
Abstract
Stroke triggers an intense inflammatory response that could be a consequence of Toll-like receptors (TLRs) activation. However, the clinical significance and the therapeutic possibilities of TLR in stroke is not completely clear. In this study, we analyze the association between the expression of TLR2 and TLR4, inflammatory molecules and endogenous ligands, and clinical outcome of ischemic stroke patients, and we test the potential of TLR2/TLR4 and their endogenous ligands as therapeutic targets. For this purpose, we included 110 patients with ischemic stroke finding that TLR2 and TLR4 are independently associated to poor outcome and correlated with higher serum levels of interleukin (IL)1β, IL6, tumor necrosis factor α, and VCAM1, and that TLR4 was independently associated to lesion volume. In addition, we have developed an in vitro model to test the potential therapeutic value of blocking TLR2/TLR4 or their endogenous ligands. Cultured cells (monocytes and human umbilical vein endothelial cells) were treated with serum from ischemic stroke patients, showing a strong inflammatory response that was blocked when TLR2/4 or cellular fibronectin (cFN) or HSP60 were blocked. In conclusion, TLR2 and TLR4 are associated to outcome in stroke patients and TLR2/4 or their endogenous ligands, cFN/HSP60 could be new therapeutic targets for ischemic stroke.
Introduction
Cellular death by necrosis after ischemic stroke activates a very intense inflammatory that has an important role in the outcome of ischemic stroke patients. Such inflammatory response could be a consequence of the activation of Toll-like receptors (TLRs). Toll-like receptors are a family of highly conserved innate immunity receptors that recognize highly preserved structures in pathogens, called pathogen-associated molecular pattern, but they also recognize damage-associated molecular patterns from endogenous molecules, which are released as a consequence of tissue damage. These molecules, also known as endogenous ligands, are able to activate TLRs in the same way that ligands coming from infectious agents do (Kariko et al, 2004). Toll-like receptor activation promotes the recruitment of several adaptive proteins to activate nuclear factor-κB, which induces the expression of proinflammatory genes, inflammatory cytokines, adhesion molecules, and the activation of adaptive immunity (Akira, 2006). Studies performed in TLR4 knockout mice showed smaller infarct sizes and improved neurologic test scores in comparison with the wild type (Cao et al, 2007; Caso et al, 2008), whereas results found for TLR2 knockout mice are controversial (Hua et al, 2009; Lehnardt et al, 2007). Furthermore, it has been observed that TLR4 polymorphisms are associated to ischemic stroke (Lin et al, 2005) and that TLR2 (Urra et al, 2009) and TLR4 (Yang et al, 2008) expression was associated with poor outcome in ischemic stroke patients. According to all described experimental clinical evidence, we tested the hypothesis that ischemic stroke induces the release of some damage-related products and proteins, such as cellular fibronectin (cFN), HSP60, and HSP70, which could work as endogenous ligands for TLR2 and TLR4, promoting the activation of inflammatory response. Furthermore, the analysis of the TLR2 and 4 expressions on peripheral blood cells could be a useful marker for stroke outcome. Finally, we postulate that ligands present in serum from ischemic stroke patients may interact with cells of the immune and/or vascular system, contributing to the increase of inflammatory response; the blockade of ligands and/or TLRs could be an effective strategy to reduce such inflammatory response.
Patients and methods
Study Population and Patients Characteristics
Between February and August 2009, 146 patients with ischemic stroke, with < 12hours of evolution, and previously independents for their daily living activities, were prospectively evaluated to be included in this study. Patients had been admitted to the University Hospital of Santiago de Compostela. Patients with chronic inflammatory diseases (n = 5), severe hepatic (n = 2) or renal (n = 3) diseases, hematological diseases (n = 3), cancer (n = 4), and infectious disease (n = 5) or antiinflammatory treatment (n = 6) in the 15 days before inclusion were excluded. Furthermore, five patients did not accept their participation in the study and three patients were lost during follow-up, ending up with a total of 110 patients (male, 58.2%; mean age, 74.6 ± 9.8 years). Seventeen patients showed fever (temperature > 37.5°C) during hospitalization, but infectious focus was only found in 11 of them. This complication appeared at 52hours in one patient, between days 3 and 7 in three patients, and between days 7 and 9 in 7 patients. We have also included 10 healthy controls (male 60%; mean age 73.4 ± 15.7 years) with the same exclusion criteria.
The experimental protocol was approved by the ethics committee from the Universitary Clinical Hospital of Santiago de Compostela. Furthermore, informed consent was given by patients or their relatives.
