
Abstract
Diffusion-weighted imaging (DWI) is commonly used to assess irreversibly infarcted tissue but its accuracy is challenged by reports of diffusion lesion reversal (DLR). We investigated the frequency and implications for mismatch classification of DLR using imaging from the EPITHET (Echoplanar Imaging Thrombolytic Evaluation Trial) and DEFUSE (Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution) studies. In 119 patients (83 treated with IV tissue plasminogen activator), follow-up images were coregistered to acute diffusion images and the lesions manually outlined to their maximal visual extent in diffusion space. Diffusion lesion reversal was defined as voxels of acute diffusion lesion that corresponded to normal brain at follow-up (i.e., final infarct, leukoaraiosis, and cerebrospinal fluid (CSF) voxels were excluded from consideration). The appearance of DLR was visually checked for artifacts, the volume calculated, and the impact of adjusting baseline diffusion lesion volume for DLR volume on perfusion-diffusion mismatch analyzed. Median DLR volume reduced from 4.4 to 1.5 mL after excluding CSF/leukoaraiosis. Visual inspection verified 8/119 (6.7%) with true DLR, median volume 2.33 mL. Subtracting DLR from acute diffusion volume altered perfusion—diffusion mismatch (
Introduction
Definition of the irreversible infarct core is of critical importance in the assessment of potential risk and benefit associated with thrombolysis in acute ischemic stroke. Diffusion-weighted magnetic resonance imaging (MRI) is the most widely used measure of infarct core. Various MRI methods of selecting patients with salvageable ‘ischemic penumbra’ for reperfusion therapies have been proposed. These include perfusion-diffusion mismatch (Donnan and Davis, 2008; Hjort et al, 2005; Warach, 2002), magnetic resonance angiography—diffusion mismatch (Lansberg et al, 2008), and clinical-diffusion mismatch (Davalos et al, 2004; Ebinger et al, 2009; Lansberg et al, 2007; Prosser et al 2005; Tei et al, 2007). All depend on diffusion-weighted imaging (DWI) for an accurate assessment of infarct core volume. In addition, large infarct core volume has been associated with symptomatic intracerebral hemorrhage (Singer et al, 2008) and is a feature of the ‘malignant profile’ that predicts poor clinical response to thrombolysis (Mlynash et al, 2011). However, a recent review emphasized the uncertainty in the literature about the relationship of diffusion restriction to irreversible injury (Kranz and Eastwood, 2009). An initial analysis of the Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution (DEFUSE) trial imaging data suggested that, on average, 43% of the acute diffusion lesion reversed (Olivot et al, 2009). In a previous analysis of the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET) imaging data, we found that coregistration inaccuracy and infarct atrophy over time were major contributors to apparent diffusion lesion reversal (DLR) and that true DLR in this population of 60 patients 3 to 6 hours after the onset of ischemic stroke was rare (Chemmanam et al, 2010). Nonetheless, the question of reversibility of diffusion lesions remains controversial. Given the importance of this issue to clinical practice, we substantially enlarged the data set by pooling the EPITHET and DEFUSE trials and used an optimized methodology, including analysis of DLR in the early hours following thrombolysis.
Materials and methods
EPITHET was a prospective, double-blind, multicenter trial with acute ischemic stroke patients randomized to IV tissue plasminogen activator (tPA) or placebo 3 to 6 hours after symptom onset. DEFUSE was an open-labeled study of IV tPA for acute ischemic stroke 3 to 6 hours after the symptom onset. Methodological details have been reported previously (Albers et al, 2006; Davis et al, 2008). In brief, in both studies, a baseline noncontrast computed tomography scan was used to exclude patients with acute hemorrhage and major early ischemic change > 1/3 MCA territory. Patients had acute MRI at 1.5 T with DWI, PWI, T2-weighted sequences and magnetic resonance angiography, and clinical assessments, with the National Institutes of Health Stroke Scale performed before the treatment. In EPITHET, these assessments were repeated between days 3 to 5 (subacute) and day 90 (follow-up). In DEFUSE, these assessments were repeated between 3 to 6 hours (subacute) and at day 30 (follow-up) after the treatment. Treatment with tPA (or randomization to tPA/placebo in EPITHET) was carried out without the knowledge of the MRI results, which were analyzed centrally before unblinding, to determine the presence of perfusion-diffusion mismatch. The studies were approved by the institutional review boards at all centers and informed consent was obtained from all the participants.
