FP) is frequently used for quantification of striatal/extrastriatal D2/3 receptors and the receptor occupancies of antipsychotics (APs). Its 110 minutes half-life allows long scan durations. However, the optimum scan duration is a matter of debate. This investigation focuses on scan-duration-related effects on simplified reference tissue model (SRTM) results and the time point of transient equilibrium in a large sample of dynamic FP positron emission tomography (PET) scans. Fifty drug-free and 50 AP-treated subjects underwent FP-PET scans (180 minutes scan duration). The binding potential (BPND) of the putamen, thalamus, and temporal cortex were calculated using the SRTM and the transient equilibrium model. Furthermore, receptor occupancies were calculated for AP-treated patients. Transient equilibrium in the unblocked putamen occurred after 121 ± 29.6 minutes. The transient equilibrium occurred much earlier in the extrastriatal regions or under AP treatment. Stepwise scan shortening caused BPND under-estimations of 0.58% for the first 10-minute reduction (putamen, SRTM), finally reaching 5.76% after 1 hour scan-time reduction. We observed preferential extrastriatal AP binding irrespective of the analytical method. [18F]fallypride scan durations of 180 minutes reliably reach equilibrium even in D2/3-receptor-rich regions. Moderate reductions in FP scan durations only caused small changes to SRTM results even in receptor-rich regions. Apparently, the D2/3 receptor occupancy results of APs, especially preferential extrastriatal binding observations, are not relevantly biased by inappropriate scan durations.
The high-affinity ligand [18F]fallypride (FP) is one of the most frequently used ligands for D2/3 receptor imaging (Mukherjee et al, 1995; Vernaleken et al, 2008a). Because of its high affinity and long half-life, this ligand has proven valuable for the quantification of striatal and extrastriatal D2/3 receptors during one single positron emission tomography (PET) scan. However, for the use in clinical studies, some more properties should be considered. Shorter, more practical scan durations and the applicability of non-invasive reference region methods can increase the patients' acceptance of such scientific investigations and prevent relevant bias in patient inclusion. The simplified reference tissue model (SRTM; Lammertsma and Hume, 1996) is frequently used in FP-PET investigations. It primarily depends on the existence of a suitable reference region devoid of D2/3 receptors. Although there have been some evidence of very low cerebellar D2/3 receptor concentrations, this structure appears to be the most appropriate reference region. Kinetic constraints for the application of the SRTM as expressed by Buchert and Thiele (2008) can be considered to be fulfilled on the basis of the kinetic parameters reported by Siessmeier et al (2005). An early comparison between the two-tissue compartment model (2TCM) and two reference region methods (SRTM, and the transient equilibrium method; TEM) (Farde et al, 1989; Ito et al, 1998) showed high and statistical significant intermethod correlations (Siessmeier et al, 2005).
As depicted earlier, it is of major interest to find the best compromise between practicality and model-related constraints. A systematic evaluation of scan-time effects on the outcome parameters of FP-PET scans has never been performed. Therefore, we conducted a post hoc analysis including 100 subjects, of which 50 were under antipsychotic (AP) medication and 50 were free of any neuropsychiatric medication. In respect to medication-free subjects, our study had three goals. (1) We searched for the existence and consequently for the corresponding time point of estimated transient equilibrium conditions. (2) The impact of different scan durations on the SRTM results was depicted by artificial and stepwise removal of later time frame data.
The subgroup analysis of 50 AP-treated patients focuses on the impact of scan durations on D2/3 receptor occupancy results. In several studies, FP-PET was used to compare striatal and extrastriatal D2/3 receptor occupancies caused by second-generation antipsychotics (Vernaleken et al, 2008a). However, it has been hypothesized that inaccurate estimation of binding potentials (BPND) in regions with high D2/3 receptor densities (caused by insufficient scan durations) can potentially influence some of the conclusions (e.g., preferential extrastriatal binding) drawn from these results (Olsson and Farde, 2001). Therefore, we also assessed the impact of scan duration on the misinterpretation of AP-induced D2/3 receptor occupancies.
Materials and methods
This investigation is a post hoc analysis of several PET studies using FP as the radioligand. Some patient and control subject data are part of previously published reports about the extent of D2/3 receptor occupancies under AP treatment with clozapine, ziprasidone, and quetiapine (Gründer et al, 2006; Vernaleken et al, 2008b, 2010). All clinical studies were approved by the ethics committee of the medical faculty of the RWTH Aachen University (Aachen, Germany), the ethics committee of the medical chamber of Rheinland-Pfalz (Mainz, Germany), and the German radiation safety authority.
Subjects
Subjects included healthy volunteers (n = 27) and patients with various neuropsychiatric disorders (n = 73). All subjects participating in the study gave written informed consent. They all underwent physical and mental state examinations. Patients suffering from neurologic or relevant somatic diseases were not included, nor were patients reporting illegal drug consumption in the last 6 months, except two patients with Tourette's syndrome who ingested THC-containing products up to 6 weeks before the PET scan. Drug screening was performed at the beginning of the inpatient stay and 1 day before the scan. All PET studies were performed at the PET centers of the University of Mainz and RWTH Aachen University, Germany.
A total of 100 subjects were included (age: 18 to 64 years, mean ± s.d.: 33.4 ± 10.4; 78 ♂ + 22 ♀). At the time of the PET scan, 50 subjects were free of any centrally acting substances and drugs directly acting on dopaminergic systems for at least 6 months (age: 18 to 58 years, mean ± s.d.: 31.0 ± 10.5; 40 ♂ + 10 ♀). This unblocked group consisted of 21 patients suffering from schizophrenia (according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV); 10 subjects were drug naive), two patients suffering from Tourette's syndrome (scanned under propofol anesthesia) (Vernaleken et al, 2009), and 27 healthy subjects. The remaining 50 subjects (age: 18 to 64 years, mean ± s.d.: 35.7 ± 9.9; 38 ♂ + 12 ♀) were patients undergoing stable AP treatment (100 to 500 mg clozapine, 80 to 200 mg ziprasidone, 200 to 1,300 mg quetiapine, or 5 to 20 mg olanzapine). In this group, the following variable diagnoses were made: schizophrenia (n = 38), schizoaffective disorder (n = 9), transient psychosis (n = 2), cyclothymic disorder (n = 1), and personality disorder (n = 1).
Radiochemistry
[18F]Fallypride was synthesized using a high-yield modification of the method for [18F]DMFP synthesis (Hamacher et al, 1986; Gründer et al, 2003) by using the tosylated precursor ((S)-N-[(1-allyl)-2-pyrrolidinyl)methyl]-5-(3-toluenesulfonyloxy-propyl)-2-ethoxybenzamide. Quality control before injection included determination of chemical and radiochemical purity, specific activity, pH, and absence of pyrogens.