Clinical Variables
All patients were admitted in the acute stroke unit and treated by the same stroke team according to the Guidelines of the Cerebrovascular Diseases Study Group of the Spanish Society of Neurology (Comité ad hoc del Grupo de Estudio de Enfermedades Cerebrovasculares de la SEN. Guía para el diagnóstico y tratamiento del ictus. Prous Science, 2004). Medical history accounting for potential vascular risk factors was recorded, and blood and coagulation tests, 12-lead electrocardiography, chest radiography, and carotid ultrasonography were performed at admission. Stroke onset was considered the time from the onset of symptoms (or the last time that patient was seen asymptomatic, when stroke was noticed at awakening), to the moment that the patient was included in the study. Stroke subtype was classified according to Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification (Adams et al, 1993). To evaluate neurologic deficit, the National Institutes of Health Stroke Scale (NIHSS) was performed on admission, at 24hours, 72hours, 7 days, and 3 months. Modified Rankin Scale (mRS) was determined at 3 months on a routine visit of patients to the hospital. Rankin score of 0 and 1 indicates patients with independence for their daily activities; 3, 4, and 5 indicates patients with dependence for the daily activities; and a score of 6 identifies death patients. NIHSS and mRS were evaluated by internationally certified neurologists.
Neuroimaging Studies
Computed tomography (CT) scans were performed on admission and between days 4 and 7 of hospitalization. Early CT signs of infarction were evaluated on admission, and infarct volume was assessed at the second CT scan. Infarct volume was calculated on the CT image by using the formula 0.5 × a × b × c (where a and b are the two major perpendicular axes of an oval that covers the lesion, and c is the number of 10 mm slices containing infarct) (Sims et al, 2009).
All CT scans were evaluated by neuroradiologists blinded to clinical and biochemical data.
Clinical Outcome Variables
The primary end point was defined as good functional outcome (mRS ≤ 2) at 3 months. Infarct volume and association between TLR expression and inflammatory response were considered as secondary variables.
Toll-Like Receptors 2 and 4 Expression Analysis
Toll-like receptors 2 and 4 expression analyses were performed by flow cytometry in blood samples collected in EDTA-anticoagulated tubes withdrawn from patients on admission and at 24 hours, 72 hours, and 7 days and from healthy controls subjects in only one extraction.
For the expression analysis of TLR2 and TLR4, monocytes, lymphocytes, and neutrophils were separated by their forward and side scattering signal characteristics on flow cytometry. APC-TLR2 antibody (BD Biosciences, NJ, USA) and biotin-TLR4 antibody (BD Biosciences) together with streptavidin-PE (BD Biosciences) were used to quantify TLR expression. Samples were analyzed on a FACSAria flow cytometer (BD Biosciences). Mean expression of TLR2 and TLR4 on monocytes was analyzed.
In Vitro Experiments With Monocytes and Human Umbilical Vein Endothelial Cells
Monocytes were isolated by fluorescent-assisted cell sorting, using CD14-FITC antibody (BD Biosciences) as specific monocyte marker. Cells were incubated for 24 hours at 37°C, 97% humidity and 5% CO2 in RPMI1640 medium, supplemented with 10% calf fetal serum, 2mmol/L glutamine, and 100U/mL penicillin (all from Invitrogen). Human umbilical vein endothelial cells (HUVECs) were acquired from PromoCell (PromoCell, Heidelberg, Germany) and cultured according to the manufacturer's instructions.
Monocytes and HUVECs were cultured with their corresponding medium and with or without a mix of culture medium and serum from ischemic stroke patients (dilution 3:1). Used serum was a pool from all patients included in the study. As a control, we used a mixture of culture medium and a pool of serum from the healthy control subjects (dilution 1:3). Treatments were performed during 18 hours at 37°C, 97% humidity, and 5% CO2. The supernatant was collected for further analysis of inflammatory molecules. For TLR2 and TLR4 blocking experiments, TLR2 and/or TLR4 neutralizing antibodies (concentration 10mg/mL; Abcam, Cambridge, UK) were added to cultured cells during 1 hour prior serum treatment. To block endogenous ligands, serum was incubated during 1 hour at 37°C with antibodies anti-HSP60 (dilution 1:80; Stressgen, San Diego, CA, USA), anti-HSP70 (dilution 1:80; Stressgen), anti-cFN (dilution 1:20; Sigma-Aldrich, St Louis, MO, USA), and the mix of the three antibodies, previously adding serum to cultured cells. Finally, supernatants from monocytes were used to analyze interleukin 6 (IL6) and tumor necrosis factor α (TNFα) and supernatants from HUVECs were used to analyze IL6, von Willebrand Factor (vWF), and E-selectin.
Molecular Variables Analysis
Blood samples, withdrawn from patients on admission and at 24 hours, 72 hours, and 7 days were collected in chemistry test tubes, centrifuged at 3,000 g for 15 minutes, and immediately frozen and stored at −80°C.
