
Abstract
The pathogenesis of delayed cerebral ischemia (DCI) after aneurysmal subarachnoid hemorrhage (SAH) remains unknown. Besides vasospasm, microthrombosis might have an important function. As in patients with thrombotic thrombocytopenic purpura an A Disintegrin And Metalloprotease with ThromboSpondin repeats-13 (ADAMTS13) deficiency leads to higher concentrations of large von Willebrand factor (vWF) multimers resulting in microthrombosis, our purpose was to compare ADAMTS13 and vWF in patients with and without DCI after aneurysmal SAH. We measured ADAMTS13 activity, vWF antigen, vWF propeptide, and vWF ristocetin cofactor activity in plasma at standard intervals. Thirty-one patients were included. Eleven patients (35%) developed DCI. No differences were observed in baseline characteristics between patients with and without DCI. Patients with DCI had a stronger decrease in ADAMTS13 activity, and a more profound increase in vWF antigen, vWF propeptide, and vWF activity in the first few days after the hemorrhage (
Introduction
Delayed cerebral ischemia (DCI) is a common complication after aneurysmal subarachnoid hemorrhage (SAH), which occurs in approximately 30% of patients (Roos et al, 2000). Although DCI is common, the pathogenesis of DCI has not yet been elucidated. Clinical signs and symptoms of DCI are often attributed to macrovascular vasospasm shown by angiography. However, DCI can occur in the absence of vasospasm, and, conversely, severe vasospasm can occur in the absence of symptoms of DCI. In an autopsy study, cortical infarcts were found in 78% of cases and represented the most common infarct pattern (Neil-Dwyer et al, 1994; Stoltenburg-Didinger and Schwarz, 1987). These lesions typically occurred in areas covered with subarachnoid blood, suggesting local effects of the clot. Especially for these cortical infarctions, several factors other than macrovascular spasm can be responsible, such as microthrombosis, embolic infarcts, microvascular spasm, and cortical spreading ischemia (Vergouwen et al, 2008; Romano et al, 2002; Dreier et al, 2006).
Von Willebrand factor (vWF) is a glycoprotein that induces platelet adhesion and aggregation at sites of vascular injury or under stress conditions. VWF is secreted as UltraLarge von Willebrand factor (ULvWF) multimers from Weibel–Palade bodies in the vascular endothelium and from
As in patients with aneurysmal SAH microthrombosis might have a role in the pathogenesis of DCI, the purpose of this study was to investigate whether a similar pathogenesis of microthrombi, as has been shown in thrombotic thrombocytopenic purpura, is also present in SAH. Therefore, we compared serial measurements of vWF and ADAMTS13 in patients with and without DCI after aneurysmal SAH.
Materials and methods
We used plasma samples from an exploratory single center, prospective, randomized, double-blind, placebo-controlled trial investigating the effects of simvastatin on endothelial function, coagulation, fibrinolysis, and inflammation in patients with aneurysmal SAH (Vergouwen et al, 2009). This study was registered in the International Standard Randomised Controlled Trial registry (ISRCTN45662651) and approved by the local Institutional Review Board. In this study, use of simvastatin did not influence any parameters of endothelial function (including vWF antigen), coagulation, fibrinolysis, and inflammation, and no effect was observed on vasospasm as detected with transcranial Doppler (TCD) or clinical signs and symptoms of DCI (Vergouwen et al, 2009). Therefore, all patients of the study, except one patient who had no aneurysm on angiography, were included in this study.