Positron Emission Tomography Data Acquisition
Images were acquired on a Siemens ECAT EXACT whole-body PET scanner in 3D mode (field-of-view, 16.2 cm; 47 planes; full width at half maximum axial, 6.0 mm; in-plane, 6.0 mm). Data acquisition consisted of a series of 39 time frames (3 × 20 seconds, 3 × 1, 3 × 2, 3 × 3, 21 × 5, 2 × 8, and 4 × 10 minutes), resulting in a total scanning time of 180 minutes. A 15-minute transmission scan using a 68Ge source was performed before each study for subsequent attenuation correction. Head movement was minimized by means of a vacuum mask. A mean of 218 ± 33.9 MBq (mean ± s.d.; range: 101 to 264 MBq) FP was injected intravenously as a bolus into a cubital vein over ∼30 seconds (unmedicated subjects: 215 ± 28.6 MBq, range: 149 to 251 MBq; treated patients: 221 ± 38.7, range: 101 to 264 MBq). There was no statistical significant difference between the two groups (Δ: 6 MBq; P = 0.45; unpaired two-sided t-test). The average specific activity at the time point of injection was 316 ± 825 GBq//mol. There was o correlation between binding potentials and specific activities (medication-free subjects), irrespective of the volume of interest (VOI) analyzed (putamen, r = 0.137; thalamus, r = 0.231; inferior temporal cortex (GTi), r = 0.146; Pearson's correlation).
Image Processing
Images were reconstructed with filtered back-projection using a Hanning filter (filter width: 4 mm). Although in most scans only moderate head movement was observed, a motion correction was performed (Flexible Image Matching and Fusion Tool (PFUS) implemented in PMOD V3.1, Zürich, Switzerland) using a sequential registration procedure beginning with frame 10 while assuming no relevant dislocation during the first 10 minutes. To check the quantity of misregistration, we checked the position of striatal VOI as well as the appropriate match of the brain surface contours by visual inspection. Rare misregistrations were corrected by manual registration. Thirteen scans had to be interrupted for two 5-minute frames mainly because of the patient's desire to urinate. Repositioning was performed using three marks, indicating the previous head position; this was followed by registration of the postinterruption frames to the previous frames. For spatial normalization, the early frames (usually frames 3 to 8) of the dynamics were averaged and registered to an Montreal Neurological Institute (MNI) template using the warp transformation process of the Automated Image Registration package (Woods et al, 1992) (implemented in MEDx software v3.43; Medical Numerics, Germantown, MD, USA); the corresponding registration parameters were then applied to the entire dynamic scan. To extract the time-activity curves (TACs), templates of polygonal VOIs were applied to the spatially normalized dynamic recordings. This VOI template was chosen in several previous FP-PET studies (Vernaleken et al, 2008b, 2009, 2010); it focuses on regions showing a sufficient extent of D2/3 receptor availability for FP binding and stable statistics. Time-activity curves were calculated for the following VOIs: the cerebellum, putamen, GTi, and thalamus. Volumes of interest for the caudate nucleus, amygdalae, and other cortical and midbrain regions were also calculated in the original studies. However, these VOIs were omitted in the present post hoc analysis because the present choice of VOIs focuses on the representation of brain regions with high, moderate, and low D2/3 receptor densities.
Data Analysis
The general quantification procedures followed the SRTM as described by Lammertsma and Hume (1996). For the calculation of BPND values by the SRTM, we used the unfitted TACs. The TEM (Farde et al, 1989) was applied under the following assumptions: the tissue radioligand activity in the nondisplaceable compartment is the same in the reference and receptor-containing tissues and the tissue radioligand activity bound to the receptors CS(t) equals the difference of CT(t)–C'T(t) (CT is the tissue radioligand activity in the receptor-containing region of interest and C'T is the tissue radioligand activity of [18F]FP in the reference tissue (cerebellum)). When CS(t) is plotted and a curve is fitted to these data, dCS(t)/dt = 0 at the peak of this curve (the point of ‘peak equilibrium’); thus, CS(t)/C'T(t) = BPND = k3/k4. The TEM provides the time point of the transient equilibrium, which is one of the main variables for this post hoc analysis.
For the TEM, the TACs of the cerebellum (as a reference region), putamen, thalamus, and GTi were fitted to predefined functions. The putamen TACs were fitted to a standard Höhrl function (f(x) = A × (BX) × XC. The TACs of the thalamus, GTi, and cerebellum were fitted to another exponential function: (f(x) = A × EXP (B/X + C × X) + D × ln(X)). These equations provide suitable approximations of the TACs for blocked and unblocked conditions. In only a few cases, the fits of very early time points (< 4 minutes) yielded implausible results. However, this did not disrupt the assessment of equilibrium. Parameter approximation for TAC fitting was performed by LabFit software V7.2.42 (Silva and Silva, 1999–2008). The fitted cerebellum curve was subtracted from the corresponding individual target-VOI curves. Afterwards, the local maximum of this curve in the limits of 0 < x < 180 was determined. For TACs that showed no maximum during the 3-hour PET scan, the CS(t)/C'T(t) ratio was determined at t = 180 minutes (n = 3).
To visualize characteristic TAC activity, data were transformed to standard uptake values (SUV = CT [Bq/g] × BW [kg]/A [MBq] to account for body weight (BW) and injected activity (A).
Statistics
The BPND values obtained from different analytical methods were compared using the paired two-sided t-test. In all analyses, the two-tailed level of statistical significance was set at P = 0.05. Pearson's correlations and linear regression analysis were performed using SPSS software (v14.0; SPSS Inc., Chicago, IL, USA), to characterize the possible impact of the analytical method on BPND values.
Simulations of reduced scan durations (60 minutes reduction in 10 minutes intervals) were performed on all putamen and thalamus TACs of unblocked subjects. These SRTM results were compared with the individual 180-minute data.
To detect possible influences on receptor occupancy values, the extent of D2/3 receptor binding under AP treatment was calculated according to the following equation:
The 50 medication-free subjects (age matched) served as a control group; we did not perform intraindividual pre/post analyses.