Serum levels of cFN (BioHit, Helsinki, Finland), HSP60 and HSP70 (Assay Designs, Ann Arbor, MI, USA), Intercellular Cell Adhesion Molecule 1 (ICAM1) (Bender Medsystem, Viena, Austria), Vascular Cell Adhesion Molecule 1 (VCAM1) (R&D, Minneapolis, MN, USA), matrix metalloproteinases 9 (R&D), vWF (American Diagnostica, Stamford, CT, USA), and E-selectin (R&D) were measured by using ELISA kits, and IL6, TNFα, and IL1β were evaluated by an immunodiagnostic robot IMMULITE 1000 System (Diagnostic Products Corporation, CA, USA), following the manufacturer's instructions.
Statistical Analysis
Results are expressed as percentage, for categorical variables, and as mean (s.d.) or median (quartiles) for continuous variables, depending on whether they were normally distributed or not. Proportions were compared using the χ2 test. To compare continuous variables between groups, a Student's t-test was used for variables normally distributed and a Mann-Whitney test for not normally distributed variables. Spearman or Pearson analysis was used for bivariate correlations.
The influence of TLRs on functional outcome was assessed by logistic regression analysis, and the influence of TLRs on lesion volumes was assessed by multiple lineal regression analysis. Regression analyses were performed after adjusting for the main baseline variables, related to outcome or lesion volume, in the univariate analyses (enter approach and probability of entry P < 0.05). Results were expressed as adjusted odds ratios (ORs) with the corresponding 95% confidence intervals (95% CIs). The statistical analysis was performed using SPSS software v16.0.
Results
Clinical Study
Primary outcome: relationship between Toll-like receptor expression and outcome: Table 1 shows the main characteristics of patients grouped by functional outcome. Sixty-two patients (56.4%) showed poor functional outcome (defined as mRS > 2) at 3 months. Atrial fibrillation was significantly more frequent in patients with poor functional outcome who also showed higher glucose and C Reactive Protein (CRP) levels, as well as more neurologic deficit on admission and larger lesion volumes between days 4 and 7.
Baseline clinical characteristics, vascular risk factors, stroke subtype, biochemical parameters, and neuroimaging findings in patients with good and poor outcome
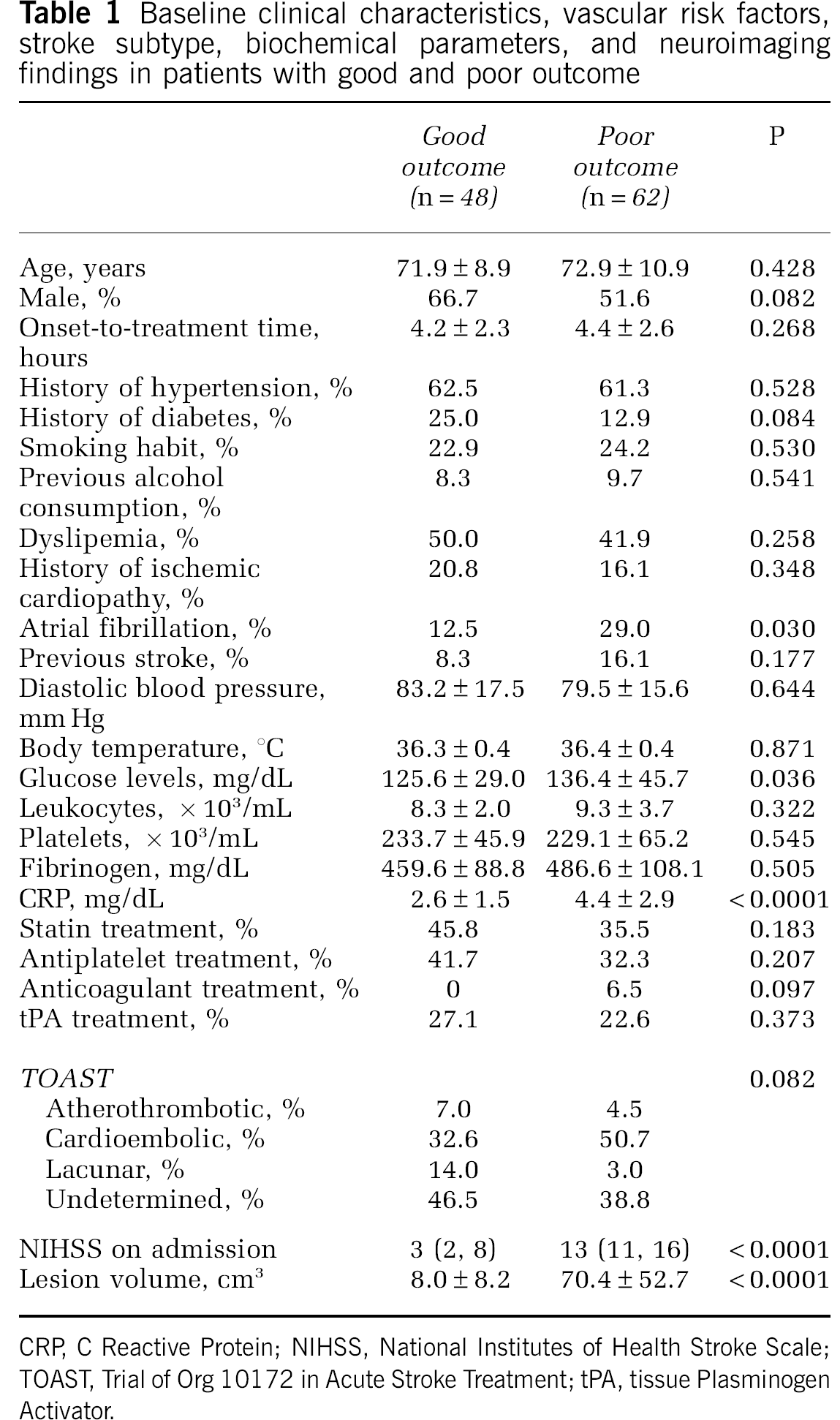
CRP, C Reactive Protein; NIHSS, National Institutes of Health Stroke Scale; TOAST, Trial of Org 10172 in Acute Stroke Treatment; tPA, tissue Plasminogen Activator.