For this analysis, coregistration of the follow-up images to the acute DWI was performed using MINC tools (Montreal Neurological Institute, McGill University, Montreal, Canada) and judged by two expert imaging scientists. Images that failed to register in the first attempt using a rigid body 3D registration were subjected to a standardized sequence of alternate registration procedures, including manual initialization as well as scaling and shear transforms to correct for echoplanar imaging artifacts. Cases that failed all attempts were excluded from this study. Regions of interest were manually drawn using careful windowing to outline the maximal visual extent of the acute DWI (B1000 trace-weighted) lesion with reference to the apparent diffusion coefficient (ADC) image to avoid regions of T2 shine-through. The B1000 image was used as the primary template as quantitative ADC thresholds tend not to accurately outline the visually evident lesion and have been shown to vary with time after stroke onset and perfusion status (An et al, 2011). Manual regions of interest were also drawn to the maximal extent of the final infarct on the coregistered day 90 T2 (EPITHET) or day 30 fluid attenuated inversion recovery (FLAIR) (DEFUSE) images. This was performed in DWI space to avoid the step artifact sometimes introduced by transforming a binary region of interest.
Apparent DWI lesion reversal was defined as the region of acute DWI lesion that did not lie within the coregistered final infarct at follow-up. The purpose of this analysis was to determine the amount of diffusion-restricted tissue that returns to a normal radiological appearance. We, therefore, limited ‘apparent reversal’ to normal-appearing brain tissue at follow-up by the use of a cerebrospinal fluid (CSF) and gliosis mask created by manual thresholding of the follow-up image. This reduced the impact of infarct atrophy where it led to ex vacuo dilatation of ventricles and sulci, and excluded preexisting gliosis or leukoaraiosis where reversal could not be assessed. Infarct core was defined as the region of acute DWI lesion that lay within the coregistered final infarct. Mismatch was defined as a ratio of perfusion lesion volume (threshold
Assessment of reperfusion was an important cofactor in the analysis. To standardize the assessment of perfusion imaging between trials, all data were reprocessed using a fully automated software package (RAPID, Stanford University), which produced
Finally, all available acute, subacute, and late imaging data were visually reviewed slice-by-slice using interactive image blending of the coregistered images by consensus of a neuroradiologist and stroke neurologist to distinguish cases with ‘true DWI lesion reversal,’ defined as a distinct region of a DWI lesion not included in the follow-up infarct and not attributable to lesion shrinkage or coregistration inaccuracy. Cases with true reversal between acute and 3 to 6 hours posttreatment time points (DEFUSE subgroup only) were carefully examined visually to determine whether the reversal was sustained on follow-up FLAIR. Regions of true DWI lesion reversal were manually outlined and the volume was calculated.
Statistical analysis was performed using PASW (v.18, SPSS, Chicago, IL, USA). Nonparametric (Wilcoxon) testing was applied to the proportion of apparent DWI lesion reversal in baseline perfusion categories and after reperfusion.
Results
Of 175 patients in the pooled EPITHET and DEFUSE studies, there were 119 patients suitable for this analysis of whom 83 were treated with intravenous tPA (Table 1). The reasons for exclusion of patients were absent follow-up imaging (43), no lesion on baseline DWI (8), coregistration failure (4), and withdrawal of consent before baseline imaging (1).