Results
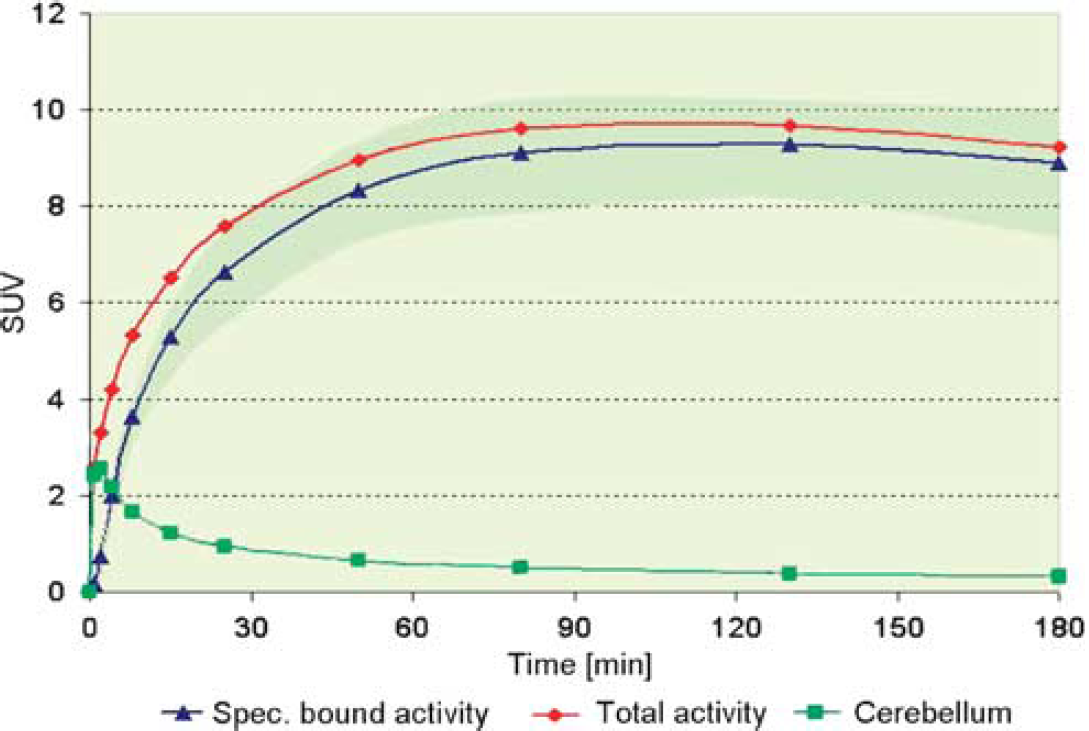
The estimated time of equilibrium from averaged SUV curves was 120.6 ± 29.6 (76.1 to > 180) minutes (mean ± s.d. (range)) in the putamen (Figure 1) as well as 29.2 ± 8.8 (14.6 to 54.7) and 29.4 ± 14.9 (7.7 to 46.1) minutes (mean ± s.d. (range)) in the thalamus and GTi, respectively. The corresponding time points under AP treatment were in the putamen 77.7 ± 31.1 (29.5 to 167.2) minutes, in the thalamus 18.4 ± 9.3 (3.8 to 39.7) minutes, and in the GTi 28.7 ± 15.9 (6.7 to 67.0) minutes (mean ± s.d. (range)). The fits of the specific binding curves for the putamen failed to reach a maximum in only two cases of medication-free subjects; their estimated time points of transient equilibrium (calculated by extrapolation of the fitted TACs) were 190 and 205 minutes after tracer injection in the putamen.
Averaged standard uptake value (SUV) curves of the putamen volume of interest (VOI) (unmedicated subjects: n = 50; red, mean total activity; blue, mean specifically bound activity) and mean cerebellar VOI (green). The average of estimated time points of equilibrium was 121 minutes after injection. The SUV curves (specifically bound) representing the 75% and 25% percentiles of the unmedicated subgroup (borders of highlighted confidence interval; green area) show their maximum before the 180-minute limit.
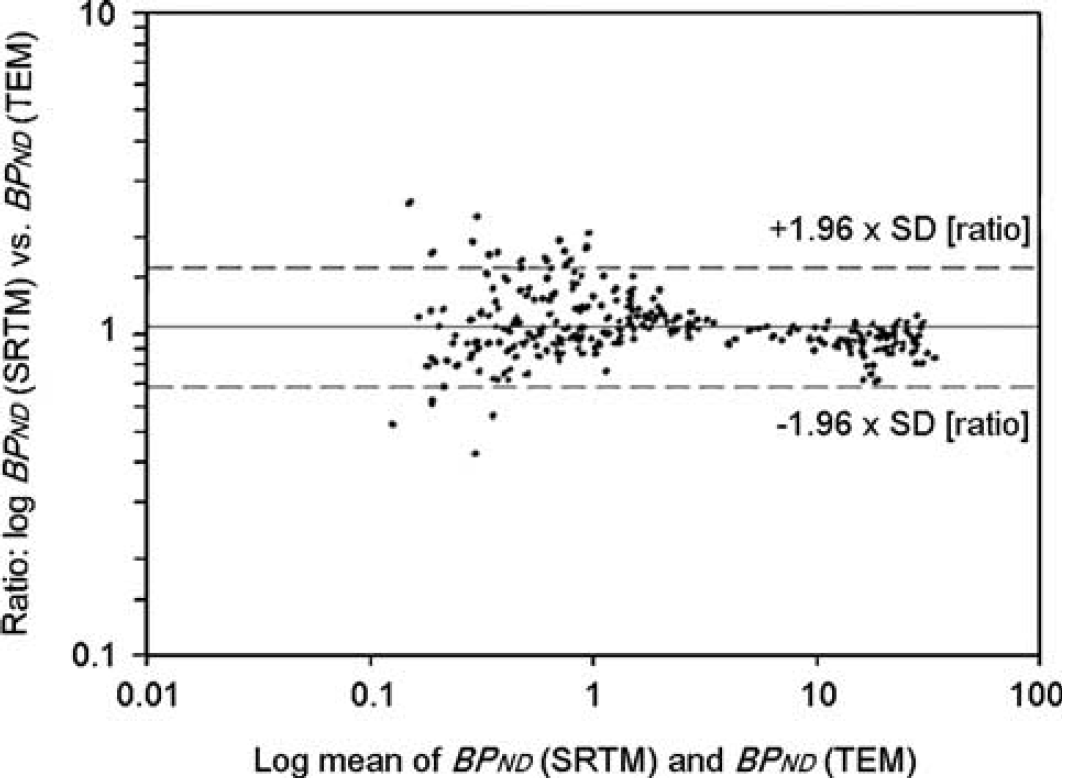
The mean BPND values (SRTM) of medication-free subjects ranged were the following: 22.2 ± 4.9 in the putamen, 2.11 ± 0.57 in the thalamus, and 0.77 ± 0.30 in the GTi (mean ± s.d.). The TEM results were slightly but significantly different in the putamen and thalamus but not in the GTi (for detailed information see Table 1). The BPND values calculated with the TEM and SRTM corresponded considerably (linear regression analysis for putamen: slope = 0.852, r2 = 0.80, P < 0.0001; thalamus: slope = 0.965, r2 = 0.94, P < 0.0001; GTi: slope = 0.841, r2 = 0.87, P < 0.0001). The comparison of SRTM and TEM results have been performed by a Bland-Altman plot; it depicts higher relative intermethod differences at lower binding potentials (Figure 2). We observed a negative correlation between age and BPND values of unmedicated subjects (putamen: r = −0.43, P = 0.0018; thalamus: r = −0.32, P = 0.025; GTi: r = −0.34, P = 0.016; Pearson?s correlation).
