
Abstract
Limited evidence exists on the relationships between severity of white-matter lesions (WMLs) and cerebral hemodynamics in patients without major cerebral artery disease. To examine changes of cerebral blood flow (CBF), oxygen metabolism, and vascular reserve capacity associated with severity of WML in patients with lacunar stroke, we used a positron emission tomography (PET). Eighteen lacunar patients were divided into two groups according to the severity of WMLs, assessed by Fazekas classification; grades 0 to 1 as mild WML group and grades 2 to 3 as severe WML group. Rapid dual autoradiography was performed with 15O-labeled gas-PET followed by 15O-labeled water-PET with acetazolamide (ACZ) challenge. Compared with the mild WML group, the severe WML group showed lower CBF (20.6 ± 4.4 versus 29.9 ± 8.2 mL/100 g per minute,
Keywords
Introduction
White-matter lesions (WMLs), observed as white-mater hyperintensity in T2-weighted magnetic resonance imaging or fluid-attenuated inversion recovery (FLAIR) image, are commonly observed among elderly people (Hachinski et al, 1987). However, they are also associated with hypertension, diabetes, and other vascular risk factors (Murray et al, 2005; Pantoni and Garcia, 1997). Development of WMLs is known to be a cause of cognitive impairment, dementia, and disability (Prins et al, 2005). Recent studies showed that WMLs are not only a stroke risk factor (Streifler et al, 2002) but also a predictor of unfavorable stroke outcome (Koton et al, 2009). Despite accumulating evidence of the clinical significance of WMLs, the pathogenesis of WMLs has not been fully clarified.
Healthy elderly subjects with severe WMLs were reported to have reduced cerebral blood flow (CBF) and preservation of oxygen metabolism (Meguro et al, 1990). Patients with dementia of the Binswanger type have marked decrease of both CBF and oxygen metabolism in the white matter; however, patients without dementia have a lesser decrease in CBF with preservation of almost-normal oxygen metabolism (Yao et al, 1992). These findings indicated that chronic hypoperfusion due to the progression of small artery disease is associated with the development of WMLs. In addition, hemodynamic disturbance induced by internal carotid artery occlusive disease was suggested to contribute to the development of extensive WMLs (Yamauchi et al, 1999).
Limited evidence exists on the relationships between severity of WMLs and hemodynamic disturbance in patients without major cerebral artery occlusive disease. Some studies showed that vascular reactivity was not related to severity of WMLs (Birns et al, 2009; Turc et al, 1994). Other studies reported that vascular reactivity in patients with severe WMLs is impaired (Bakker et al, 1999; Chabriat et al, 2000; Fu et al, 2006; Isaka et al, 1994; Kozera et al, 2010; Mochizuki et al, 1997). These inconsistencies may be due to differences in modalities for evaluation of vascular reserve capacity; i.e., transcranial Doppler ultrasound (Bakker et al, 1999; Birns et al, 2009; Fu et al, 2006; Kozera et al, 2010), perfusion MRI (Chabriat et al, 2000), xenon inhalation computed tomography (Isaka et al, 1994; Mochizuki et al, 1997), and single photon emission computed tomography (Turc et al, 1994). There are also differences in the vasodilatory stimulus used; i.e., CO2 inhalation (Bakker et al, 1999), breath holding, hyperventilation tests (Birns et al, 2009; Kozera et al, 2010), and acetazolamide (ACZ) challenge test (Chabriat et al, 2000; Fu et al, 2006; Isaka et al, 1994; Mochizuki et al, 1997; Turc et al, 1994). Although single photon emission computed tomography study with ACZ challenge can detect stage II hemodynamic failure (Powers, 1991) by positron emission tomography (PET) in patients with major cerebral artery occlusive disease (Hirano et al, 1994), the relationship between ACZ reactivity and oxygen metabolism in patients with WMLs without major artery disease has not been elucidated. We hypothesized that either impairment of vascular reserve capacity or chronic hypoperfusion in the white matter contributes to the development of WMLs without major artery disease.
The aim of this study was to examine the changes of CBF, oxygen metabolism, and vascular reserve capacity associated with the severity of WMLs in patients with lacunar stroke.
Materials and methods
Patients
This study was a single-center hospital-based prospective study. The study protocol was governed by the guidelines of national government based on the Helsinki Declaration revised in 1983, and it was approved by the Institutional Research and Ethics Committee of our hospital. All patients gave written informed consent to participate in the study. Patients with lacunar stroke, at least 3 weeks after the onset, were enrolled between April 2009 and April 2010. All patients underwent PET studies with 15O-labeled gas (C15O2, 15O2, C15O) inhalation and 15O-water with ACZ challenge autoradiography as described previously (Kudomi et al, 2005, 2007), as well as MRI studies. Lacunar stroke was defined as a typical clinical syndrome associated with a small infarct, <15 mm in diameter on MRI, restricted to the territory of a perforating artery without adjacent major artery occlusive lesions. Patients with stenosis (> 50% in diameter) or occlusion of the internal carotid artery or the trunk of the middle cerebral artery on magnetic resonance angiography or ultrasonography were excluded from the study. The median time interval between the onset of stroke and PET studies was 1,017 days (interquatile range 519 to 1,856).