Clinical characteristics of patients (
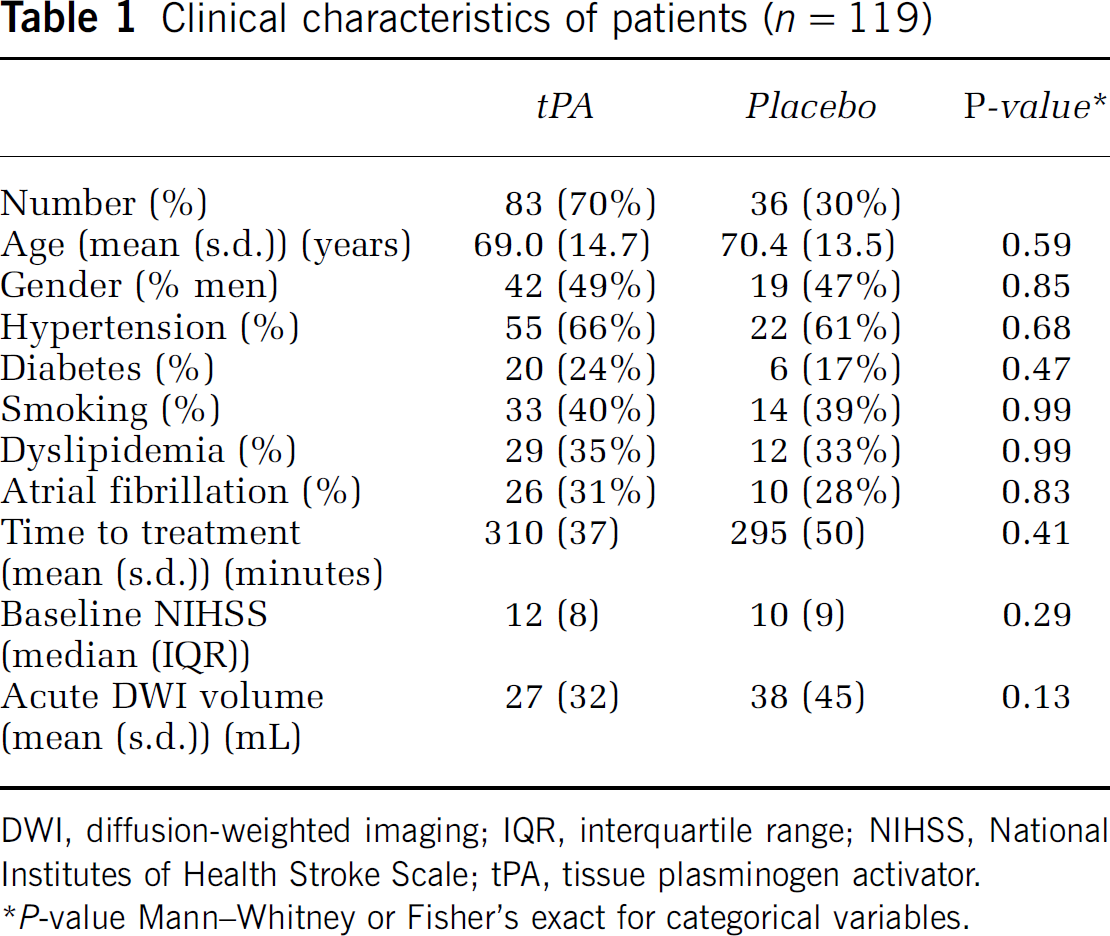
DWI, diffusion-weighted imaging; IQR, interquartile range; NIHSS, National Institutes of Health Stroke Scale; tPA, tissue plasminogen activator.
A CSF/gliosis exclusion mask was utilized to reduce the impact of infarct atrophy, as well as gliosis and leukoaraiosis on the follow-up scan, where reversal could not be reliably assessed (Figure 1). This reduced the median volume of apparent reversal from 4.4 mL (interquartile range 1.6 to 8.1 mL) to 1.5 mL (interquartile range 1.5 to 3.0 mL, paired Wilcoxon,
