
Abstract
The naturally occurring antagonist of interleukin-1, IL-1RA, is highly neuroprotective experimentally, shows few adverse effects, and inhibits the systemic acute phase response to stroke. A single regime pilot study showed slow penetration into cerebrospinal fluid (CSF) at experimentally therapeutic concentrations. Twenty-five patients with subarachnoid hemorrhage (SAH) and external ventricular drains were sequentially allocated to five administration regimes, using intravenous bolus doses of 100 to 500 mg and 4 hours intravenous infusions of IL-1RA ranging from 1 to 10 mg per kg per hour. Choice of regimes and timing of plasma and CSF sampling was informed by pharmacometric analysis of pilot study data. Data were analyzed using nonlinear mixed effects modeling. Plasma and CSF concentrations of IL-1RA in all regimes were within the predicted intervals. A 500-mg bolus followed by an intravenous infusion of IL-1RA at 10 mg per kg per hour achieved experimentally therapeutic CSF concentrations of IL-1RA within 45 minutes. Experimentally, neuroprotective CSF concentrations in patients with SAH can be safely achieved within a therapeutic time window. Pharmacokinetic analysis suggests that IL-1RA transport across the blood–CSF barrier in SAH is passive. Identification of the practicality of this delivery regime allows further studies of efficacy of IL-1RA in acute cerebrovascular disease.
Keywords
Introduction
Cerebral ischemia in stroke and subarachnoid hemorrhage (SAH) is a major cause of death and disability (Rabinstein et al, 2004). Although there have been in excess of 110 trials of potentially neuroprotective drugs (O'Collins et al, 2006), few have shown promising results and only one, recombinant tissue plasminogen activator, is currently licensed for administration. The use of recombinant tissue plasminogen activator is limited to within 4.5 hours of stroke after the onset of symptoms and requires that the criteria for patients with ischemic stroke who could be treated with recombinant tissue plasminogen activator are fully satisfied (Adams et al, 2007). Although the proportion of patients arriving to hospital with 4.5 hours of stroke onset is ~30% (Deng et al, 2006), recombinant tissue plasminogen activator is administered to only 6% to 25% for a variety of reasons (Huang et al, 2006b). Apart from the use of calcium channel blocker nimodipine in SAH (Dorhout Mees et al, 2007), no pharmacological agent has been proven to improve outcome in hemorrhagic stroke, intracerebral hemorrhage, or SAH. Moreover, side effects resulting from administration of nimodipine occasionally limit its use (Topcuoglu and Singhal, 2006).
There is an increasing body of evidence to suggest that inflammation has an important function in the pathological events arising as a consequence of cerebral ischemia (Huang et al, 2006a) and that the proinflammatory cytokine interleukin-1 (IL-1) is particularly implicated as an important mediator (Boutin et al, 2001; Buttini et al, 1994; Hara et al, 1997; Yamasaki et al, 1995). The IL-1RA is the naturally occurring antagonist of IL-1 and is the most widely studied putative neuroprotective agent in acute cerebrovascular disease (Banwell et al, 2009). It is a potent inhibitor of experimentally induced ischemic brain damage when given intracerebroventricularly (Loddick and Rothwell, 1996), intraperitoneally (Ohtsuki et al, 1996), intravenously (Clark et al, 2008), and subcutaneously (Relton et al, 1996) up to 3 hours after induction of ischemia (Mulcahy et al, 2003). A recombinant formulation of IL-1RA, anakinra (Kineret) (Amgen Inc, Thousand Oaks, CA, USA) is manufactured and licensed as a secondary-line treatment for rheumatoid arthritis. Clinically, it is effective in reducing peripheral markers of inflammation in stroke (Emsley et al, 2005) and has been shown to have a good safety and tolerability profile in SAH (Clark et al, 2008), stroke (Emsley et al, 2005), and other diseases such as rheumatoid arthritis (Nuki et al, 2002) and diabetes mellitus (Larsen et al, 2007). In SAH, IL-1 potentially contributes to the development of cerebral ischemia through various mechanisms. It may cause vasospasm by the upregulation of potent vasoconstrictors such as endothelin and induction of IL-6 that has been shown to induce vasospasm in experimental studies. The IL-1 contributes to blood–brain barrier (BBB) dysfunction, worsens cerebral edema, and leads to increased intracranial pressure (Blamire et al, 2000). It may enhance cytotoxicity caused by NMDA-mediated cortical spreading depression, another potential cause of delayed cerebral ischemia after SAH (Obrenovitch and Zilkha, 1996). The IL-1 may also be a primary driver of a systemic acute phase response, including an increase in plasma IL-6 (McMahon et al, 2010). Finally, it acts as an endothelial activator and is induced during the coagulation cascade triggered by tissue injury (Cicala and Cirino, 1998).