Toll-like receptor expression in the different score groups of mRS is shown in Figure 1 and TLR expression at different time points by functional outcome is shown in Table 2. No differences were found in TLR2 and TLR4 expression on admission between patients with good and poor outcome. However, TLR2 and TLR4 expression at 24 hours, 72 hours, and day 7 was significantly higher in patients with poor outcome (Table 2).
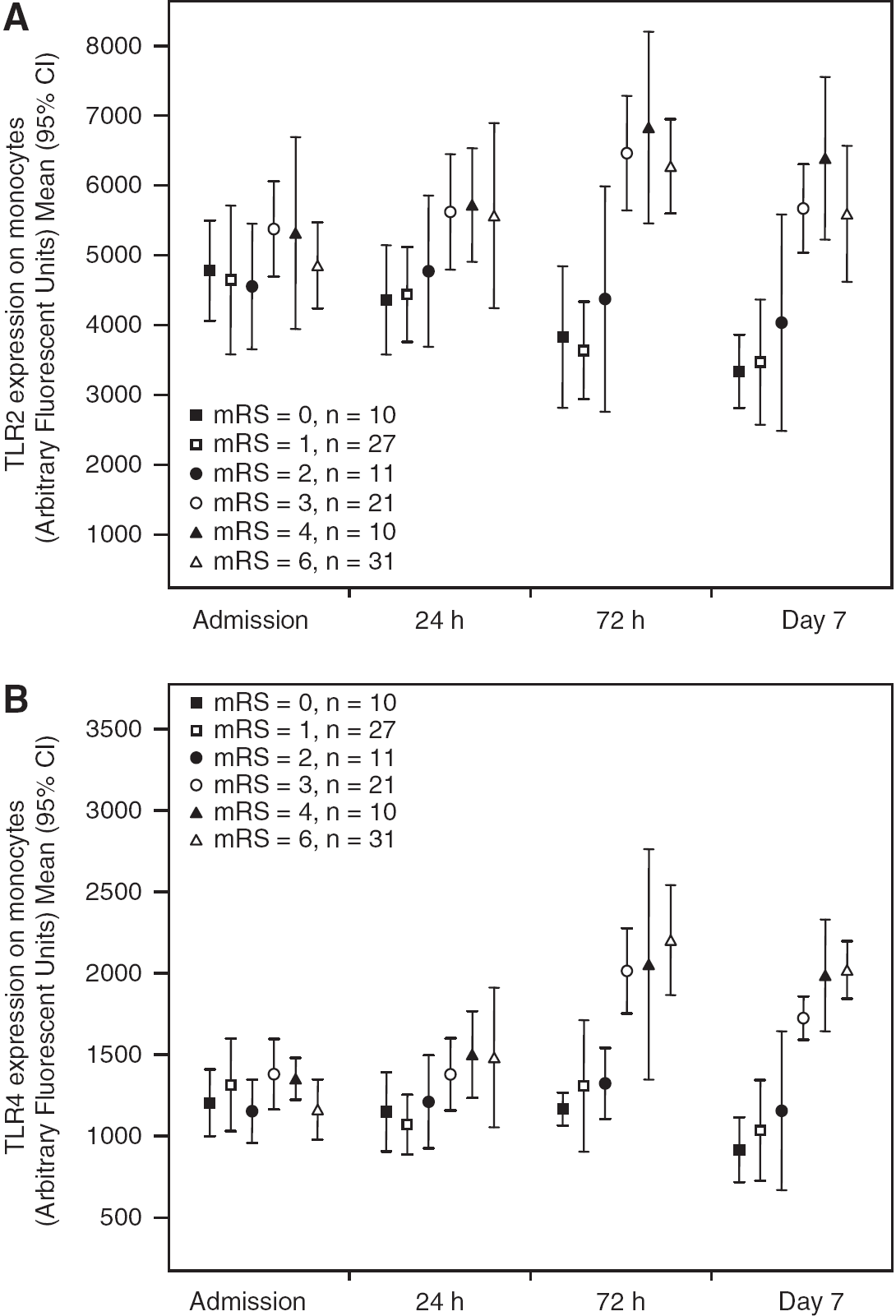
TLR2 (
Comparative analysis of TLR2 and TLR4 mean expressions on monocytes between patients with good and poor outcome and TLR2 and TLR4 mean expression on monocytes of healthy control subjects
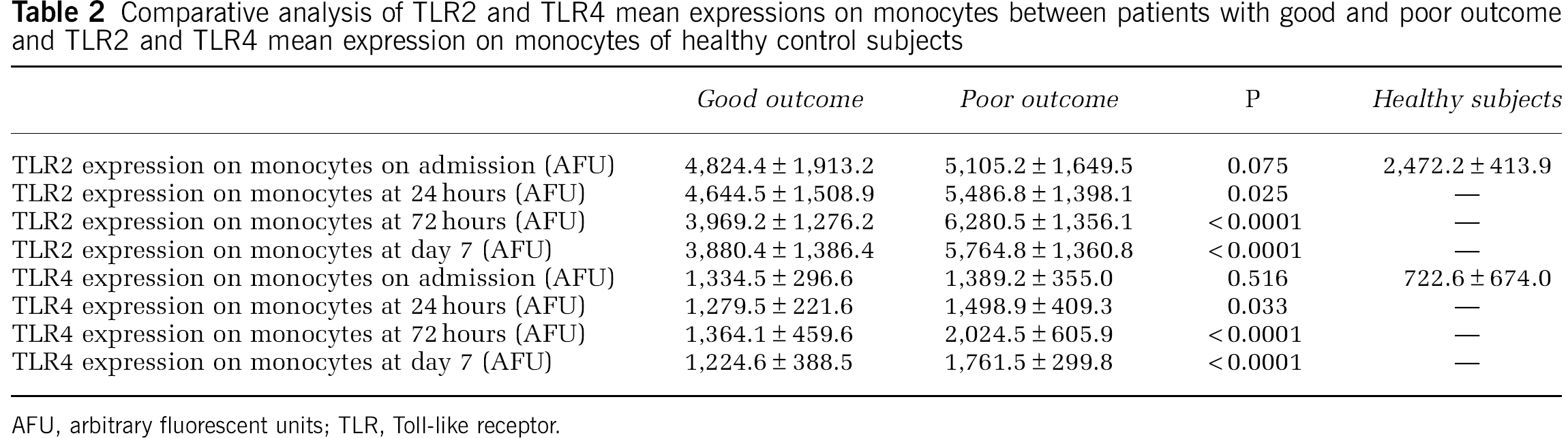
AFU, arbitrary fluorescent units; TLR, Toll-like receptor.
In the logistic regression analysis, TLR2 expression at 24hours (OR, 2.9; 95% CI, 1.6 to 5.3), 72hours (OR, 8.7; 95% CI, 3.0 to 25.6), and 7 days (OR, 13.9; 95% CI, 2.8 to 69.0), and TLR4 expression at 24hours (OR, 21.0; 95% CI, 2.5 to 137.9), 72hours (OR, 63.2; 95% CI, 1.0 to 718.2), and 7 days (OR, 408.0; 95% CI, 16.6 to 1,046.5) were independently associated with poor outcome after adjustment for atrial fibrillation, glucose and CRP levels, baseline stroke severity, and infarct volume.