Baseline clinical characteristics including age, sex, hypertension, diabetes mellitus, dyslipidemia, and current smoking were recorded. Information of risk factors and medical history was collected from a self-reported medical history or inferred from prescribed medication by the primary physicians. Criteria for hypertension, diabetes mellitus, and dyslipidemia were as previously defined (Yokota et al, 2009). Cognitive function was evaluated in all patients by the mini-mental state examination (Folstein et al, 1975) and clinical dementia rating (Hughes et al, 1982). Dementia was defined as clinical dementia rating ≥ 1, and patients with dementia met the criteria proposed by National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association (NINCDS-ADRDA Alzheimer's Criteria) (Roman et al, 1993).
Magnetic Resonance Imaging
Magnetic resonance imaging was performed on a 1.5-T scanner (Magnetom Vision or Magnetom Sonata; Siemens Medical Systems, Erlangen, Germany). The imaging protocol consisted of a T1-weighted spin-echo, a T2-weighted spin-echo, and FLAIR image. Severity of WMLs was assessed using the FLAIR (repetition time 900 ms, echo time 119 ms, field-of-view 230 × 201 mm2 matrix 256 × 210, 4 mm slice thickness, and 2 mm gap between slices).
Two investigators (CY and TN), who were unaware of all clinical data, graded the degree of severity of WMLs by visual inspection using the Fazekas classification of WMLs as follows: none (grade 0), punctate (grade 1), early confluent (grade 2), and confluent lesions (grade 3) (Fazekas et al, 1987). The patients with grades 0 to 1 were defined as the mild WMLs group and those with grades 2 to 3 were defined as the severe WMLs group. Additionally, WMLs volume was measured manually based on FLAIR imaging (20 slices) using Dr View/LINUX software (AJS, Ver R2.5, Tokyo, Japan).
Positron Emission Tomography Imaging
We used an ECAT47 PET scanner (Siemens Medical Systems), which provided an intrinsic spatial resolution of 4.5 mm full-width at half-maximum at the center of the field-of-view. Data were acquired in 2D mode, and corrected for scatter compensation. A catheter was placed in the brachial artery for continuous monitoring of the arterial blood radioactivity concentration and arterial input function using a scintillator block detector system (BeCON; Molecular Imaging Labo, Suita, Japan) (Kudomi et al, 2003).
Quantitative images of CBF and oxygen extraction fraction (OEF) were obtained from a series of PET scans with 15O-labeled gas (C15O2, 15O2, and C15O) inhalation after a rapid dual autoradiography protocol as reported in a series of publications by Kudomi
Additionally, two sets of PET scans were performed, each followed with 15O-labeled water injection to assess regional CBF images using 15O-water autoradiography (Kanno et al, 1987). The first scan was initiated without any pharmacological or physiological stress (at rest) and the second scan was performed at 10 minutes after an intravenous injection of ACZ titrated to 17 mg/kg. Physiological and laboratory data such as blood pressure, heart rate, and blood gas analysis (Siemens RAPIDLab 1265; Siemens Medical Systems) were obtained during the PET study.
Data Analysis
The small circular regions of interest (ROIs) (10 mm in diameter) were placed in the frontal cortex, parietal cortex, occipital cortex, basal ganglia, and centrum semiovale based on automatic registration of MRI to PET by using PVElab (the PVEOut Consortium) (Quarantelli et al, 2004; Svarer et al, 2005). The program is followed by automatic segmentation (running with Statistical Parametric Mapping 5 (SPM5) Software (Institute of Neurology, University College of London, London, UK) and correction of PET counts for fractional volume as determined from the segmentation. The ROIs were manually placed on the FLAIR images and transferred to the CBF images for analysis (Figure 1). We defined the ACZ reactivity as the percentage increase in CBF after ACZ administration relative to baseline CBF. In each subject, the mean measures were obtained by averaging the values for both hemispheres.