A comparison of binding potential (BPND) values according to the simplified reference tissue model (SRTM) and transient equilibrium method (TEM) for 100 subjects (50 second-generation antipsychotic (SGA)-treated patients and 50 drug-free subjects) and for all regions (the putamen, thalamus, and inferior temporal cortex (GTi); observations: n = 300). Data are presented as Bland-Altman plots, showing the individual mean values (TEM and SRTM) on the abscissa as well as the individual ratios of SRTM/TEM on the ordinate. Because of the large range of outcome values (approximately a factor of 102), the plot is scaled logarithmically. The mean ratio of SRTM/TEM is 1.073 (solid line). The plot depicts higher relative differences at lower values of binding potentials.
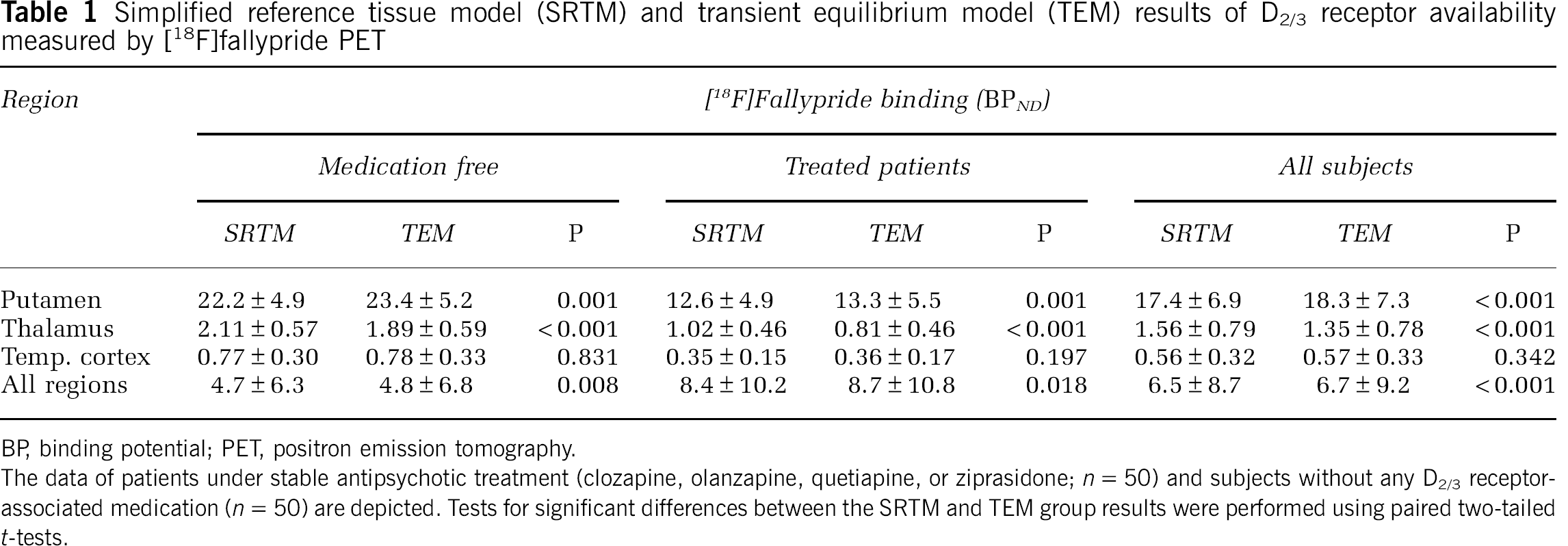
Simplified reference tissue model (SRTM) and transient equilibrium model (TEM) results of D2/3 receptor availability measured by [18F]fallypride PET
The data of patients under stable antipsychotic treatment (clozapine, olanzapine, quetiapine, or ziprasidone; n = 50) and subjects without any D2/3 receptor-associated medication (n = 50) are depicted. Tests for significant differences between the SRTM and TEM group results were performed using paired two-tailed t-tests.
In the subgroup of patients receiving AP medications, we congruently found small but significant differences between the TEM and SRTM in the putamen and thalamus but not in the GTi (for detailed information see Table 1). Both methods were strongly correlated with each other (linear regression analysis putamen: slope = 0.878, r2 = 0.95, P < 0.0001; thalamus: slope = 0.932, r2 = 0.85, P < 0.0001; GTi: slope = 0.780, r2 = 0.75, P < 0.0001).
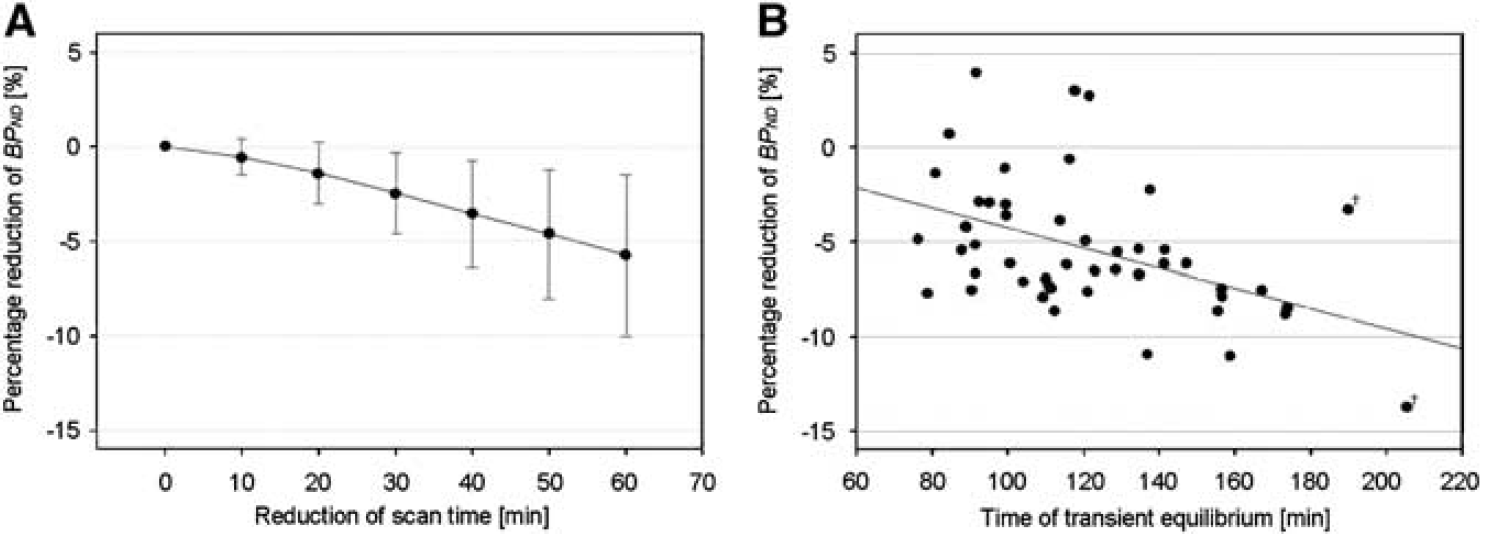
The SRTM simulation of reduced scan durations in the putamen, which was the brain region with the highest D2 receptor density, revealed an average BPND underestimation of −0.13 ± 0.21 (−0.58% ± 0.94%) for the first 10-minute reduction (180 to 170 minutes) (Figure 3A). This effect increased with ongoing time reductions (ΔBPND: −0.25 ± 0.25 (−1.16% ± 1.17%); 130 to 120 minutes). The summed ΔBPND effect of a 1-hour reduction in the scan duration was −1.28 ± 0.96 (−5.8% ± 4.3%). In the extrastriatal regions, we found no effects of reduced scan durations on binding potentials (e.g., 1-hour reduction in the thalamus: −0.01% ± 2.37%). In the putamen, but not in other regions, the change in BPND due to a 60-minute scan-time reduction was significantly correlated with the corresponding individual estimation of equilibrium time point (r = 0.46, P = 0.0008; Pearson?s correlation; Figure 3B).