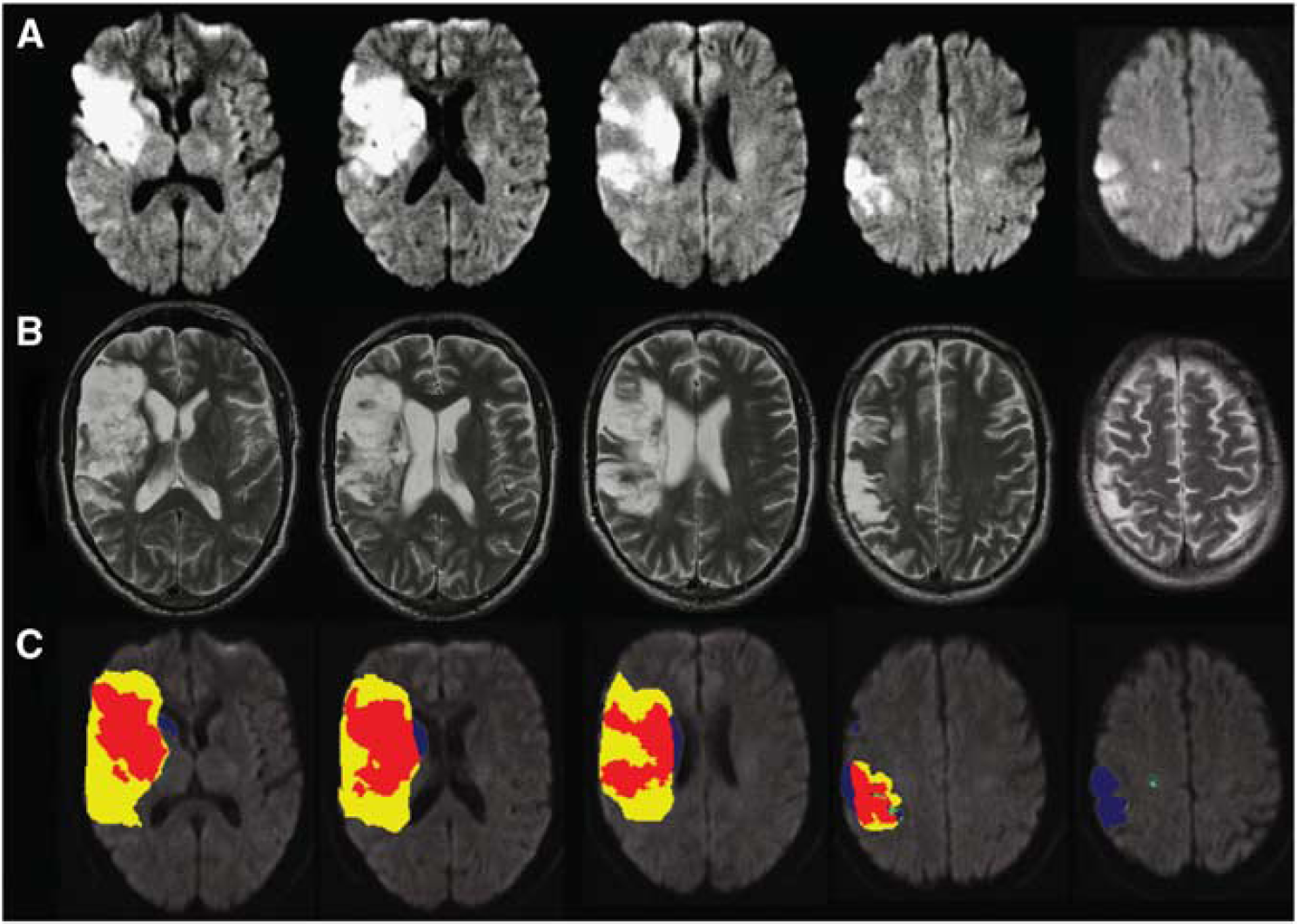
A patient with apparent diffusion lesion reversal due to infarct atrophy (
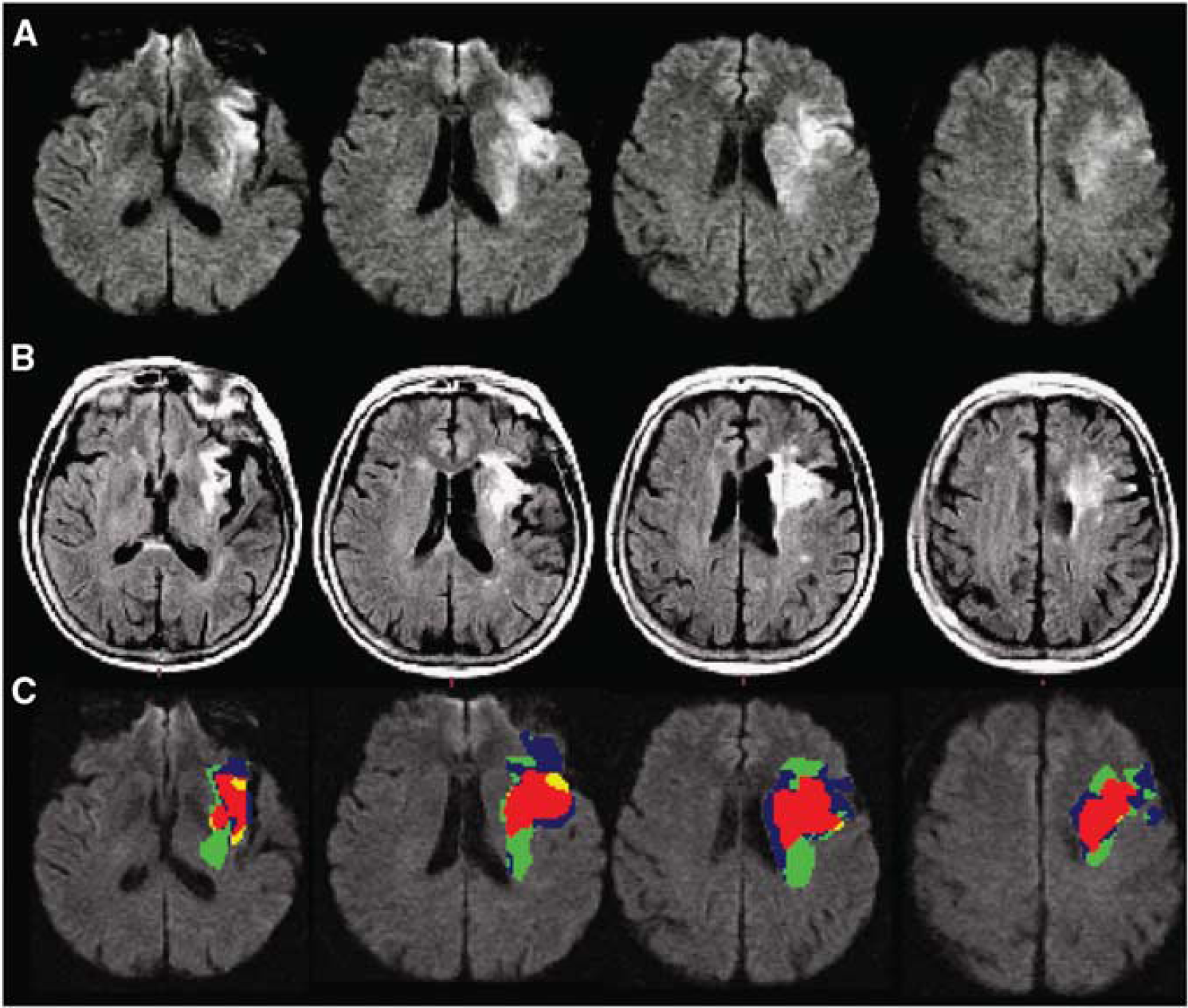
A patient with true diffusion lesion reversal (
Diffusion lesion reversal between baseline and 3 to 6 hours DWI was also reviewed in 65 DEFUSE cases with available data. The median volume of apparent reversal was 1.1 mL (interquartile range 0.64 to 2.5). Adjusting baseline DWI volume for apparent reversal only altered perfusion-diffusion mismatch classification in 2/65 cases (3%). Visual checking verified the reversal in seven cases, all but one of whom had reperfused. The median volume affected in these cases of true ‘acute’ reversal was 4.2 mL. Adjusting baseline DWI for this volume reclassified mismatch in the same single case as in the acute to follow-up analysis. The seven cases of true acute reversal included the only two cases of true permanent reversal identified in the acute to follow-up analysis that had 3 to 6 hours imaging. Importantly, in the other five cases of acute DLR, the region in question had abnormal FLAIR signal at follow-up (Figure 3). Thus, the majority of acute DLR did not translate to permanent tissue salvage.
