
Abstract
Since a pioneer work that has shown in vitro that the rat's fibrinolytic system is 10-fold less sensitive to recombinant tissue-plasminogen activator (rtPA) than the human system, most preclinical studies are performed with 10 instead of 0.9 mg/kg rtPA (the clinical dose in stroke patients). In this study, we compared the effects of these doses on mean time to reperfusion, reperfusion slope, brain infarct volume and edema in a rat model of thrombo-embolic stroke. Our data provide evidence that the dose of 0.9 mg/kg rtPA is as appropriate as that of 10 mg/kg for preclinical stroke studies in rodents.
Introduction
Brain insults that follow disruption of cerebral blood flow still remain a major cause of acute mortality and chronic morbidity. Given the magnitude of the problem, in terms of disability for the affected patients and subsequent financial cost on society, the need and development of new and efficient therapeutic interventions are recognized as a major challenge to minimize the severity of disability and long-term neurological disorders that may result from such critical life events. Two strategies have been pursued for the treatment of ischemic stroke: first, limitation of the primary vascular insult by early reperfusion; second, blockade of the neurotoxic cascade initiated by glutamate (Lee et al, 1999). Until today, the only therapy approved by the Food and Drug Administration and the European Medical Agencies for the treatment of acute ischemic stroke was thrombolysis by the recombinant form of human tissue-type plasminogen activator (tPA), a serine protease that acts by converting the proenzyme plasminogen to the protease plasmin, which is ultimately responsible for the degradation of the thrombus (Lijnen et al, 1980). In contrast, although many drugs have been proven to reduce ischemia-induced brain damage in animal models, most of them have failed to reach clinical trials or, if not, have failed to be efficient in ischemic stroke patients. Consequently, there has been and there is still an enormous effort of research to attempt discovering a drug (compatible with the recombinant tissue-plasminogen activator (rtPA)) that would be really efficient for neuroprotection against cerebral ischemia. However, one of the major difficulties in preclinical studies remains the pertinence of the animal models and protocols used.
Since the work of Korninger and Collen (1981), who have shown in vitro that the rat's fibrinolytic system would be about 10-fold less sensitive to rtPA than the human system, the vast majority of stroke studies in rodents have been performed with 10 mg/kg rtPA instead of 0.9 mg/kg rtPA, which is the clinical dose used in ischemic stroke patients. However, to the best of our knowledge, no or little studies have actually compared the in vivo effects of 0.9 and 10 mg/kg rtPA in rodents. Here, to answer this question, we compared the effects of 0.9 and 10 mg/kg rtPA on cerebral blood flow reperfusion, including mean time to reperfusion and reperfusion slope, infarct volume, and brain tissue edema in rats subjected to a thromboembolic model of middle cerebral artery occlusion (MCAO).
Materials and methods
Male Sprague–Dawley rats weighing 250 to 275 g were subjected to MCAO-induced ischemia by injection of an autologous blood clot by the intraluminal method, in accordance with the framework of the French Legislation for Biomedical Experimentation (agreement no. 14-27) and The European Communities Council Directive of 24 November 1986. At 24 h before the animals were subjected to ischemia, a whole caudal blood sample of 200 μl was withdrawn using PE-50 tubing and allowed to clot at 37°C for 2 h. Then, the clot measuring approximately 0.35 mm in diameter and 120 mm in length was extruded from the catheter into a saline-filled petri dish and stored at 4°C for 22 h before being used to induce thrombo-embolic acute ischemic stroke. On the day of surgery, the rats were anesthetized with 5 vol% isoflurane in medical air, intubated, and ventilated artificially throughout the experiment using an anesthesia ventilator. Isoflurane was reduced at 2 vol% in medical air all along the experiment. Catheters