Results of artificial stepwise reduction of scan durations from 180 (0 minutes reduction) to 120 minutes (60 minutes reduction). Binding potential (BPND) values were calculated for the putamina of 50 subjects without second-generation antipsychotic (SGA) treatment using the simplified reference tissue model (SRTM). (A) The mean percentage reductions of BPND results (circles) and the standard deviations of percent discrepancies (error bars) for every 10-minute reduction in scan time. We found an average BPND underestimation of 0.58% for the first 10-minute reduction. (B) The individual extent of BPND reduction is linearly correlated with the estimated time point of transient equilibrium. In two subjects (†), the equilibrium could not be observed within 180 minutes; in these two cases, the estimated time points of equilibrium (by extrapolation of the fitted time-activity curves) are depicted.
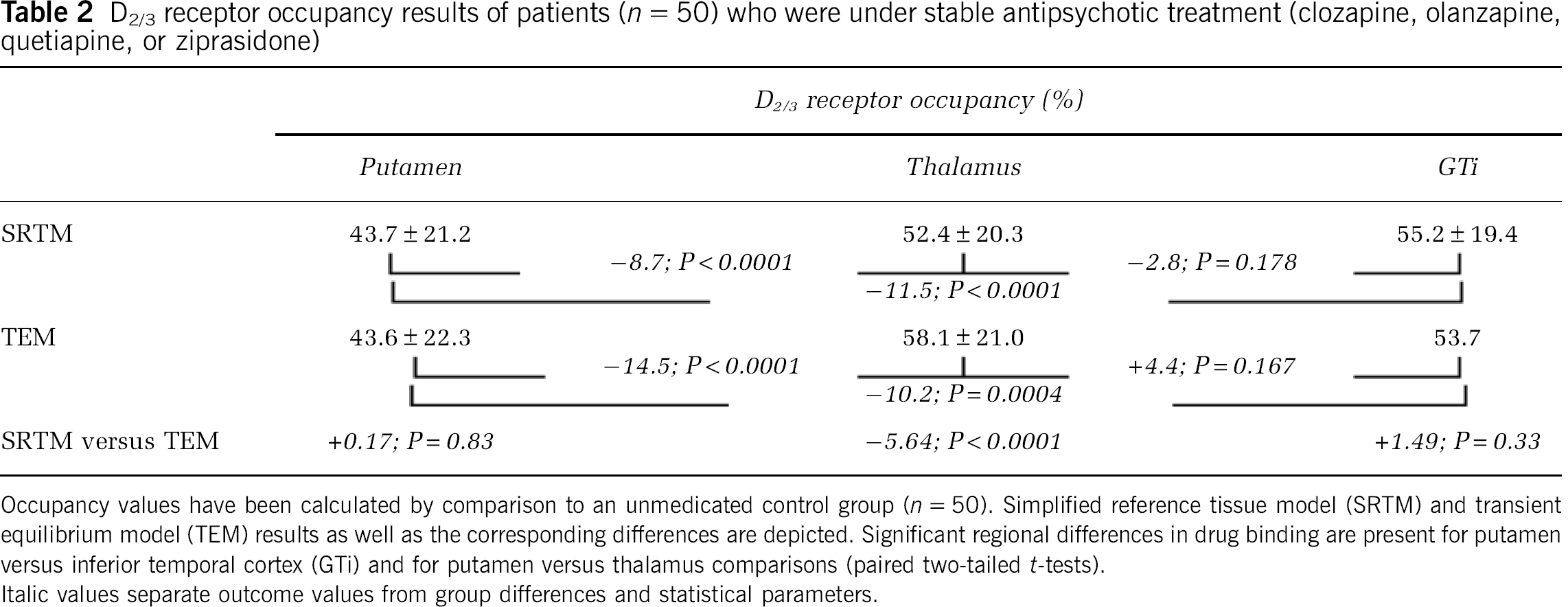
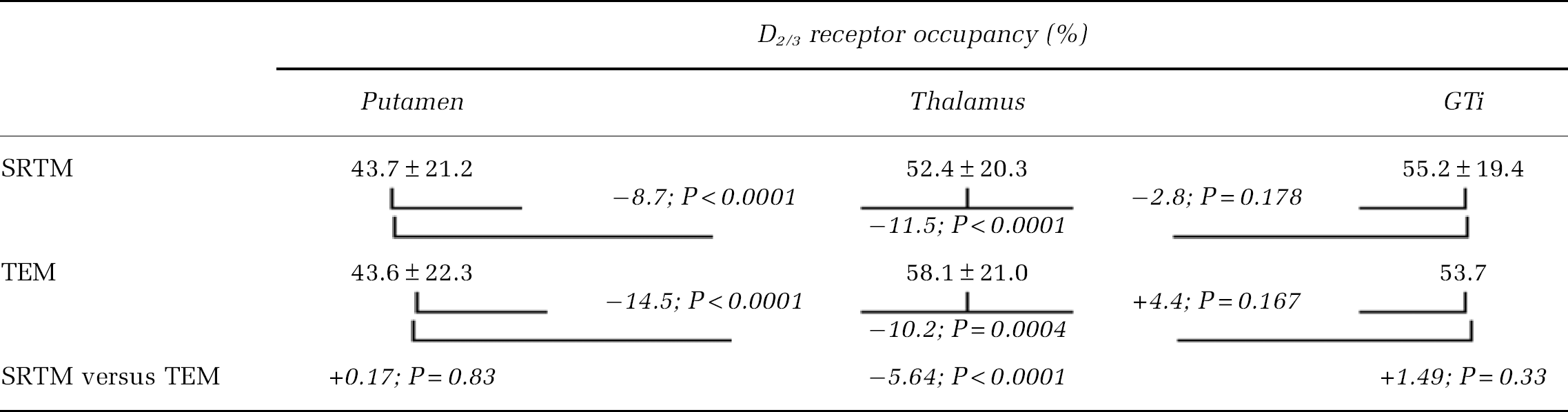
The mean regional D2/3 receptor occupancies caused by AP treatment are depicted in Table 2. In the thalamus, but not in the putamen or GTi, the SRTM and TEM results showed some significant differences. We found significantly lower D2/3 receptor occupancies in the putamen than in the thalamus irrespective of the method used (TEM: −14.5%, P < 0.0001; SRTM: −8.7%, P < 0.0001; two-sided paired t-test). The same was true for the GTi (TEM: −10.2%, P = 0.0004; SRTM: −11.5%, P < 0.0001; two-sided paired t-test). There was no significant difference between the thalamic and cortical occupancies. Based on the simulated data of reduced scan times, a 10-minute reduction of the scan duration would increase these differences (SRTM) to −9.0% (putamen versus thalamus; P < 0.0001; two-sided paired t-test) and −11.8% (putamen versus GTi; P < 0.0001) two-sided paired t-test).