Studying the pharmacokinetics of IL-1RA is pivotal to the process of development of the drug as a potential neuroprotective agent, is a prerequisite for pharmacodynamic studies and one of the main Stroke Therapy Academic Industry Roundtable (STAIR) criteria drafted in effort to maximize the potential success of any potential stroke treatment (STAIR, 2001). Investigating the pharmacokinetics of IL-1RA within the central nervous system is technically challenging in stroke given the lack of access to both CSF and intraparenchymal tissue. The SAH patients who undergo insertion of an external ventricular drain (EVD) to control intracranial pressure provide ready access to CSF and therefore present an ideal cohort in which to investigate IL-1RA pharmacokinetics across the BBB. The BBB integrity influences the transfer of IL-1RA across the BBB and there is inter- and intracondition heterogeneity in the extent of BBB disruption. Radiological evidence of BBB disruption is present in stroke patients, cerebral small vessel disease, and lacunar stroke (Topakian et al, 2010). In poor-grade SAH, contrast-enhanced computed tomography and isotope brain scintigraphy studies have also shown that there is widespread BBB dysfunction (Doczi, 1985). Moreover, in SAH patients who experience overt delayed cerebral ischemia (DCI) leading to cerebral infarction, the extent of BBB dysfunction within the infarct would be expected to be similar to that in primary acute stroke affecting the same vascular distribution.
In preclinical studies, a cerebrospinal fluid (CSF) concentration of 100 ng/mL of IL-1RA within 1 hour of transient middle cerebral artery ischemia was observed to correspond to its neuroprotective effect (Clark et al, 2008). A pilot study in SAH patients showed that intravenous IL-1RA given as a bolus of 100 mg followed by an infusion of 2 mg per kg per hour was safe and penetrated the BBB to achieve this experimentally therapeutic concentration within 3 hours of commencement of infusion (Clark et al, 2008). Given that an average of 1.9 million neurones are destroyed per minute (Saver, 2006), and the delay from onset of symptoms to commencement of drug administration (Lacy et al, 2001), it is essential that therapeutic concentrations are achieved within the shortest time possible. We therefore set out to identify a safe, tolerable, practical administration regime that could achieve experimentally therapeutic CSF concentrations of IL-1RA within a reasonable time window.
Materials and methods
The study protocol was submitted and approved by Amgen Inc who provided the drug, anakinra, free of charge. Medicine and Healthcare Products Regulatory Agency and National Research Ethics Committee approvals were obtained before the study commenced.
Patient Recruitment
Eighty-eight patients were screened and 30 were recruited from the Intensive Care and High Dependency units at Salford Royal NHS Foundation Trust, UK and Cambridge University Hospitals NHS Foundation Trust, UK between December 2007 and December 2008 (Figure 1). Patients were Caucasian, aged 37 to 76 years (mean age = 53 years), with a mean weight of 73 kg (range, 58 to 110 kg). Patients eligible for the study had radiologically confirmed SAH and an external ventricular drain inserted to manage ensuing hydrocephalus. Exclusion criteria for study entry included a clinically significant concurrent medical condition, participation in another study in the last 30 days or concurrent immunosuppressant medication. Pregnant or breast-feeding patients, those with a history of sensitivity to products derived from
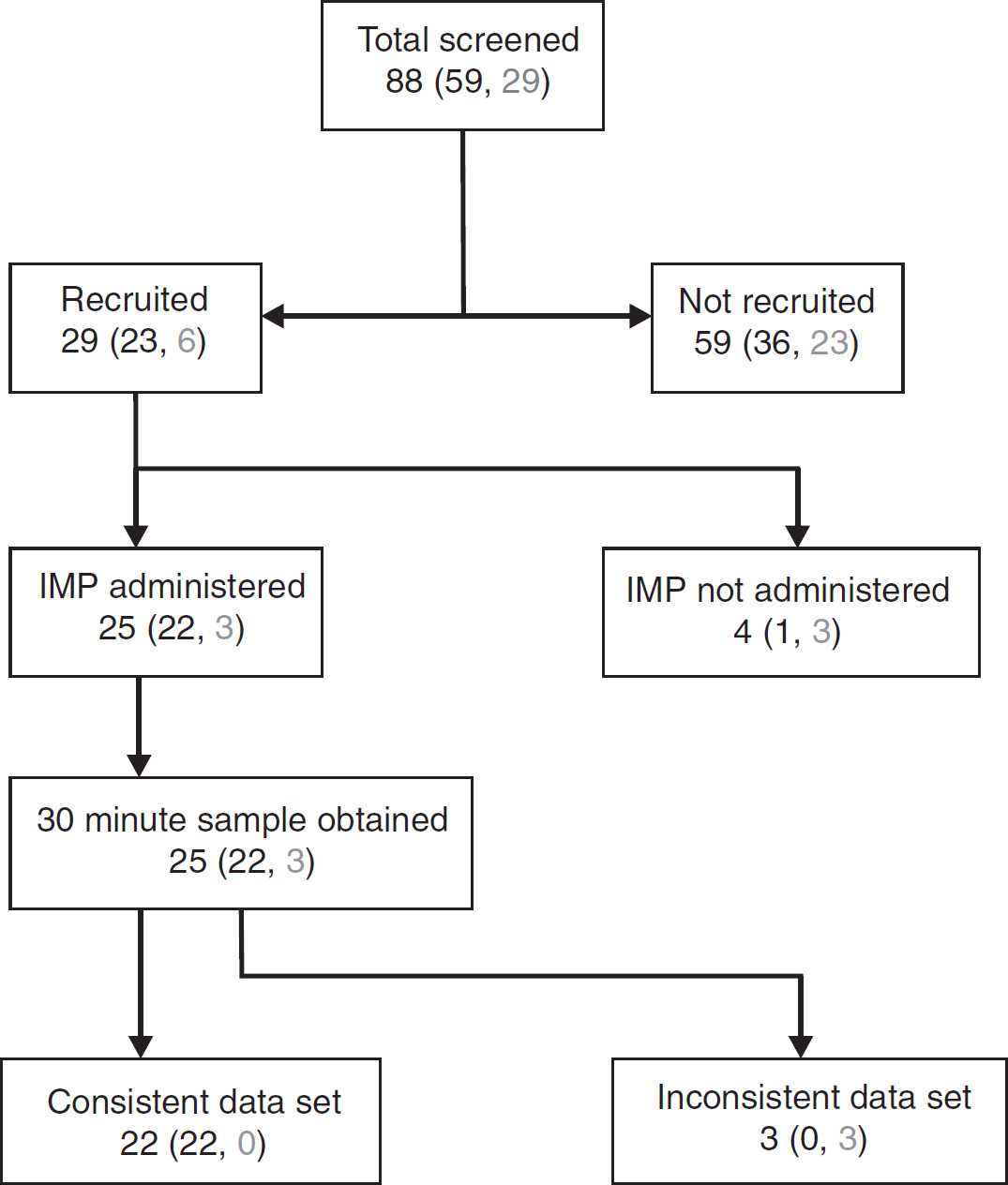
Screening and recruitment schema (black = SRFT, gray = Cambridge). IMF, investigational medicinal product.