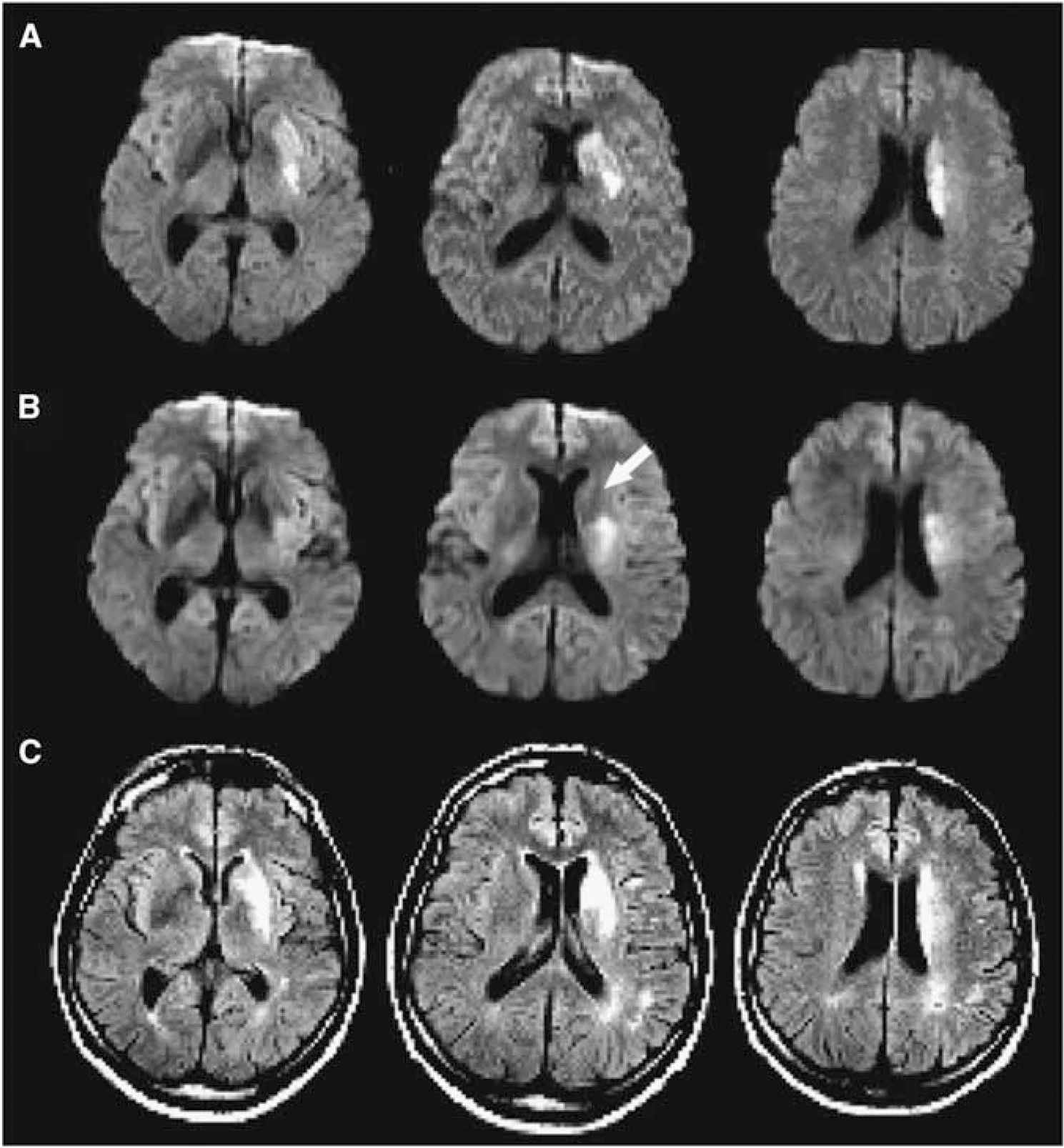
An example of temporary diffusion lesion reversal in a patient who reperfused with tissue plasminogen activator (tPA). (
Discussion
In this study, the largest addressing the issue of DLR after tPA, we found that DLR was uncommon using both a quantitative volumetric approach and a more subjective expert visual assessment. When it did occur, the volume of brain tissue affected was small and unlikely to be clinically relevant. In addition, temporary DLR was observed but, in the majority of cases, did not lead on to true tissue salvage. When permanent diffusion reversal did occur, it was universally associated with early reperfusion and generally affected small volumes of tissue in the deep white matter. These are important findings as the use of MRI-based selection for thrombolysis in extended time windows is increasing, although further validation is required (Mishra et al, 2010). The reliability of infarct core assessment in MRI-based selection depends on the irreversibility of the diffusion lesion. This is regardless of whether the strategy for patient selection is perfusion-diffusion mismatch, magnetic resonance angiography-diffusion mismatch, or clinical-diffusion mismatch. We have demonstrated that the impact of apparent DLR on perfusion-diffusion mismatch classification is minimal.