were inserted into the femoral vein to allow injection of rtPA or saline solution, and in the femoral artery for continuous monitoring of heart rate, diastolic, systolic, and mean arterial pressures, and for the periodic analysis of blood gases and pH. A midline neck incision was performed, and the right common carotid artery was exposed to perform coagulation of the proximal branches of the external carotid artery. Rats were placed prone in a stereotaxic frame, and a laser-Doppler flowmetry probe was positioned onto the right parietal bone—previously thinned with a saline-cooled dental drill (coordinates 1.7 mm posterior, 5.5 mm lateral from the bregma)—to assess successful induction of brain ischemia into the middle cerebral artery territory by monitoring cerebral blood flow continuously. Changes in cerebral blood flow were recorded on a computer, over 5-min intervals, and expressed as a percentage from the perfusion values recorded during a 20-min pre-occlusion period. The external carotid artery was incised to allow introduction of a PE-10 catheter. A single clot measuring 35 mm in length was collected in an additional PE-10 tubing that was connected to the PE-10 catheter previously introduced in the external carotid artery. The PE-10 catheter was directed into the internal carotid artery up to 2 mm after the pterygopalatin–internal carotid artery bifurcation, and the clot was injected in a volume of 50 μL saline solution. The interval between the clot collection and injection was less than 5 min. On clot administration, to mimic clinical recommendations (Meyer and Rauch, 2000), rats showing less than 50% reduction or more than 85% reduction in cerebral perfusion (as calculated over a 15-min period before rtPA injection) were strictly excluded from the study design. After a 45-min period of ischemia, the PE-10 catheter was removed from the internal carotid artery to the external carotid artery, and the rats were given rtPA at 0.9 (n = 5) or 10 mg/kg (n = 5) in 1 mL saline solution into the femoral vein (10% bolus plus 90% perfusion over a 45-min additional period) as described above. Sham-treated rats (n = 5) were administered saline solution. Rats were maintained normothermic at 37.5 ± 0.5°C using a feedback-controlled thermostatic heating pad connected to a rectal probe. At the end of the experiment, the PE-10 catheter was removed totally, the external carotid artery stump tied off, and all incisions closed. Then, the rats were awakened and allowed to move freely in their home cage with food and water ad libitum before being used to assess ischemic brain damage.
Ischemic brain damage was assessed as follows. Rats were killed by decapitation under isoflurane anesthesia 24 h after the onset of brain ischemia, which is a time condition that has been clearly demonstrated to allow obtaining consolidated and reliable infarct volume in several comparative studies using magnetic resonance imaging, triphenyltetrazolium chloride, thionin, and neuronal nuclei immunochemical staining techniques (Henninger et al, 2006; Haelewyn et al, 2008). Then, the brain was rapidly removed, frozen in isopentane, and placed at −80°C. Coronal brain sections (20 μm) were cryostat-cut, mounted on slides, stained with thionin, and digitized on a computer. Volumes of brain infarction were analyzed using an image analyzer (ImageJ software, Scion Corp., MD, USA). The lesion areas were delineated by the pallor of staining in the necrotic tissue compared with the surrounding healthy tissue; then, infarction volumes were calculated by integrating the infarct surfaces over the whole brain, corrected for tissue edema and expressed in mm3 of infarction volume.
The experiments were performed in a masked manner (STAIR, 1999). The investigators performing the surgery gave each group of animals a secret code that remained unknown to the experimenters in charge of assessing the effects of 0.9 and 10 mg/kg rtPA on the rat's cerebral reperfusion (see above) and histological outcome until the end of the study. Data are given as mean ± s.e.m. Data were analyzed using the Mann–Whitney non-parametric unpaired U-test. The level of significance was set at P < 0.05.