D2/3 receptor occupancy results of patients (n = 50) who were under stable antipsychotic treatment (clozapine, olanzapine, quetiapine, or ziprasidone)
Discussion
The SRTM approach has frequently been used by different workgroups to quantify the binding potentials using various PET ligands, also including the high-affinity D2/3 receptor ligand [18F]fallypride (Slifstein et al, 2010; Kessler et al, 2009; Siessmeier et al, 2005). Whereas most of these groups accept the SRTM as a suitable model, they use different scan durations and protocols. This retrospective analysis of 100 FP scans reveals some important findings, concerning the sufficient scan duration of FP scans. The estimated time point of the transient equilibrium in untreated subjects (n = 50) and the region with the highest D2 receptor densities (the putamen) was mainly observed within 3 hours; individual inspection of equilibrium times revealed only 2 out of 100 scans (all two under unblocked conditions) that failed to reach a peak for the binding curve in the putamen during 180 minutes acquisition. However, in most scans, equilibrium occurred much earlier. The mean equilibrium time point in the putamen for unblocked subjects, 121 ± 29.6 minutes, suggests that 180 minutes is adequate for FP scanning in most subjects. The subjects in this study included healthy control subjects, patients suffering from schizophrenia, and subjects undergoing deep brain stimulation to treat Tourette?s syndrome. After deep brain stimulation and in schizophrenic patients, D2/3 receptor availability was elevated in various brain regions including the basal ganglia (Laruelle, 1998; Vernaleken et al, 2009). In particular, deep brain stimulation caused BPND elevations that exceeded previously measured BPND values (Vernaleken et al, 2009). However, the outliers mentioned above (equilibrium later than 180 minutes) were subjects from the control group. Within the unblocked group, there was no correlation between BPND and the time to reach equilibrium. This suggests that the present results can be generalized to all subject groups and scan situations. To our knowledge, this is the first systematic publication of equilibrium data for FP.
The main purpose to include the TEM was to estimate the individual time points of transient equilibrium (versus). Though it was not intended to validate the SRTM by the less appropriate TEM, it is noteworthy that there were significant correlations and linear regression slopes of ∼0.9 in all regions under both conditions (AP medication and drug free). By definition, such comparisons are only possible when a graphical detection of a transient equilibrium state was possible. A crucial constraint of the TEM is the assumption that the kinetics of nonspecific binding is the same for the reference as well as for the target region. Remarkably, the variability between the two methods was much lower (3.8%) than the test-retest variability (6.1% to 7.9%) reported by Mukherjee et al (2002). Possibly, these considerable TEM/SRTM intercorrelations may hint toward the fact that the time course of the nonspecific binding is indeed similar in the cerebellum and the VOI regions.
As a limitation, this investigation did not provide 2TCM data due to the absence of arterial blood sampling. However, in a previous study comparing the SRTM and 2TCM in 10 subjects (also part of the present sample), while there was a high correlation between analytical methods (r = 0.95), there was a significant elevation of BPND values measured by the 2TCM (Siessmeier et al, 2005). Similar differences in the extent of BPND values have been reported in other studies (Slifstein et al, 2010). However, the differences between the SRTM and 2TCM are comparable in regions with high and low D2/3 receptor binding (10% to 15%).
Low cerebellar-specific ligand binding may cause a bias in reference tissue-based BPND calculations. The effects of specific binding in reference tissue on the estimation of occupancy have been studied previously (Asselin et al, 2007; Pinborg et al, 2007). Based on the BPND calculated by V as V/VF+NS–1, and assuming the regional drug-induced occupancies are same across all brain tissues including the ?reference tissue,? then the apparent occupancy is underestimated as Occapp = Occ/(1 + (1-Occ) × BPND (baseline, cerebellum)), where Occ is the true occupancy (see Asselin et al, 2007, Eq. A13). Thus, the underestimation in occupancies increases as BPND in the reference tissue increases. As depicted in detail by Asselin et al (2007), this effect may cause underestimation of BPND by > 50% in the case of [11C]FLB457. This also confirmed by published [123I]epidepride data (Pinborg et al, 2007). In contrast, for FP, there are no data supporting differences of a similar extent. A comparison of FP and [11C]FLB457 suggests that FP is less vulnerable to cerebellar receptor binding (Vandehey et al, 2010). These authors argue and illustrate by simulation that in case of [11C]FLB457 a higher plasma clearance and the observed lower k2 and koff as well as the higher affinity contribute to its higher extent of specific cerebellar binding compared with FP. A relatively low proportion of lipophilic metabolites (> 20% after 100 minutes) was reported both for FP and [11C]FLB457, with little effect on parameter estimations (Vandehey et al, 2010). Congruently, for FP, the comparison of 2TCM and SRTM never revealed BPND differences of much > 15% as mentioned previously (Siessmeier et al, 2005; Slifstein et al, 2010). As illustrated by Asselin et al (2007), a possible effect of specific cerebellar FP binding on drug-associated occupancy calculations should be similar for all VOIs, as long as confounding factors of ligand binding (e.g., AP action or stimulation of dopamine release) affect the specific ligand binding in cerebellar and cerebral regions to a similar extent. Finally, another factor may account for miscalculations of outcome parameters using the TEM. We cannot exclude that in different regions of the brain (i.e., reference region versus regions with specific binding) the kinetics of free and unspecifically bound ligands can differ.
Insufficient scan durations, however, would definitely cause spatial selective miscalculations depending on the corresponding regional receptor densities. Previously, Olsson and Farde (2001) mentioned that the high-affinity D2/3 receptor ligand, 11C-labeled FLB457, is not suitable for these investigations because of its short half-life. However, concerns over FP also arose because of the potential for failure to reach equilibrium conditions, which would cause an underestimation of BPND in striatal regions (Vernaleken et al, 2010).