Secondary outcome: relationship between Toll-like receptor expression and infarct volume: Infarct volume was associated with history of diabetes (r = 0.227, P = 0.023), history of atrial fibrillation (r = 0.208, P = 0.038), CRP levels on admission (r = 0.393, P < 0.0001), and NIHSS on admission (r = 0.560, P < 0.0001).
In the multivariate analysis, TLR4 expression at 72 hours (B, 41.9; 95% CI, 28.1 to 55.6) and at day 7 (B, 45.0; 95% CI, 25.5 to 64.6) was independently associated with infarct volume after adjustment by history of diabetes and atrial fibrillation, CRP levels, and baseline stroke severity.
Relationship between the expression of Toll-like receptors 2 and 4 and levels of endogenous ligands cellular fibronectin, HSP60, and HSP70: Cellular fibronectin levels on admission were positively correlated with the mean expression of TLR2 on monocytes at 24 hours, 72hours, and 7 days, but not on admission. In the multivariate analysis, only the mean expression of TLR2 on monocytes at 24hours was independently associated with cFN levels on admission (OR, 3.8; 95% CI, 1.2 to 11.6). On the other hand, no correlation was found between cFN levels on admission and the mean expression of TLR4 on monocytes.
No significant correlations were found between HSP60 levels on admission and TLR2 and TLR4 expression on admission, 24hours, 72hours, or 7 days.