Results and Discussion
Physiological parameters remained within normal ranges in all groups of rats as monitored all along the experiments (Table 1). On clot injection, cerebral blood flow disruption in the middle cerebral artery territory was similar in all groups of rats and was not significantly different between groups (control rats: 71.7 ± 1.8%; 0.9 mg/kg rtPA-treated rats: 63 ± 4.3%; 10 mg/kg rtPA-treated rats: 64.7 ± 5.6%). Rats showing less than 50% reduction (n = 2) or more than 85% reduction (n = 3) in cerebral perfusion were strictly excluded from the study design because, in line with the clinical review by Meyer and Rauch (2000), these animals respectively showed spontaneous reperfusion before rtPA injection and lack of reperfusion despite rtPA injection. Within this range of reduction in cerebral blood flow, all rats treated with either 0.9 or 10 mg/kg rtPA exhibited cerebral blood flow reperfusion. Cerebral blood flow disruption in sham-treated animals remained stable throughout the 2-h duration of the study and yielded cerebral infarction in the expected territory of the middle cerebral artery. Treatment with either 0.9 or 10 mg/kg rtPA did restore cerebral blood flow perfusion to preischemic baseline values and further led to a significant decrease in infarction volume (391 ± 33 mm3 in sham-treated rats; 165 ± 11 mm3 in those treated with 0.9 mg/kg rtPA, P < 0.005; 95.1 ± 41.9 mm3 in rats treated with 10 mg/kg rtPA, P < 0.005) and brain tissue edema (20.2 ± 3.2% in sham-treated rats; 11.6 ± 0.4% in those treated with 0.9 mg/kg rtPA, P < 0.05; 3.5 ± 2.7% in rats treated with 10 mg/kg rtPA, P < 0.01). Comparison between the effects of 0.9 and 10 mg/kg rtPA on cerebral blood flow reperfusion was as follows. As was expected, rats treated with 0.9 mg/kg rtPA had a smaller cumulated reperfusion flow as compared with rats treated with 10 mg/kg rtPA (85.5 ± 13.2% vs 190.9 ± 24.7%, P < 0.01; Figure 1A and 1B). In addition, rats treated with 0.9 and 10 mg/kg rtPA further