Using TEM, we showed that transient equilibrium conditions were fulfilled for nearly all of the scans. The high correlations between the SRTM and TEM in all regions (in the validated presence of a transient equilibrium) do not suggest any bias in SRTM-BPND calculation caused by improper scan durations. However, for reliable estimations of sufficient scan durations, an analysis of artificially reduced scan durations is necessary. This was recently performed for SRTM analyses of [11C]raclopride and [11C]FLB457 (Ikoma et al, 2008). In the present study, we artificially reduced the putamen input values of the SRTM stepwise from 180 to 120 minutes; the effect on BPND values was surprisingly minimal. The first 10 minutes reduction caused a BPND reduction in the putamen of only −0.13 (−0.58%). The BPND difference per 10 minutes time reduction increased with further shortening of the scan time up to −0.25 (−1.16%). This increase is expected, because for most of the subjects, the scan duration approximates the time point of equilibrium or even falls below it. Consequently, the error induced by reduced scan duration was strongly associated with the time of equilibrium. The data also suggest that further increase of the scan duration would not cause any relevant change to the BPND values of high-binding regions (far less than 0.5% per 10 minutes block asymptotically approximating 0%). Thus, our results confirm the significant influence of scan duration on BPND estimates obtained with the SRTM. However, they also illustrate that the extent of miscalculation is very low for FP scans of 180 minutes, even in the critical subset of subjects that have a later occurrence of transient equilibrium than the mean of 120 minutes. As mentioned previously, shorter scan duration can help to avoid breaks in the scan protocol as well as head movements caused by the subject?s increasingly realized inconvenience during the PET scan. Thus, hypothetically, the possibility of scan duration shorter than 180 minutes may be beneficial and needs to be discussed. As depicted by Figure 3A, the scan-time reduction from 180 to 170 minutes causes only little changes in the BPND measures (−0.58%). After 30 minutes, the average difference raises to −1.05% per 10-minute interval finally leading to −1.12% after an hour of scan-time reduction. This effect is mainly driven by results of subjects with later time points of transient equilibrium. A further reduction of the scan times would in realiter remarkably increase the number of individuals that fail to reach this state of equilibrium (six subjects after reduction to 150 minutes and 21 subjects in case of 2-hour scans). Thus, the data do not suggest a scan duration of < 3 hours.
Many PET studies using high-affinity ligands have been performed to characterize the D2/3 receptor-binding properties of various APs. Some, but not all, investigations of second-generation antipsychotics report increased receptor binding in extrastriatal regions compared with striatal binding (Frankle, 2007). All PET studies describing this preferential extrastriatal binding effect have been performed using FP as the radioligand. In our previous investigations using quetiapine, ziprasidone, and clozapine (Gründer et al, 2006; Vernaleken et al, 2008b, 2010), we found an overall elevation of + 26% in D2/3 receptor binding in the GTi compared with that in the putamen (55.2% versus 43.7%; GTi versus putamen) using the SRTM. The difference in occupancy values calculated by the TEM was comparable. If the BPND values of unblocked putamen or caudate nucleus are systematically biased by improper scan durations, this would cause relevant and region-specific errors of D2/3 receptor occupancy estimations. The present results do not suggest a relevant methodological bias—at least none caused by insufficient scan durations: reducing scan time by 10 minutes increased the differences only by 0.3%. This small but significant effect is most likely due to the fact that the sensitivity of BPND calculations regarding scan-time reductions was present only in unblocked striatal regions (later time point of transient equilibrium) but could neither be observed under blocked conditions nor in regions with low D2/3 receptor density. On extrapolating a change of 0.58% per 10 minutes block to a scan duration of 4 hours, even after neglecting the asymptotic reduction of this effect, significant preferential extrastriatal binding observation would still remain. Thus, the preferential extrastriatal binding of APs with low or moderate affinity for the D2/3 receptor does not appear to be a methodological artifact caused by improper scan duration.
The calculation of the AP-induced D2/3 receptor occupancies was based on the comparison with the unmedicated control group but not on individual pre/posttreatment comparisons. Because of the comparatively large interindividual variability of the binding potential under unblocked conditions, this may cause miscalculations of receptor occupancies on the individual level and can affect correlations with other individual measures (e.g., drug plasma level). The mean occupancy levels as well as the average regional differences in drug binding should be unaffected by this procedure.
We furthermore compared the occupancy values obtained by the SRTM and TEM, and calculated the effect of scan-time reduction on the occupancy values. In the comparison of D2/3 receptor occupancy results measured by SRTM versus TEM, it needs to be mentioned that we found significant discrepancies between the TEM and SRTM for the thalamus VOI. The observed 33% reduction in drug binding in the thalamus compared with the putamen using the TEM shrank to a 20% difference when using the SRTM; that was nevertheless statistically significant. This decrease was most likely caused by fitting problems of the blocked thalamus TAC. Inspection of these curves showed that the Hoerl function was unable to perfectly describe this kind of measure. However, in general, the SRTM results are in line with the TEM data. Both the methods suggest preferential extrastriatal binding.
In summary, to the best of our knowledge, this post hoc analysis includes the largest sample of FP data sets thus far. Justifying our chosen time duration for FP-PET scans (180 minutes), we found only a negligible number of scans that exceeded the 180-minute limit in respect to transient equilibrium. Neither the time point of equilibrium nor the choice of the reference method had any relevant influence on BPND or occupancy values. Three hours FP-data acquisition is sufficient to reliably calculate the D2/3 receptor availability using the SRTM and TEM. A limitation of this study is the lack of compartment analysis in the absence of arterial input functions in most subjects.
Footnotes
Acknowledgements
The authors thank Sabine Höhnemann and Markus Piel for performing the [18F]fallypride radiosynthesis. These scans were funded in part by Pfizer, Karlsruhe, Germany, IZKF (TV-N 67), and the German Research Council (DFG, Grant KFO 112/10).
Dr Ingo Vernaleken has served on the speakers' bureaus of Bristol-Myers Squibb (New York, NY, USA), Eli Lilly (Indianapolis, IN, USA), and Glaxo-SmithKline (London, UK). Dr Gründer has served as a consultant for Astra Zeneca (London, UK), Bristol-Myers Squibb (New York, NY, USA), Johnson & Johnson (Beerse, Belgium), Lundbeck (Copenhagen, Denmark), Otsuka (Rockville, MD, USA), and Pfizer (New York, NY, USA). He has served on the speakers' bureaus of Astra Zeneca, Bristol-Myers Squibb, Eli Lilly, Janssen Cilag, Otsuka, Pfizer, Servier (Paris, France), and Wyeth (Madison, NJ, USA). He has received grant support from Alkermes (Cambridge, MA, USA), Bristol-Myers Squibb, Eli Lilly, Johnson & Johnson, and Pfizer. Dr Dean F. Wong has received grant support from the NIH, Amgen, Avid, the DANA Foundation, Intracellular, Johnson & Johnson, Otsuka, Lilly, Lundbeck, Merck, Orexigen, Roche, and Sanofi Aventis. Dr Wolfgang Schaefer has served as a consultant for GE Healthcare Buchler (München, Germany), Siemens Medical Solutions (Erlangen, Germany), Philips (Aachen, Germany), and Bristol-Myers Squibb (München, Germany). He has received grant support from Mediso Medical Imaging Systems (Budapest, Hungary).