HSP70 levels on admission were positively correlated with the mean expression of TLR2 on monocytes at 24hours, 72hours, and 7 days. However, none of such correlations kept their independence when adjusted models were applied in the multivariate analysis. Likewise, HSP70 levels were also associated with TLR4 expression on monocytes at 72hours and at 7 days, but their independence was lost when adjusted models were applied in the multivariate analysis.
Relationship between the expression of Toll-like receptors 2 and 4 and the levels of inflammatory markers: Toll-like receptors 2 and 4 expression at baseline is correlated with IL1β, TNFα, IL6, and VCAM1 levels at 24 hours, 72hours, and 7 days, but not on admission. Furthermore, correlations were found between TLR4 at baseline and ICAM1 at the same time points. However, no correlation was observed between TLRs and matrix metalloproteinases 9 (Figure 2).
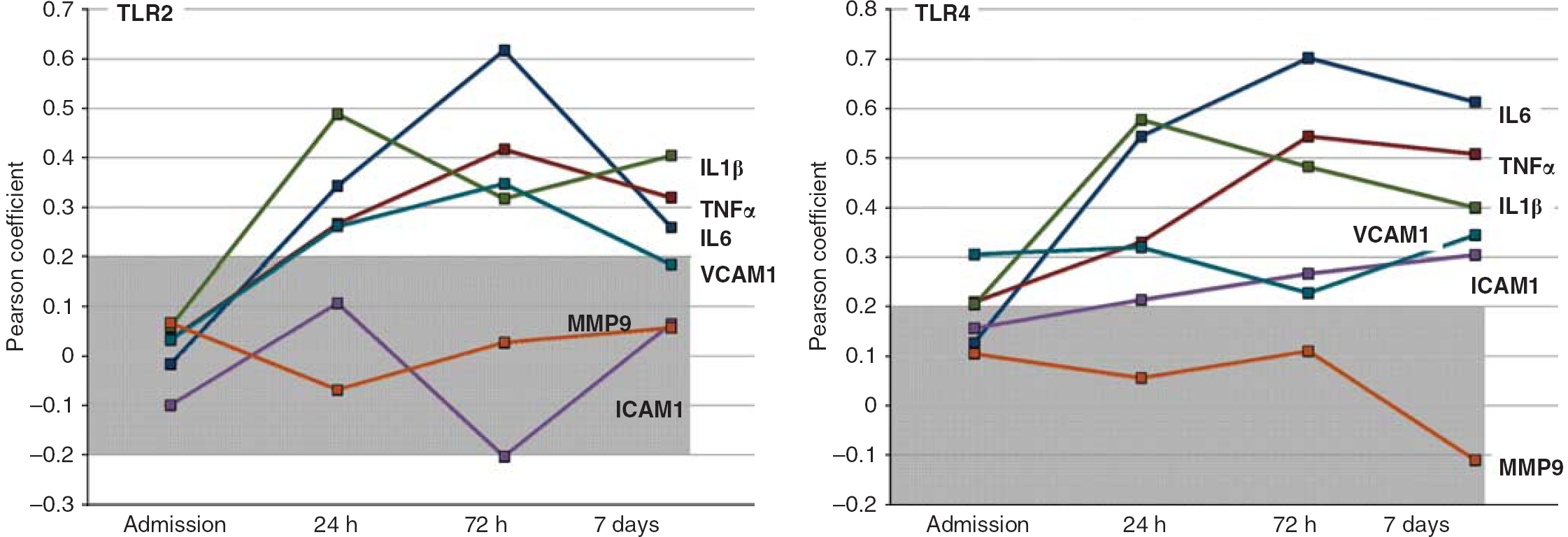
Graphic representations of Pearson coefficients between the expression of TLR2 and 4 on admission (n = 110 patients), and levels of inflammatory (interleukin (IL)1 β, tumor necrosis factor α (TNFα), IL6, and matrix metalloproteinases 9 (MMP9)) and adhesion molecules (VCAM1 and ICAM1) at baseline, 24 hours, 72 hours, and 7 days. Gray-shadowed points represent coefficients that were not statistically significant. Hollowed points represent statistically significant coefficients. ICAM1, Intercellular Cell Adhesion Molecule 1; TLR, Toll-like receptor; VCAM1, Vascular Cell Adhesion Molecule 1.
In Vitro Study
Serum obtained from patients with ischemic stroke on admission was added to cultured monocytes and HUVECs, using regular medium and serum from healthy subjects as negative control. All analyzed inflammatory markers showed higher expression in the supernatants of cells treated with serum from ischemic stroke patients (P < 0.0001) (Figure 3A). When cells were treated with antibodies against TLR2, TLR4, cFN, HSP60, or HSP70 without human serum, no significant effect was observed in the inflammatory markers analyzed. When cells were pretreated with neutralizing antibodies anti-TLR2 and/or TLR4, inflammatory marker levels were significantly lower (Figure 3C). Furthermore, when serum was pretreated with antibodies against potential endogenous ligands, such as cFN and HSP60, levels of inflammatory markers were significantly decreased (Figure 3D). However, HSP70 blockade did not show any effect in the reduction of inflammatory response.