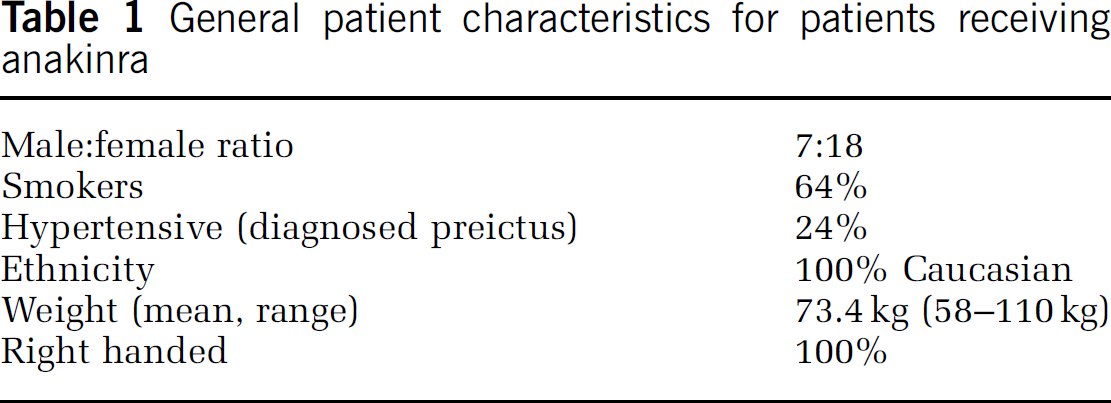
Written consent was obtained from the next of kin for all patients as none were deemed fit to consent at the time of recruitment. Two patients improved cognitively during the course of the study and were subsequently approached for consent. Four patients recruited into the study did not receive the investigational medicinal product for various reasons including accidental removal of the EVD and death. Of the 25 patients receiving the drug, 22 were recruited from Salford and 3 from Cambridge. General patient characteristics are shown in Table 1.
General patient characteristics for patients receiving anakinra
Clinical history and demographic data were collected and a physical examination was performed on each patient. At presentation, 17 patients were poor grade (World Federation of Neurosurgeons Score IV and V) and 8 were good grade (World Federation of Neurosurgeons Score I–III). The distribution of blood on computed tomography scan varied but all had diffuse clots of blood (Fisher grade III) or intraventricular blood (Fisher grade IV). Of the 25 patients receiving the investigational medicinal product, 20 had solitary aneurysms and 5 had multiple aneurysms. In all, 76% of the aneurysms were located within the anterior circulation and the majority (21) were coiled.
Pharmacokinetics
An empirical pharmacokinetic (PK) model for intravenous anakinra has already been published by our research group (Gueorguieva et al, 2008), with population pharmacokinetics (PPK) fitting a linear two-compartment model for plasma with elimination from the central compartment and a one-compartment model for CSF. Before using this model to inform the design of our dose-ranging study, the raw data for the model-making study were reviewed and the parameter estimates for the published model were refined using the NONMEM computer program, version VI (ICON Development Solutions, Dublin, Ireland).