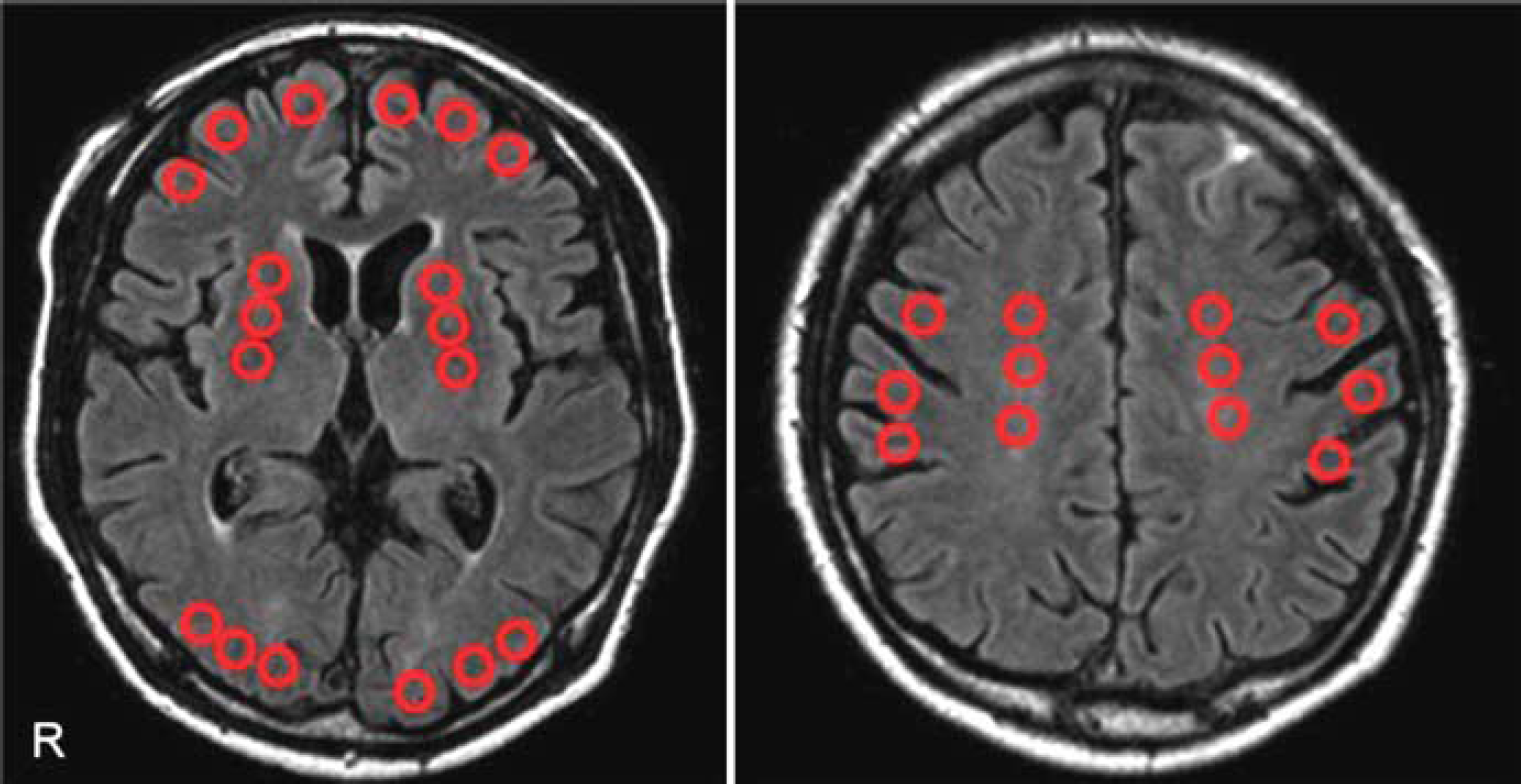
Regions of interest (ROIs) on fluid-attenuated inversion recovery (FLAIR). The small circular ROIs (10 mm in diameter) were placed on the frontal cortex, parietal cortex, occipital cortex, basal ganglia, and the centrum semiovale based on FLAIR image.