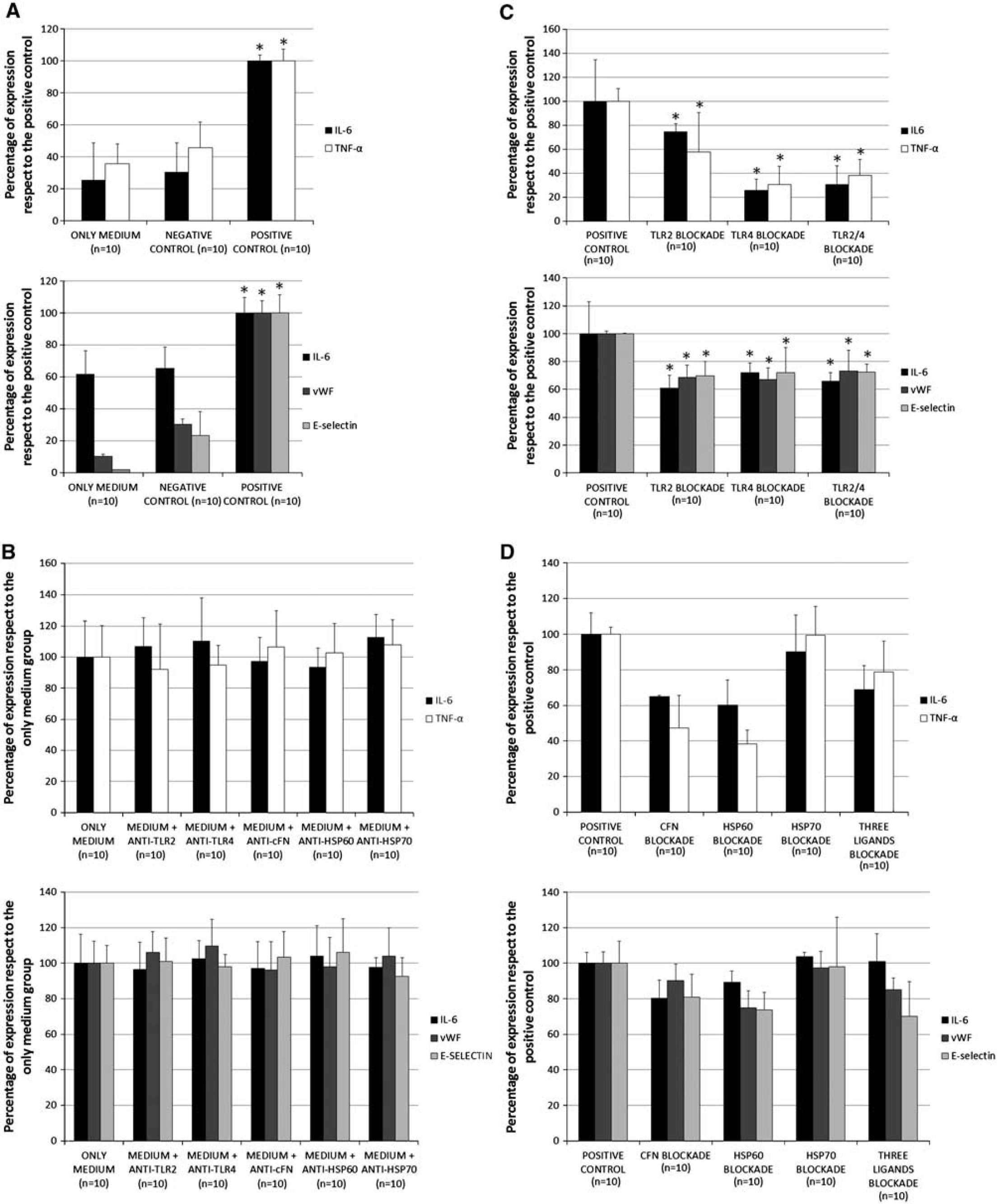
Graphical representation of levels of inflammatory markers in the supernatant of monocytes (left graphic) and human umbilical vein endothelial cells (HUVECs) (right graphic) cultured during 18 hours. (
Discussion
This is, to the best of our knowledge, the first prospective study that has evaluated the role of TLR2 and 4, together with their potential endogenous ligands (cFN, HSP60, and HSP70) and the inflammatory molecules that are expressed as a consequence of their activation in acute ischemic stroke. Remarkably, higher expression of TLR2 and TLR4 was associated with poor functional outcome in ischemic stroke patients. These results are in line with those obtained by Urra et al (2009) and Yang et al (2008), who found that TLR4 expression is independently associated with functional outcome and stroke severity, respectively. In our study, we additionally found that TLR4 expression is associated with infarct volume too. On the other hand, we have analyzed the role of cFN, HSP60, and HSP70 as potential endogenous ligands for TLR2 and 4. In this regard, we found an independent association between cFN levels on admission and TLR2 expression on monocytes at 24hours. In addition, the correlation between TLR2 and 4 expression and the levels of inflammatory and cell adhesion molecules at different time points during acute phase of stroke was analyzed. Toll-like receptors 2 and 4 expression on admission was found to be correlated with IL1β, IL6, TNFα, and VCAM1 levels at 24 hours, 72hours, and 7 days. Furthermore, TLR4 is also associated to ICAM1. The fact that we have found an association between TLRs on admission and inflammatory molecules at 24 hours, 72hours, and 7 days, but not on admission, seems to indicate that TLR2 and 4 could be involved in the activation of the inflammatory response during the acute phase of ischemic stroke. Finally, we have also conducted an in vitro study to investigate the role of molecules present in serum of ischemic stroke patients, such as cFN, HSP60, and HSP70 on the activation of TLR2 and 4. Additionally, we have tested whether the blockade of TLRs or endogenous ligands could be a therapeutic antiinflammatory approach for cerebral ischemia. We have demonstrated that serum from patients with ischemic stroke induces a powerful inflammatory response in cultured cells such as monocytes and endothelial cells. We analyzed several inflammatory markers that have been previously reported as markers for the activation of endothelial cells and monocytes (Damas et al, 2006; Fischer et al, 2009; Kamgang et al, 2008; Kikkert et al, 2008). As mentioned previously, treatment of cultured cells with serum from ischemic stroke patients induced an increase on the expression of inflammatory markers that was reduced when cells were pretreated with neutralizing antibodies against TLR2 and/or TLR4. Furthermore, when serum from patients was treated with antibodies against HSP60 or cFN before being added to cultures of monocytes and HUVECs, similar reduction in inflammatory markers was observed. However, when serum was treated with antibodies against HSP70, such reduction on inflammation was not observed. These results suggest that HSP60 and cFN, but not HSP70, present in the serum from ischemic patients, could act as endogenous ligands for TLR2 and/or TLR4 activation. Together with the results from the clinical study, we have to highlight that