Using revised parameter estimates, simulation of different permutations of intravenous boluses (ranging from 100 to 1000 mg in 100 mg steps) and infusions (ranging from 1 to 10 mg per kg per hour for 4 hours in 1 mg per kg per hour steps) of anakinra were performed. Simulations were performed using a custom script in GNU-R. The administration regime that would potentially achieve our target CSF concentration within 30 minutes of start of infusion of IL-1RA with the lowest peak plasma concentration (
Summary of proposed treatment regimes including estimated peak plasma concentrations and estimated times to reach 100 ng/mL in the CSF
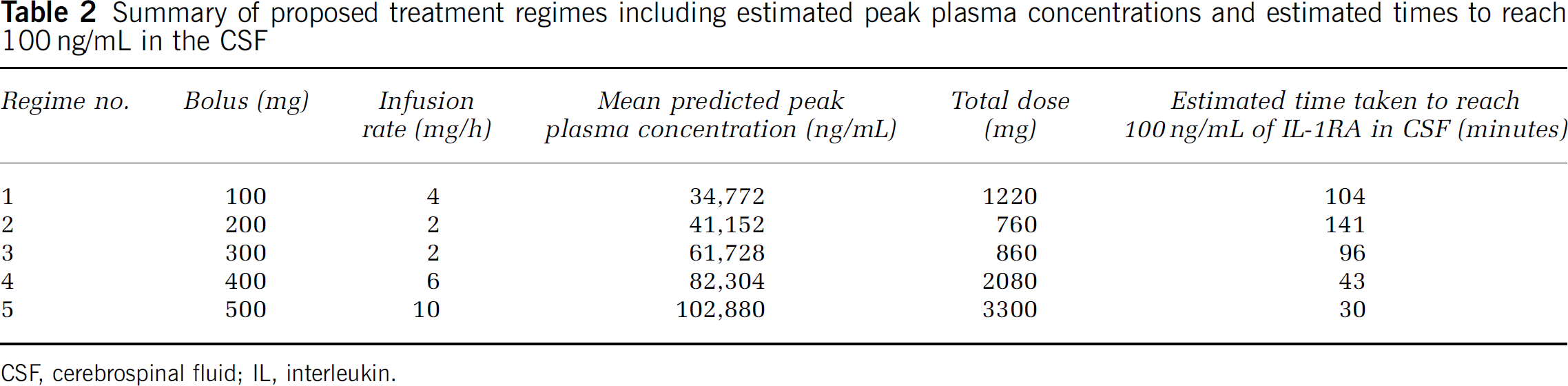
CSF, cerebrospinal fluid; IL, interleukin.
The published PPK model was based on a single-dose regime using a much lower bolus dose and infusion rates of intravenous IL-1RA. Given that earlier experimental data had indicated that the IL-1 family (IL-1α, IL-1β, and IL-1RA) is transported through a saturable mechanism across the BBB (Banks et al, 1991; Gutierrez et al, 1994), it was important to determine whether data generated during this study would match the concentrations profiles predicted by the model. Prediction intervals for plasma and CSF for each of the administration regimes were therefore calculated. To further optimize the efficacy and reduce the risk of introducing central nervous system infection by unnecessary repeated sampling, the optimal sampling time points for plasma and CSF were determined by pharmacometric analysis using published techniques (Ogungbenro et al, 2005).
Patients received anakinra within a mean of 4 days (range, 2 to 12 days) from ictus. Baseline blood and CSF samples were obtained within 5 minutes before anakinra administration for measurement of IL-1RA concentrations and determination of preinfusion biochemical and hematological profiles. Participants were administered a bolus of anakinra over 1 minute through a dedicated intravenous line that was immediately followed by a continuous infusion of anakinra diluted in 500 mL of clinical grade 0.9% saline over 4 hours through a volumetric pump (Graseby, Watford, UK). Five patients were allocated to each of the five regimes sequentially.
Samples of up to 3 mL of CSF and up to 5 mL of blood were obtained using a sterile nontouch technique after removal and discard of ~2 mL of CSF or blood. At 10, 20, 30, 45, 60, 90, 120, 240, 300, 360, 540 minutes and at days 1, 2, 3, and 7 ± 1, CSF and plasma samples were collected in EDTA and anticoagulant-free tubes, respectively, and kept at 0°C to 4°C. Samples were centrifuged at 2000
The occurrence of adverse events was monitored by the research team. Full clinical examinations were performed at days 1, 2, 3, and 7 ± 1 after infusion. Hematological, biochemical, and microbiological results were monitored on a daily basis until day 7 after commencement of infusion. The CSF was sent for microscopy, culture and antibiotic sensitivity whenever sampled for research purposes. The EVD infections were defined as the presence of a ratio of white cells: red blood cells of > 500 in the CSF or the presence of organisms in two consecutive CSF samples. They were documented as being expected if the drains had been
Concentration profiles of anakinra in plasma and CSF were analyzed to ensure that they did fit within prediction intervals calculated
Results
Safety
All patients completed the 4-hour infusion of anakinra. Pharmacokinetic data for CSF for the three patients recruited from Cambridge had to be omitted because of contamination with plasma resulting in aberrant IL-1RA concentrations. There were four deaths during the 7-day study period and all of these were related to cerebral ischemia. One of these patients had demonstrable absence of filling of the ipsilateral middle cerebral artery at the time of initial angiography before commencing the infusion.
The infection rate for EVDs was 3/25 or 12%, with two of these being expected. An independent audit performed by the neurosurgical department during the same period showed an overall infection rate for EVDs in the neurosurgical unit of 20%. The complete list of adverse events is listed in Table 3. All adverse events were reported to the Independent Data Monitoring and Safety Committee but none were deemed attributable to the study drug.