Statistical Analysis
Statistical analysis was performed using JMP 7.0 software (SAS Institute, Cary, NC, USA). The statistical significance of inter-group differences was assessed by χ2 tests, unpaired
Results
Patients were divided into two groups of severe WMLs (
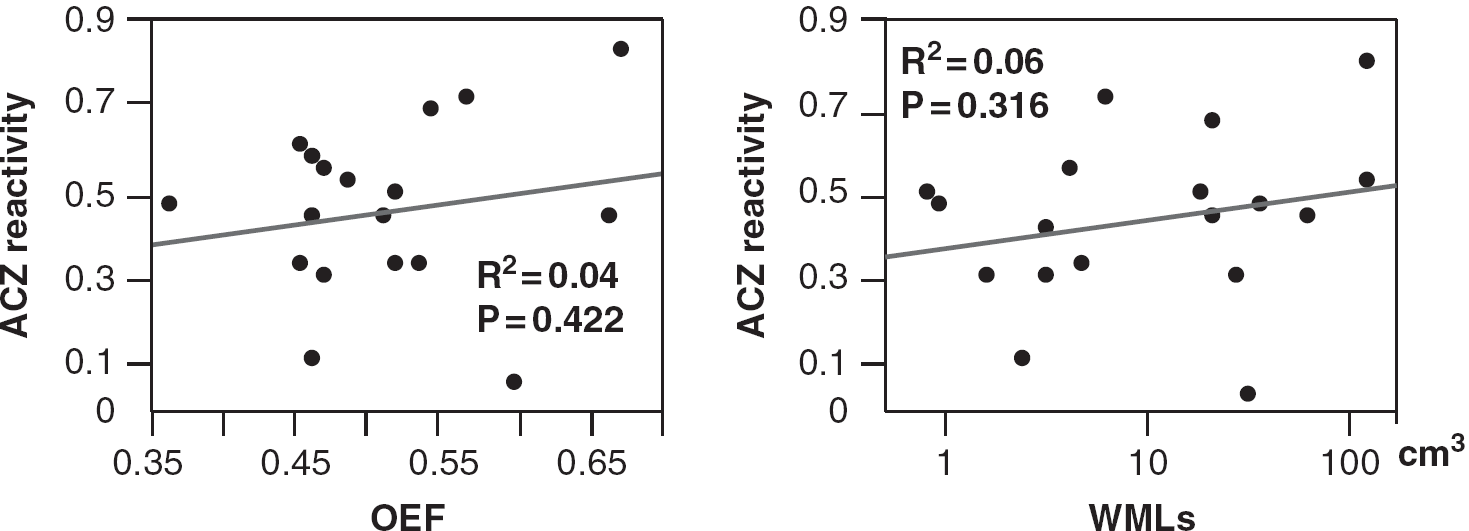
The correlation between ACZ reactivity and OEF or WML volume in the centrum semiovale. Neither OEF nor WML volume was correlated with ACZ reactivity. ACZ, acetazolamide; OEF, oxygen extraction fraction; WMLs, white-matter lesions.
Baseline characteristics
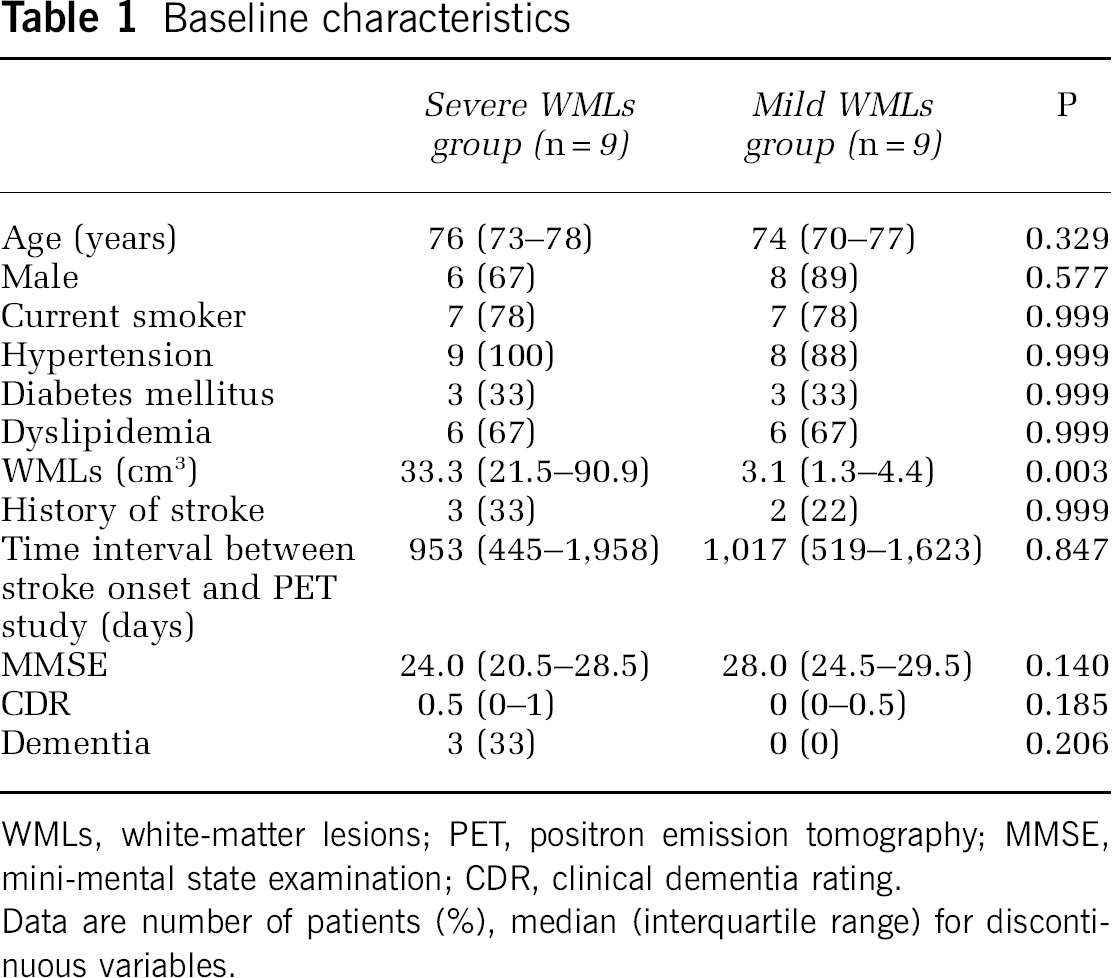
WMLs, white-matter lesions; PET, positron emission tomography; MMSE, mini-mental state examination; CDR, clinical dementia rating.