exhibited major differences in mean time to reperfusion time of 39.6 ± 3.3 mins and 25.2 ± 3.1 mins (P < 0.05; Figure 1C), but showed similar reperfusion slopes (2.2643 ± 0.389 vs 2.50 ± 0.3415, NS) as calculated from the time reperfusion actually started; Figure 1D). Together, these latter data indicate that differences in reperfusion following injection of 0.9 and 10 mg/kg rtPA mainly result from a slower effect of 0.9 mg/kg rtPA at starting reperfusion rather than from major differences in the kinetics of reperfusion by itself, a delay that could be due to the relatively low sensitivity of the rat's fibrinolytic system to rtPA. All rats treated with 10 mg/kg rtPA, except one, had smaller brain infarction volume (95.1 ± 41.9 vs 165 ± 24 mm3) and tissue edema (3.5 ± 2.7% vs 11.6 ± 0.5%) than rats treated with 0.9 mg/kg rtPA (P < 0.10; Figure 1E).
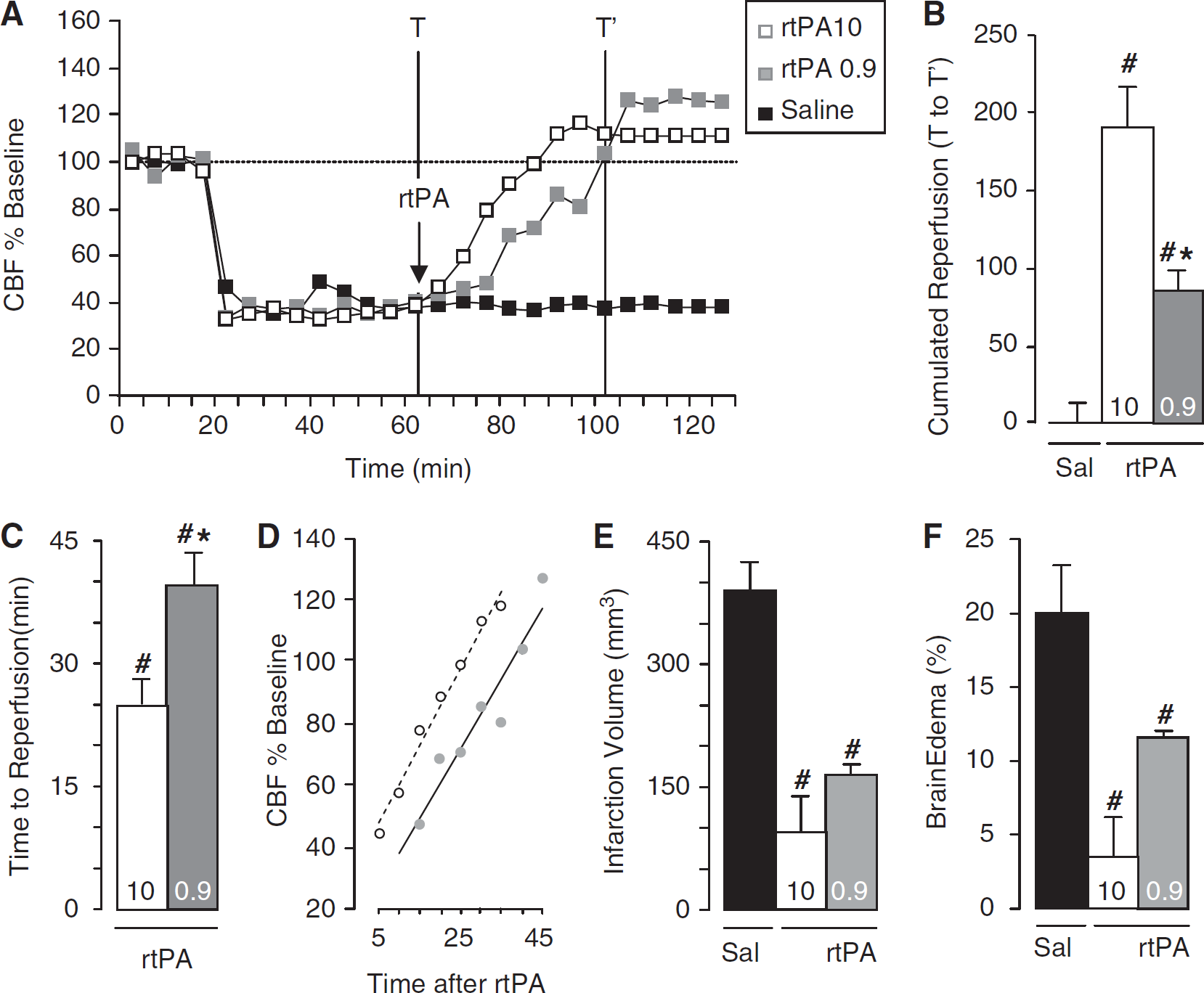
Time course (
Mean Values of arterial PO2, PCO2, SaO2, pH, body temperature, and MAP during the ischemic period in rats treated with rtPA at 0.9 mg/kg and 10 mg/kg
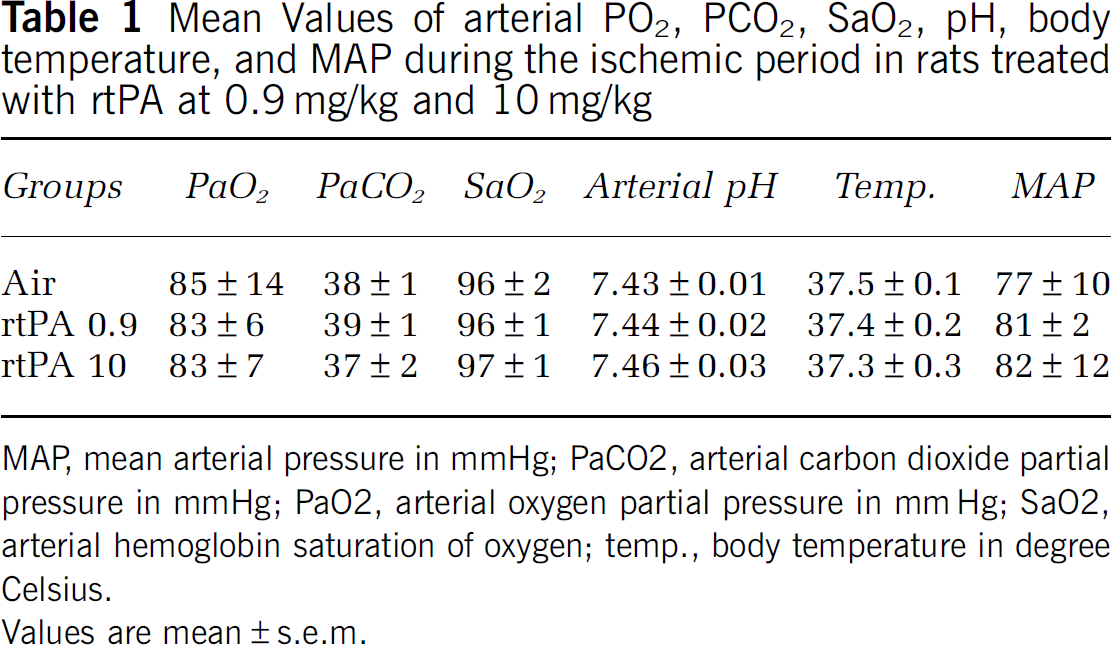
MAP, mean arterial pressure in mmHg; PaCO2, arterial carbon dioxide partial pressure in mmHg; PaO2, arterial oxygen partial pressure in mmHg; SaO2, arterial hemoglobin saturation of oxygen; temp., body temperature in degree Celsius.
Values are mean ± s.e.m.
So far as the dose of 0.9 mg/kg rtPA is concerned, our findings are in line with clinical studies that have shown that the median time to obtain complete recanalization in rtPA-treated patients is in most cases approximately 40 mins (Christou et al, 2000; Delgado-Mederos et al, 2007) or more (Merino et al, 2008). These data, together with the fact that the cumulated reperfusion flow induced by 0.9 mg/kg rtPA was only one-half instead of one-tenth that induced by 10 mg/kg rtPA—as it might be expected from the in vitro studies of Korninger and Collen (1981)—indicate that the dose of 0.9 mg/kg rtPA could be as appropriate as that of 10 mg/kg rtPA for