List of adverse events reported to the IDMSC during the study
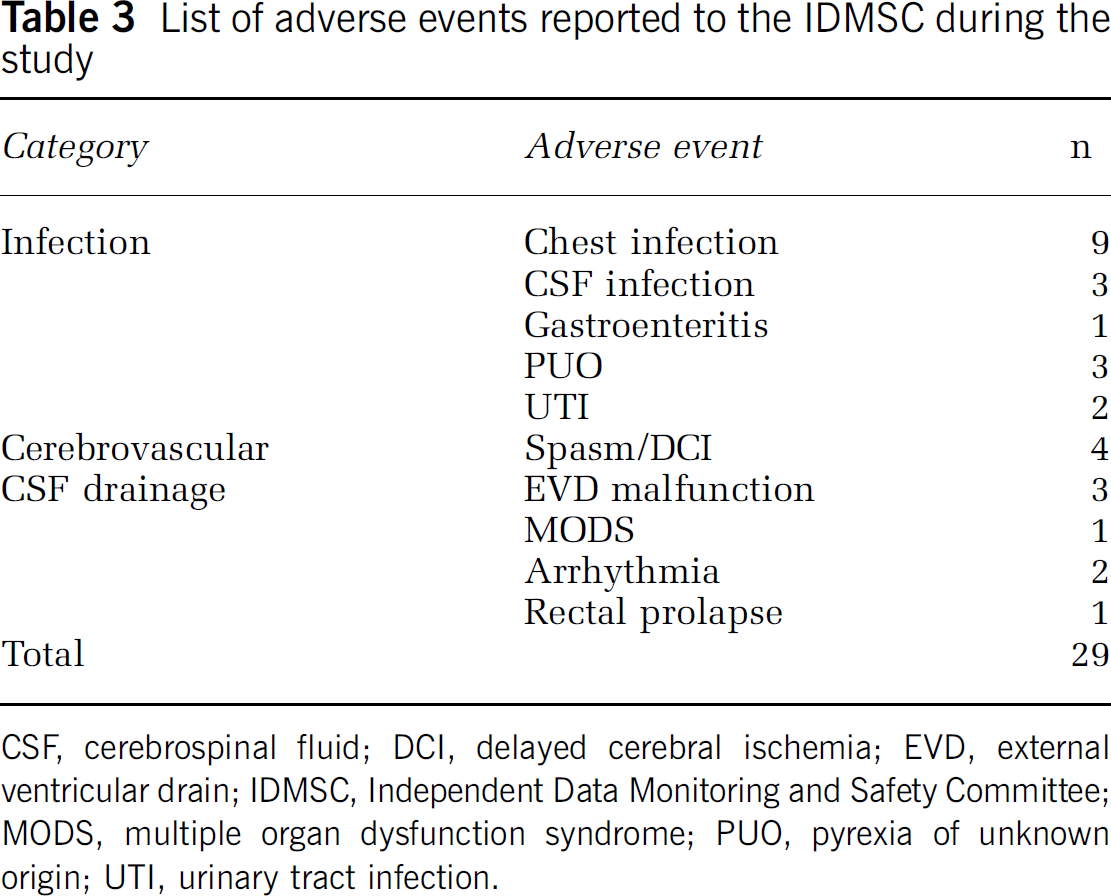
CSF, cerebrospinal fluid; DCI, delayed cerebral ischemia; EVD, external ventricular drain; IDMSC, Independent Data Monitoring and Safety Committee; MODS, multiple organ dysfunction syndrome; PUO, pyrexia of unknown origin; UTI, urinary tract infection.
Effect of Hematological and Biochemical Parameters
There was a statistically significant reduction in neutrophil counts between before administration and day 1 after administration of anakinra (