Data are number of patients (%), median (interquartile range) for discontinuous variables.
Comparison of each parameter of the gas-PET study between patients with severe or mild WMLs in the brain
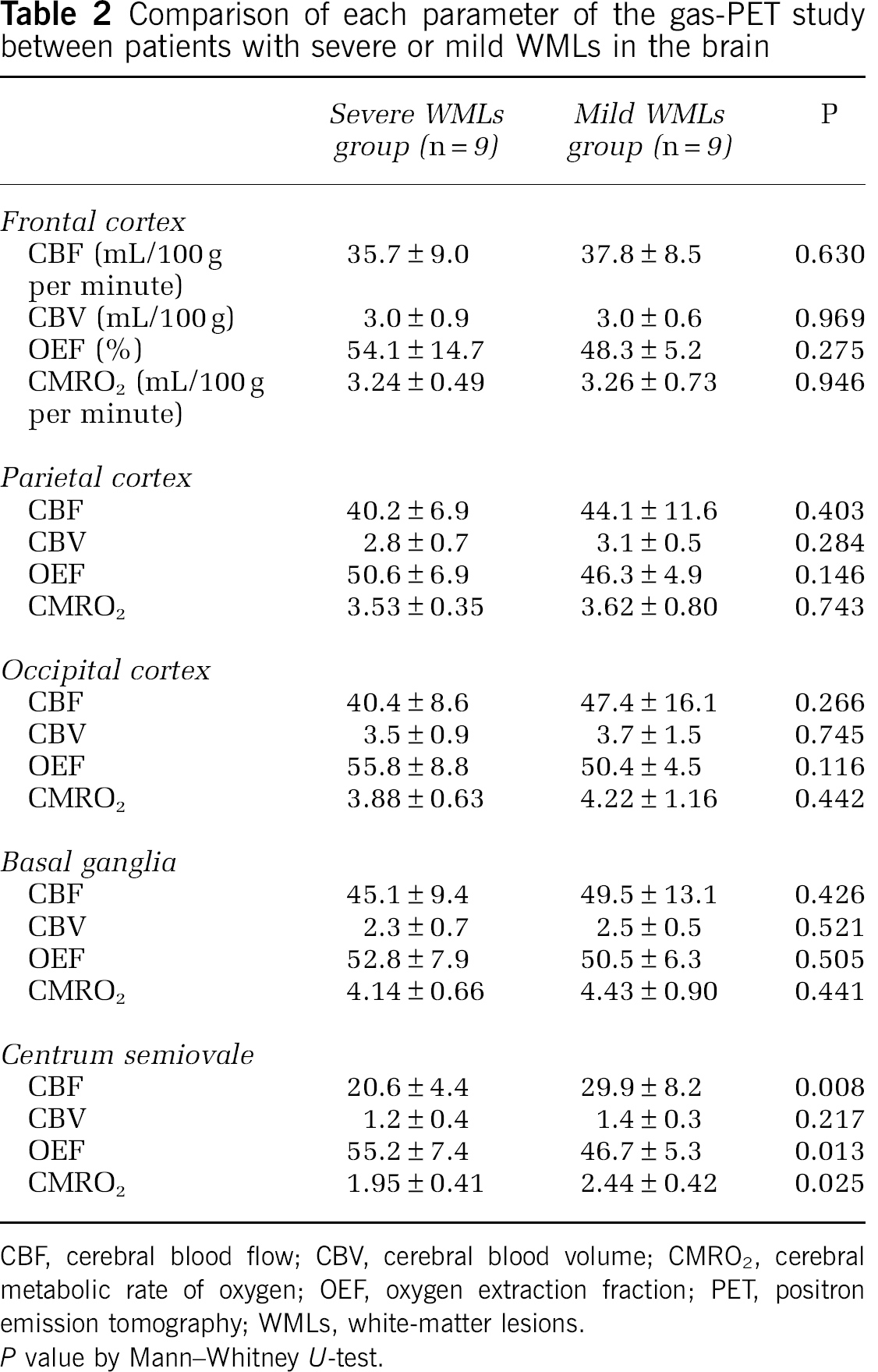
CBF, cerebral blood flow; CBV, cerebral blood volume; CMRO2, cerebral metabolic rate of oxygen; OEF, oxygen extraction fraction; PET, positron emission tomography; WMLs, white-matter lesions.