correlations between cFN and TLR expression were found, and cFN showed its potential as endogenous ligand in the in vitro study. However, no positive correlation between HSP60 and TLRs was found in the clinical study although it shows its potential as endogenous ligand in the in vitro study. This fact indicates that cFN and HSP60 activate TLR-dependent inflammatory response. However, only cFN influences the expression of TLRs. We do not know if this effect is mediated by the engagement of cFN to the TLR or by other receptors.
Analyzing our in vitro results, we could postulate that serum from ischemic stroke patients contains endogenous ligands, which facilitate the activation of TLR pathways. This activation occurs in peripheral tissues, as we have tested cells from the immune (monocytes) and the vascular systems (HUVECs)), contributing to increase the inflammatory response and contributing to the outcome of patients. Contribution of peripheral inflammation in outcome of patients is justified by the fact that peripheral inflammatory response precedes brain inflammation after experimental stroke (Chapman et al, 2009) and that leukocytes are activated in the peripheral immune compartment, before they access to the brain (Offner et al, 2006). We reasoned that stroke induces the activation of peripheral inflammatory response, activating TLRs on peripheral leukocytes, before their entry to the brain, and that these activated leukocytes influence stroke outcome directly. In this way, peripheral inflammatory activation can influence stroke outcome.
The role of cFN and HSP60 as potential endogenous ligands of TLRs (Lasarte et al, 2007) and its relationship to other diseases has been previously described (Goos et al, 2007; Methe et al, 2005). However, these studies were conducted using recombinant proteins (Lasarte et al, 2007) or selected serum (Yang et al, 2008), instead of a pool of serum from ischemic stroke patients. Besides, they have used transformed cells instead of cells from human origin.
In our study, there was a baseline difference in the stroke severity (NIHSS) between the poor-outcome [13(11,16)] versus the good-outcome group [3(2,8)]. This finding is not surprising and it is in agreement with previous studies that have found association between NIHSS and outcome of patients at 3 months (Adams et al, 1999). As NIHSS is strongly correlated with outcome, we included it in the logistic analysis and such differences did not hamper the finding of TLR2 and TLR4 as prognostic factors.
We are aware that this study presents some limitations. In the first place, the size of the sample is limited. Second, patients were excluded when they showed any infection within 15 days before admission, while they were not excluded if infections developed during the acute phase. This fact may have some impact in the final results; however, only four patients showed infection during the time that samples were acquired. For this reason, we consider that infections do not influence our results; nevertheless, it is not possible to completely rule out that the presence of subclinical infections could be influencing our results.
In conclusion, TLR2 and TLR4 expression is associated with poor outcome and higher inflammatory response in acute ischemic stroke. Besides, TLRs and/or endogenous ligands, such as cFN or HSP60, could be therapeutic antiinflammatory targets.
Footnotes
The authors declare no conflict of interest.