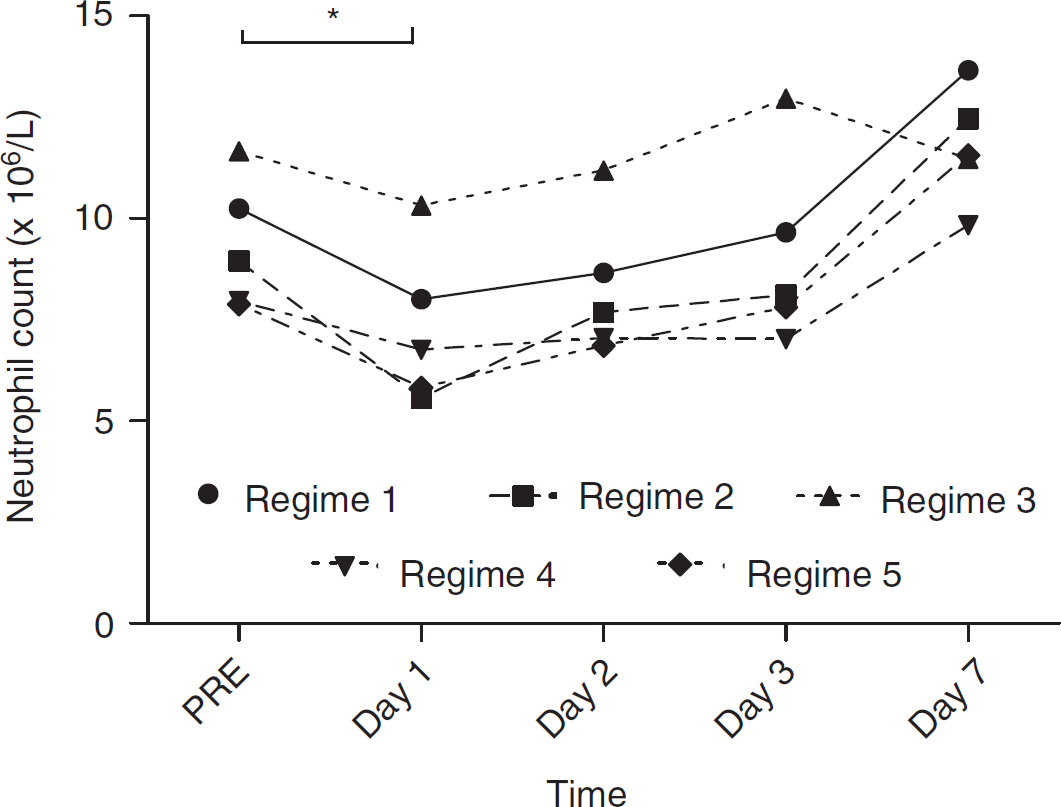
Neutrophil count pre and days 1, 2, 3, and 7 after administration of anakinra (*
Pharmacokinetics of Anakinra
All IL-1RA plasma concentrations from the five regimes fitted the prediction intervals that were calculated
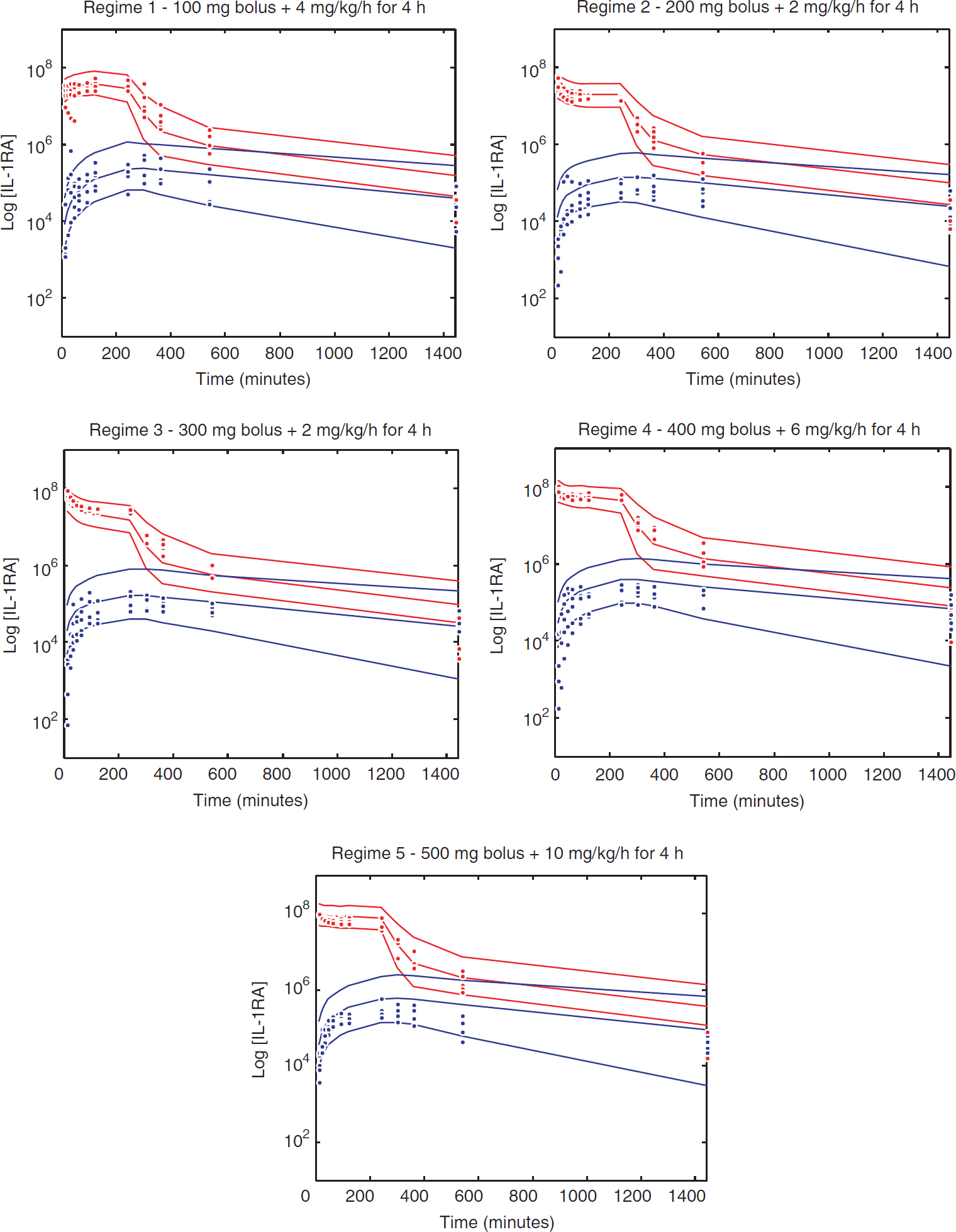
Predicted plasma (red lines) and cerebrospinal fluid (CSF) (blue lines) mean and interval concentration profiles, and actual plasma (red points) and CSF (blue points) for each regime. IL, interleukin.