The determination of DLR is highly dependent on the definition of diffusion abnormality employed. Outlining the diffusion lesion can be performed in a number of ways. However, no automated thresholding approach currently available can reliably segment the entire visually apparent lesion. This relates to heterogeneity of ADC across the individual's brain and between individuals, especially with increasing age (Thomas et al, 2010). The optimal ADC threshold to define infarction also appears to vary with time from stroke onset (An et al, 2011). We have, therefore, used manual outlining, a technique with good reproducibility (Butcher et al, 2008), that leads to regions of interest considerably larger than automated segmentation (Lansberg et al, 2011). This means that DLR volumes in this study are, if anything, overestimated compared with automated segmentation techniques. Likewise, the effect of any coregistration inaccuracy would be to increase the volume of apparent DLR.
A limitation of this study is that interpretation is restricted to patients beyond 3 hours from stroke onset. It is possible that diffusion restriction after less prolonged ischemia may have a degree of reversibility in humans. However, in practical terms, MRI is rarely used to select patients in earlier time windows, given that intravenous tPA is a proven therapy based simply on a noncontrast computed tomography brain (Lees et al, 2010). It could be argued that the exclusion of gliosis and leukoaraiosis on follow-up images biases the results against finding diffusion reversal. However, whether these lesions date from the incident stroke or were preexisting cannot be reliably determined. At any rate, the gliotic tissue is not likely to be functioning normally. The follow-up imaging differed between EPITHET and DEFUSE in both time (90 versus 30 days) and technique (T2 versus FLAIR). However, there is evidence that most infarct atrophy has already occurred by day 30 with minimal further evolution (Gaudinski et al, 2008). Although lesion volumes using T2 and FLAIR may differ slightly, the proportions of apparent DLR after exclusion of CSF and gliosis were very similar between studies (median 14.3% in DEFUSE and 13.8% in EPITHET).
The most impressive reports of DLR have occurred after reperfusion induced by intraarterial therapy (Kidwell et al, 2000). However, in many cases, the initial reversal was transient and did not herald tissue salvage, as the diffusion restriction subsequently returned or FLAIR hyperintensity developed (Kidwell et al, 2002). This is consistent with our study findings that the majority of early DLR was not sustained at follow-up. Indeed, there are important methodological considerations affecting most previous reports of diffusion reversal in humans. In some cases, follow-up was early and fell during a period when temporary reversal is now recognized to be common (Chalela et al, 2004). Other studies used delayed follow-up without accounting for infarct atrophy (Ritzl et al, 2004; Rivers et al, 2006). The imaging modality used for follow-up is also critical as ADC normalizes after a few days and infarct volume using T2 images varies depending on the windowing employed.
The lack of correlation between early DLR and tissue salvage is also supported by animal data. In rats, diffusion restriction after 10 and 30 minutes of ischemia demonstrated initial reversal after reperfusion (Li et al, 2000). The diffusion restriction later returned in the 30-minute group but not the 10-minute group. However, there was histologically evident neuronal loss in both groups of rats. In our study and previous reports (Fiehler et al, 2004), white matter seemed to be more likely to exhibit DLR. This may reflect an increased tolerance to ischemia. It is possible that reversal of diffusion restriction represents a potentially salvageable state and that subsequent return of imaging abnormalities represents a secondary injury (Kidwell et al, 2002). Support for this comes from molecular pathology as cytotoxic edema (the putative substrate of diffusion restriction) is theoretically reversible with restoration of cellular energy status (Simard et al, 2007). Future developments in neuroprotection may allow further investigation of this possibility. However, for the moment, the presence of diffusion restriction can be taken as a clinically reliable indicator of irreversible ischemic damage.
Footnotes
Acknowledgements
tPA was supplied at no charge by Boehringer Ingelheim (Australia, New Zealand, and European sites) and Genentech (US and Canada sites). Neither Boehringer Ingelheim, Genentech nor the NIH played a role in the design and the conduct of the studies; collection, management, analysis, and interpretation of the data; or preparation or approval of the manuscript.
The authors declare no conflict of interest.