Comparison of CBF between patients with severe or mild WMLs in the brain by H2O-PET
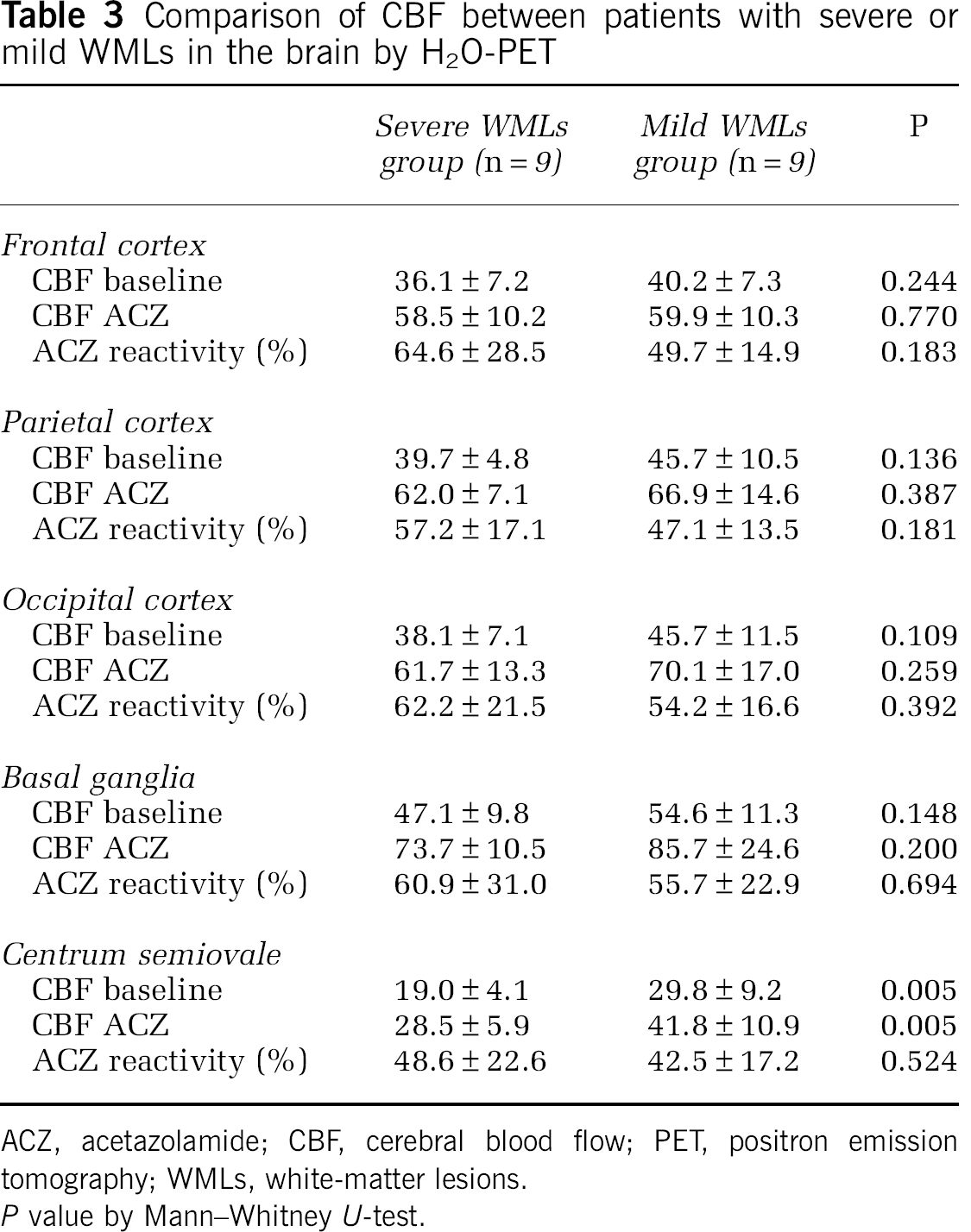
ACZ, acetazolamide; CBF, cerebral blood flow; PET, positron emission tomography; WMLs, white-matter lesions.