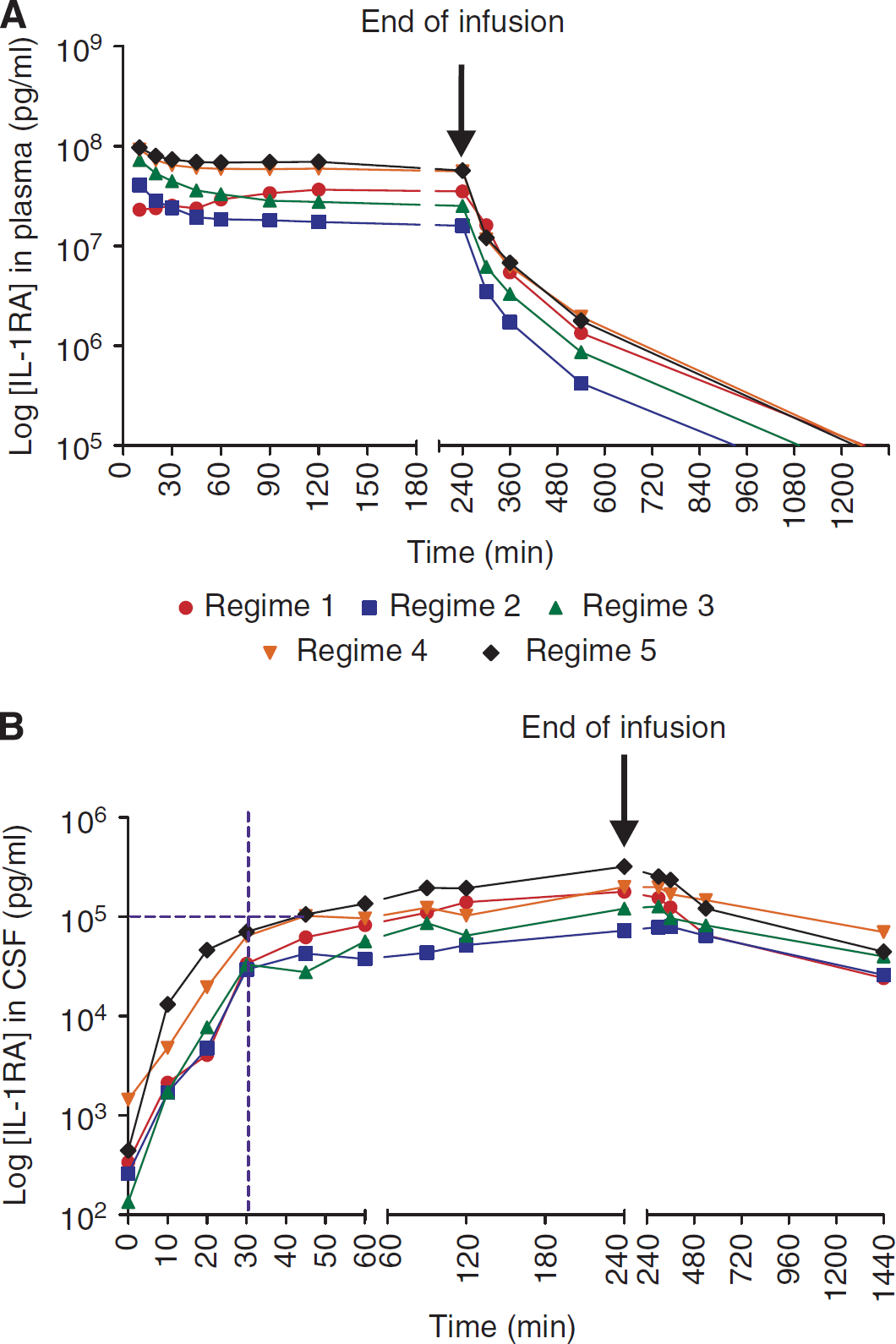
Mean plasma (
The mean baseline concentration of IL-1RA in CSF was 606 pg/mL (± 1300 pg/mL). The concentration of IL-1RA in CSF after intravenous infusion of anakinra increased slowly over the 4-hour period and continued to rise for a variable period beyond the cessation of infusion. Steady state concentrations were not reached. Concentrations in CSF decreased slowly with an initial half-life of 238 minutes for regime 5. Area under the curve analysis for each of the regimes comparing plasma and CSF concentrations showed that 1.6% (± 0.4%) of intravenous administered anakinra crossed into the CSF of patients with SAH. There was no relationship between the administration regime and amount of IL-1RA entry into CSF.
The cumulative pharmacokinetic data from the model-making study and the current study fit a two-compartment and a one-compartment linear model for plasma and CSF, respectively. The IL-1RA concentration achieved in CSF in regime 5 at 30 minutes was 70,403 ± 23,417 pg/mL and at 60 minutes was 135,909 ± 45,963 pg/mL. The concentrations observed at 30 minutes were less than those predicted. Simulations using this updated PPK model would suggest that a regime consisting of an intravenous bolus of 1 g of anakinra followed by 10 mg per kg per hour would potentially achieve 100 ng/mL of anakinra in CSF within 30 minutes.