performing preclinical stroke studies in rodents. Particularly, using 0.9 mg/kg rtPA could be of major importance for pharmacological considerations. For instance, in line with previous data that have demonstrated that the noble gas xenon binds within the catalytic site of a series of serine proteases (Schiltz et al, 1995), recent data from our laboratory have shown that xenon, which possesses neuroprotective properties (David et al, 2003, 2008; Homi et al, 2003), also inhibits the catalytic (enzymatic) and thrombolytic activity of rtPA (David et al, 2010). As medical gases such as xenon cannot be used at concentrations above 75 to 80 vol% (as at least 20 vol% oxygen is required to maintain normal body oxygenation), it appears of critical importance to use the clinical dose of 0.9 mg/kg rtPA to avoid the presence of rtPA molecules free of xenon as it would occur if rtPA would be given in excess at 10 mg/kg. Importantly, using the clinical dose of 0.9 mg/kg instead of 10 mg/kg rtPA could also be of major importance to investigate the effects between pharmacological compounds other than gases susceptible of interacting with rtPA or the tPA–plasmin pathway, and to assess reliable clinically relevant evaluations of the beneficial and adverse effects of rtPA, such as neuroprotection vs hemorrhage, in preclinical models.
In conclusion, the present investigation shows that the clinical dose of 0.9 mg/kg rtPA that is currently used in acute ischemic stroke patients can be used confidently and advantageously in preclinical reperfusion stroke studies in rodents, as it provides more clinically relevant time course effects and mean time to reperfusion than the dose of 10 mg/kg rtPA that is used in the majority of stroke studies that are performed in rodents.
Footnotes
Acknowledgements
This research was supported by NNOXe Pharmaceuticals, the French Ministry of Defence, the University of Caen, and the CNRS.
HND and BH are NNOXe Pharmaceuticals scientists. The authors declare no conflict of interest.