References
1.
AsselinMCMontgomeryAJGrasbyPMHumeSP (2007) Quantification of PET studies with the very high-affinity dopamine D2/D3 receptor ligand [11C]FLB 457: re-evaluation of the validity of using a cerebellar reference region. J Cereb Blood Flow Metab27:378–92
2.
BuchertRThieleF (2008) The simplified reference tissue model for SPECT/PET brain receptor studies. Interpretation of its parameters. Nuklearmedizin47:167–74
3.
FardeLErikssonLBlomquistGHalldinC (1989) Kinetic analysis of central [11C]raclopride binding to D2-dopamine receptors studied by PET–a comparison to the equilibrium analysis. J Cereb Blood Flow Metab9:696–708
4.
FrankleWG (2007) Neuroreceptor imaging studies in schizophrenia. Harvard Rev Psychiat15:212–32
5.
GründerGLandvogtCVernalekenIBuchholzHGOndracekJSiessmeierTHärtterSSchreckenbergerMStoeterPHiemkeCRöschFWongDFBartensteinP (2006) The striatal and extrastriatal D2/D3 receptor-binding profile of clozapine in patients with schizophrenia. Neuropsychopharmacology31:1027–35
6.
GründerGSiessmeierTPielMVernalekenIBuchholzHGZhouYHiemkeCWongDFRöschFBartensteinP (2003) Quantification of D2-like dopamine receptors in the human brain with 18F-desmethoxyfallypride. J Nucl Med44:109–16
7.
HamacherKCoenenHHStocklinG (1986) Efficient stereospecific synthesis of no-carrier-added 2-[18F]-fluoro-2-deoxy-D-glucose using aminopolyether supported nucleophilic substitution. J Nucl Med27:235–8
8.
IkomaYItoHArakawaROkumuraMSekiCShidaharaMTakahashiHKimuraYKannoISuharaT (2008) Error analysis for PET measurement of dopamine D2 receptor occupancy by antipsychotics with [11C]raclopride and [11C]FLB 457. Neuroimage42:1285–94
9.
ItoHHietalaJBlomqvistGHalldinCFardeL (1998) Comparison of the transient equilibrium and continuous infusion method for quantitative PET analysis of [11C]raclopride binding. J Cereb Blood Flow Metab18:941–50
10.
KesslerRMWoodwardNDRiccardiPLiRSib AnsariMAndersonSDawantBZaldDMeltzerHY (2009) Dopamine D2 receptor levels in striatum, thalamus, substantia nigra, limbic regions, and cortex in schizophrenic subjects. Biol Psychiatry65:1024–31
11.
LammertsmaAAHumeSP (1996) Simplified reference tissue model for PET receptor studies. Neuroimage4:153–8
12.
LaruelleM (1998) Imaging dopamine transmission in schizophrenia. A review and meta-analysis. Q J Nucl Med Mol Imag42:211–21
13.
MukherjeeJChristianBTDuniganKAShiBNarayananTKSatterMMantilJ (2002) Brain imaging of 18F-fallypride in normal volunteers: blood analysis, distribution, test-retest studies, and preliminary assessment of sensitivity to aging effects on dopamine D-2/D-3 receptors. Synapse46:170–88
14.
MukherjeeJYangZYDasMKBrownT (1995) Fluorinated benzamide neuroleptics—III. Development of (S)-N-[(1-allyl-2-pyrrolidinyl)methyl]-5-(3-[18F]fluoropropyl)-2, 3-dimethoxybenzamide as an improved dopamine D-2 receptor tracer. Nucl Med Biol22:283–96
15.
OlssonHFardeL (2001) Potentials and pitfalls using high affinity radioligands in PET and SPET determinations on regional drug induced D2 receptor occupancy–a simulation study based on experimental data. Neuroimage14:936–45
16.
PinborgLHVidebaekCZiebellMMackeprangTFribergLRasmussenHKnudsenGMGlenthojBY (2007) [123I]Epidepride binding to cerebellar dopamine D2/D3 receptors is displacable: implications for the use of cerebellum as a reference region. Neuroimage34:1450–3
17.
SiessmeierTZhouYBuchholzHGLandvogtCVernalekenIPielMSchirrmacherRRöschFSchreckenbergerMWongDFCummingPGründerGBartensteinP (2005) Parametric mapping of binding in human brain of D2 receptor ligands of different affinities. J Nucl Med46:964–72
18.
SilvaWPSilvaCM (1999-2008) LAB Fit Curve Fitting Software (Nonlinear Regression and Treatment of Data Program): Universidade Federal de Campina Grande, Paraiba, Brazil; available at: http://www.labfit.net
19.
SlifsteinMKegelesLSXuXThompsonJLUrbanNCastrillonJHackettEBaeSALaruelleMAbi-DarghamA (2010) Striatal and extrastriatal dopamine release measured with PET and [(18)F] fallypride. Synapse64:350–62
20.
VandeheyNTMoiranoJMConverseAKHodenJEMukherjeeJMuraliDNicklesRJDavidsonRJSchneiderMLChristianBT (2010) High-affinity dopamine D2/D3 PET radioligands 18F-fallypride and 11C-FLB457: a comparison of kinetics in extrastriatal regions using a multiple-injection protocol. J Cereb Blood Flow Metab30:994–1007
21.
VernalekenICummingPGründerG (2008a) Imaging studies—differential action of typical and atypical antipsychotics in a network perspective. Pharmacopsychiatry41(Suppl 1):S60–9
22.
VernalekenIFellowsCJanouschekHBröchelerAVeselinovicTLandvogtCBoyCBuchholzHGSpreckelmeyerKBartensteinPCummingPHiemkeCRöschFSchaeferWWongDFGründerG (2008b) Striatal and extrastriatal D2/D3-receptor-binding properties of ziprasidone: a positron emission tomography study with [18F]Fallypride and [11C]raclopride (D2/D3-receptor occupancy of ziprasidone). J Clin Psychopharmacol28:608–17
23.
VernalekenIJanouschekHRaptisMHellmannSVeselinovicTBröchelerABoyCCummingPHiemkeCRöschFSchaeferWMGründerG (2010) Dopamine D2/3 receptor occupancy by quetiapine in striatal and extrastriatal areas. Int J Neuropsychopharmacol13:951–60
24.
VernalekenIKuhnJLenartzDRaptisMHuffWJanouschekHNeunerISchaeferWMGründerGSturmV (2009) Bithalamical deep brain stimulation in Tourette syndrome is associated with reduction in dopaminergic transmission. Biol Psychiatry66:e15–7
25.
WoodsRPCherrySRMazziottaJC (1992) Rapid automated algorithm for aligning and reslicing PET images. J Comput Assist Tomogr16:620–33