Studies investigating penetration of IL-1RA past the BBB have been performed in rodent models using radiolabeled substrates (Banks et al, 1991; Gutierrez et al, 1994). These studies have shown that the transport mechanism is saturable by virtue of varying degrees of mutual cross-inhibition of entry of IL-1α, IL-1β, and IL-1RA across the BBB. The percentage transfer of IL-1RA across the blood–CSF barrier in our study ranged from 0.97% to 1.27% and did not differ significantly in our five regimes, suggesting that transport of IL-1RA using administration regimes up to 500 mg bolus and 10 mg per kg per hour is largely passive.
Discussion
This dose-ranging study has determined the optimal dose regime required to safely achieve an experimentally therapeutic IL-1RA concentration in CSF within a time window that would be appropriate for the treatment of acute cerebral ischemia. This regime has been identified as an intravenous bolus of 500 mg administered over a minute followed by intravenous infusion of 10 mg per kg per hour. The study has also explored the effects of altering the bolus dose and the infusion rate on the time to reach steady state and
Anakinra has an excellent safety and tolerability profile in the subcutaneous formulation that is currently licensed for use in rheumatoid arthritis and has been used in clinical trials for type 2 diabetes (Larsen et al, 2007), juvenile arthritis (Ilowite et al, 2009), Muckle Wells syndrome (Hawkins et al, 2004), Schnitzler's syndrome (Schneider et al, 2007), and non-ST segment myocardial infarction. Concerns over the potential risk of infection have occasionally arisen given the slight increase (2% in anakinra patients versus < 1% in placebo) in rheumatoid arthritis patients (Nuki et al, 2002). This increase in infection rate occurred in the context of long-term administration in patients that were on a variety of immune-modulating drugs such as steroids and methotrexate. The intravenous formulation has already been trialled in studies of patients with acute sepsis without any safety concerns and the administration regime used had already been used by our group in the model-making study in SAH patients. In this study, however, the infusion rate and
Plasma concentrations of IL-1RA after intravenous anakinra administration were predicted very accurately by our previously published model and the deviation from the mean individual predicted values was low. Although CSF concentrations during the infusion and immediate postinfusion period of most patients did fit within the 2.5% to 97.5% prediction intervals, the spread around the mean individual predicted profile was much larger. This was a reflection of the relatively unconstrained nature of the original model equation predicting CSF concentrations. The CSF concentrations in the later phase (terminal half-life period) varied considerably. At such low concentrations, the endogenous production of IL-1RA significantly affects the overall (endogenous IL-1RA and anakinra) IL-1RA concentrations and probably accounts for moderate deviations from the predicted mean. The CSF infection, inflammation from mechanical irritation of brain parenchyma, and possibly inflammation as a response to delayed cerebral ischemia may account for elevated endogenous concentrations of IL-1RA.
A key question governing the pharmacokinetics of IL-1RA that could affect the applicability of our PPK data to patients with good grade SAH and patients with other forms of acute cerebrovascular disease is the degree of breakdown of compartmentalization of inflammation. We are aware that our patient cohort may not be representative of the general population suffering from SAH given those patients who require EVDs tend to represent the poorer grades, have more brain edema and may consequently exhibit a leakier BBB and blood–CSF barrier. Similarly, it may be debatable whether the pharmacokinetics of anakinra in this subpopulation of SAH patients is similar in other acute cerebrovascular disease states. It is, however, exceedingly difficult to gain repeated access to CSF in diseases such as stroke, as this can precipitate incipient tonsillar brain herniation, is not warranted for clinical reasons, and may cause unnecessary patient distress.
Another dilemma that may affect the validity of our study is the likely site of action of IL-1RA. If the main mode of action of IL-1RA is within the BBB, brain extracellular fluid concentrations associated with experimental neuroprotection may be more important than CSF concentrations. In the absence of reliable mechanisms of detecting concentrations of anakinra within extracellular fluid (unpublished studies using microdialysis of IL-1RA
In contrast to other failed neuroprotective agents for which penetration into the site of action was not shown, there is now significant evidence that IL-1RA enters CSF and that the rate at which this occurs can be safely modulated by altering the administration regime. A functional PPK model for anakinra has potential significant clinical therapeutic implications. If IL-1RA is proven to be neuroprotective and its efficacy is maximal within a certain therapeutic time window, administration of the drug may be individually tailored to patients to ensure maximal efficacy. Phase II efficacy studies informed by safety and PPK data from this study are currently under way. We believe that our approach may be widely applicable to the evaluation of other pharmacological therapeutic strategies targeting mechanisms within the central nervous system.
Footnotes
Acknowledgements
The authors are grateful to Amgen Inc (CA, USA) for providing the IL-1RA as anakinra, to the Medical Research Council (MRC; UK) for funding the study, and Salford Royal NHS Foundation Trust for funding the author and acting as sponsor for the study. The authors are also grateful to the members of the Independent Data Monitoring and Safety Committee: Professor G Ford (Newcastle), Dr S Lane (Liverpool), and Mr P Whitfield (Plymouth); and the Trial Steering Committee: Professor A Burns (Manchester), Professor D Crossman (Sheffield), Professor C Moody (MRC), Mr A Vail (Salford), Dr L Gregory (Sponsor representative), and Sandra Buckley (BASIC, Salford). The authors also thank Rachel Georgiou (Salford R&D), the patients who kindly participated in this study, and the neurosurgical team at Hope Hospital for their support.
The authors declare no conflict of interest.