Discussion
This study showed reduced CBF, reduced CMRO2, and increased OEF in patients with severe WMLs compared with those with mild WMLs in the centrum semiovale. All patients in this study had lacunar stroke without major cerebral artery disease. The study also showed that ACZ reactivity was not impaired in either the cortex or the white matter of the patients of both groups.
Hatazawa et al (1997) found asymptomatic WMLs subjects exhibited reduction of CBF in the white matter and basal ganglia without decrease in CMRO2. They also observed an increase in OEF in these areas, suggesting a chronic hypoperfusion in these territories. The present study provided additional information of reduction of both CBF and CMRO2 with an increase in OEF in the WML in the patient groups with severe WMLs. Centrum semiovale is located at the border of an area supplied by deep perforating arteries and the terminal branches of the middle cerebral artery. A decrease in CBF with reduction of CMRO2 in the centrum semiovale in the present study should indicate a consequence of a reduced tissue metabolism in this terminal zone.
In the present study, patients with severe WMLs without major artery disease had increased OEF showed by gas-PET; however, their ACZ reactivity by H2O-PET was preserved. The vascular reserve capacity evaluated by ACZ reactivity was preserved in both patients with severe and mild WMLs. Reduction of both CBF and CMRO2 in the white matter was previously shown in patients with the Binswanger type dementia (Yao et al, 1990), being consistent with our results. Postmortem neuropathologic studies have shown decreased neuronal connectivity in the white matter in progressive subcortical vascular encephalopathy of Binswanger type (Yamanouchi et al, 1989, 1990). Functional reduction in cortical neuronal activity due to disruption of connections between the cortex and subcortex, as indicated previously (Pozzilli et al, 1987; Sette et al, 1989), is likely to be associated with a reduction of CMRO2 in the centrum semiovale in the patients with severe WMLs. Furthermore, the cerebral vessels would not dilate during fluctuations in systemic arterial pressure in daily life in these conditions of disruption of connections. Chronic hypoperfusion with a reduction of CMRO2 in accordance with a disconnection between the cortex and subcortex may be the cause of development of WMLs without major artery disease.
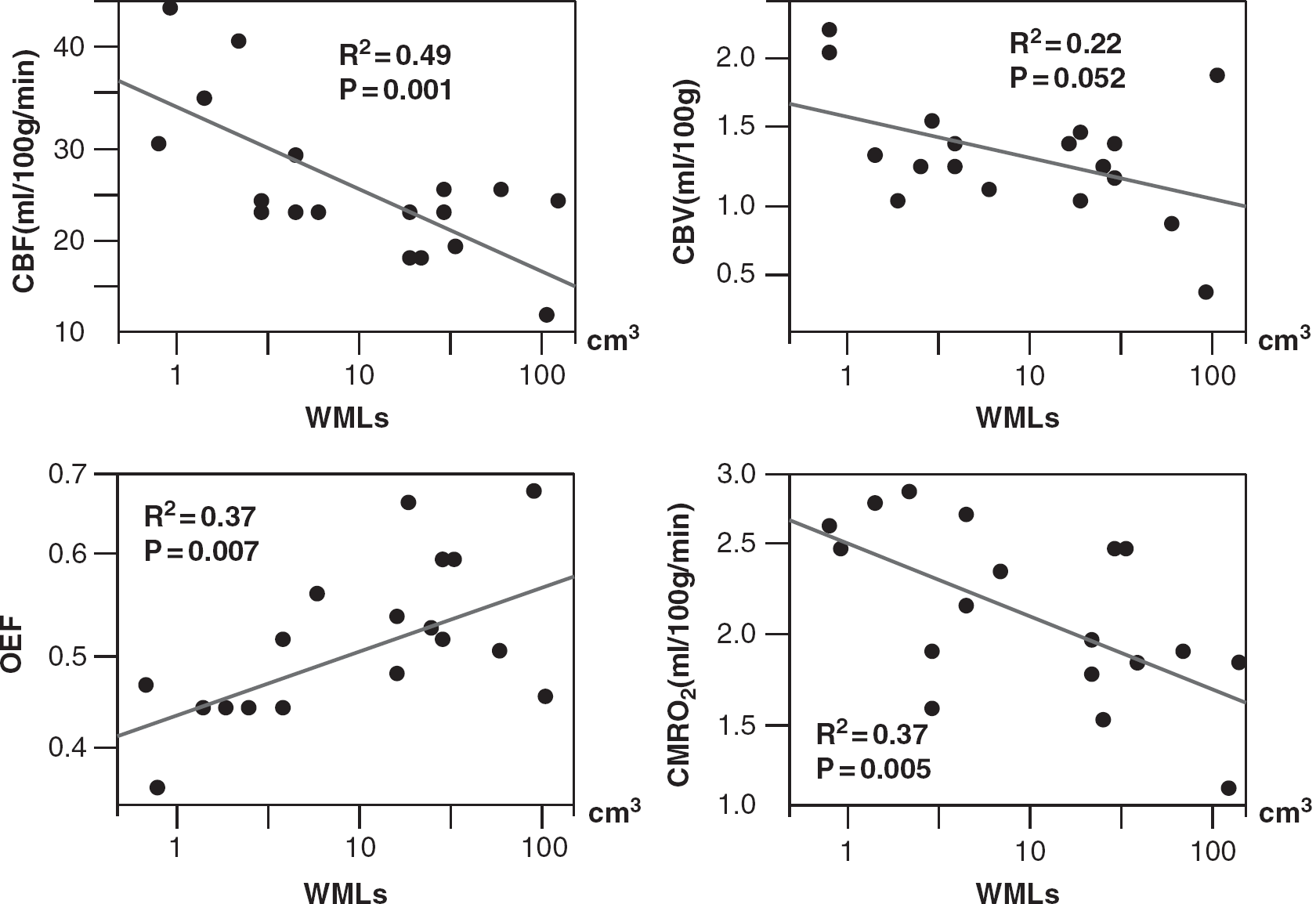
Correlation between WML volume and each gas-PET parameter in the centrum semiovale. CBF and CMRO2 had a negative correlation with the severity of WMLs, while OEF was positively correlated with the severity of WMLs. CBF, cerebral blood flow; CBV, cerebral blood volume; OEF, oxygen extraction fraction; CMRO2, cerebral metabolic rate of oxygen; WMLs, white-matter lesions; PET, positron emission tomography.
To our knowledge, this is the first report of alterations in CBF, CMRO2, and OEF, with preservation of ACZ reactivity in patients with mild or severe WMLs, with careful consideration of possible methodological errors. Indeed, quantitation of physiological parameters using PET is still a challenging issue, particularly in the white-matter area. As shown in earlier studies (Herscovitch and Raichle, 1983; Huang et al, 1987), the absolute values of both CBF and CMRO2 could be biased because the spatial resolution of PET devices is limited compared with the physical size of the brain tissue component, or the partial volume effects. Oxygen extraction fraction is relatively stable and is less affected by partial volume effects. Our observation of increased OEF could not be explained by partial volume effects alone. Scatter is smaller in 2D mode in PET as compared with 3D acquisition. In this study, scatter correction was applied to minimize the contribution of radioactivity from the surrounding tissue components due to scatter. The ROIs were placed carefully with a guide of anatomical MRI to minimize the errors arising from radioactivity counts of surrounding tissues. These factors remain concerns to be dealt with in future investigations.
There are several issues that need to be addressed, as follows. First, we intended to avoid possible bias in the patient selection, but a relatively small number of subjects could cause selection bias despite our efforts. Second, three patients with dementia were enrolled in the severe WMLs group. Because oxygen metabolism in demented patients was reported to be different from that in non-demented patients (Yao et al, 1992), a reduced CMRO2 with reduced CBF in the severe WMLs group could be attributed to secondary effects arising from decreased cognitive function. Third, we examined the vascular reserve capacity by ACZ challenge. Recently, ACZ-induced vasodilation was reported not to inhibit the visually evoked flow response (Yonai et al, 2010), which indicates that the vasodilatory mechanism during neurovascular coupling may be different from the mechanism of ACZ-induced vasodilation. Acetazolamide at a dose of 17 mg/kg would not cause maximal cerebral vasodilatation. However, there were no significant differences in ACZ reactivity between the two groups, and ACZ reactivity was preserved in all patients in the present study. Fourth, PET imaging in the present study was a single scatter subtraction technique based on the Klein—Nishina formulation which was implemented in the reconstruction software (Watson, 2000). This technique was shown to provide reasonable accuracy in several phantom experiments. It should also be noted that the data were acquired in 2D mode, which has much smaller amount of scatter as compared with recently available 3D mode. Further, the filtered-back projection technique was applied for the image reconstruction. In this procedure, the scatter contribution is likely reduced in the reconstructed images. However, limited spatial resolution of PET devices is a significant source of errors that causes possible contamination of radioactivity counts of cortical grey matter tissue. Exact magnitude of errors in the calculated parameters in the WML cannot be well defined. In addition, PET scanning in the present study has not been applied to age-matched normal subjects. Further systematic study is needed.
In conclusion, we showed that there is reduced CBF and CMRO2, and increased OEF in the centrum semiovale of patients with severe WMLs compared with patients with mild WMLs. The ACZ reactivity was preserved in both patients with severe and mild WMLs. Further studies will be needed to clarify the pathogenesis of WMLs.
Footnotes
The authors declare no conflict of interest.