Patients
Patients with signs and symptoms of aneurysmal SAH admitted to the Academic Medical Center, Amsterdam, the Netherlands were included if a computed tomography (CT) scan showed an aneurysmal or perimesencephalic bleeding pattern, in combination with the presence of an appropriate aneurysm at angiography, and if written informed consent was obtained. Exclusion criteria were (1) under 18 years of age; (2) if death seemed imminent; (3) patients using aspirin, warfarin, or statins; (4) more than 72 h after SAH; (5) contraindication for simvastatin (active liver disease, liver alanine aminotransferase, or aspartate aminotransferase more than three times the normal upper limit, myopathy); (6) kidney insufficiency; and (7) pregnancy or lactation. All patients received standard care including treatment with nimodipine 360 mg a day orally (60 mg every 4 h). Initiation of hypertension and hypervolemia therapy was at the discretion of the treating neurosurgeon, according to the Academic Medical Center Subarachnoid Hemorrhage Treatment guideline to which all neurologists, neurosurgeons, and intensive care physicians adhere.
At baseline, several baseline characteristics were recorded such as age, sex, Glasgow Coma Scale, presence of focal neurologic deficits, loss of consciousness during ictus, warning leak, blood pressure at admission, smoking, history of hypertension, and location of aneurysm.
DCI was defined as the gradual onset of new focal neurologic impairment and/or a decreased level of consciousness of at least two points as recorded on the Glasgow Coma Scale, either with cerebral infarction on CT scan compatible with clinical presentation or proven at autopsy, or in case no CT scan or autopsy was obtained, suspect for infarction with exclusion of other causes by appropriate laboratory studies (Van Gijn et al, 1994). Events were scored by one investigator (MDIV), and in case of uncertainty discussed with another investigator (YBWEMR).
Ancillary Investigations
The amount of blood on admission CT scan was calculated using the Hijdra score (Hijdra et al, 1990). Blood withdrawals were performed at six standardized moments during hospitalization: 2±1, 4±1, 7±1, 10±1, 14±1, and 17±1 days after SAH, between 8 a.m. and 9.30 a.m. avoiding the effect of diurnal fluctuations in blood parameters. During the first blood withdrawal at day 2, and the last at day 17 after SAH, patients did not use study medication. All blood withdrawals were performed by the same investigator (MDIV). In case of hospital discharge before day 17 after SAH, patients did not return to the hospital for the remaining blood withdrawals. After withdrawal, blood was directly processed and stored in a −80°C freezer, until laboratory analyses were performed. In citrate plasma we measured ADAMTS13 activity (Kokame et al, 2005), vWF antigen (ELISA using antibodies from DAKO, Glostrup, Denmark), vWF propeptide (ELISA from Sanquin, Amsterdam, the Netherlands), and vWF ristocetin cofactor activity (BC von Willebrand, Dade Behring, Marburg, Germany). ADAMTS13 antigen and autoantibodies against ADAMTS13 were determined with Imubind ELISA kits from American Diagnostica, only at day 7 after SAH (Greenwich, CT, USA). A plasma sample was considered positive for autoantibodies if the value exceeded that of a locally prepared pooled normal plasma (pool of more than 200 healthy volunteers). Measurements of prothrombin fragment F1+2 (Dade Behring) were performed by ELISA. Interleukin (IL)-6 and tumor-necrosis factor-
Statistics and Analyses
To investigate differences in baseline characteristics between patients with and without DCI we used the unpaired
The possible differences over time in ADAMTS13 activity, vWF antigen, vWF propeptide, and vWF cofactor activity, between the groups of patients with and without DCI were investigated with a linear random effects model, using the nlme package in the R statistical program (R Development Core Team, 2008). As in the analysis of ADAMTS13 activity levels first decreased and than increased, and in the analyses of vWF antigen, vWF propeptide, and vWF cofactor activity first increased and than decreased over time, a polynomial trend over time was assumed, which was allowed to differ by treatment group. Furthermore, because ADAMTS13 activity might be influenced by IL-6, TNF-
Results
After written informed consent was obtained, 31 patients were included in this study. Baseline characteristics are listed in Table 1. In twenty-four patients (77%) the aneurysms were coiled and in seven patients (23%) clipped. Median day of aneurysm treatment after SAH was day 1 (range 0 to 30).
Characteristics of patients with and without delayed cerebral ischemia
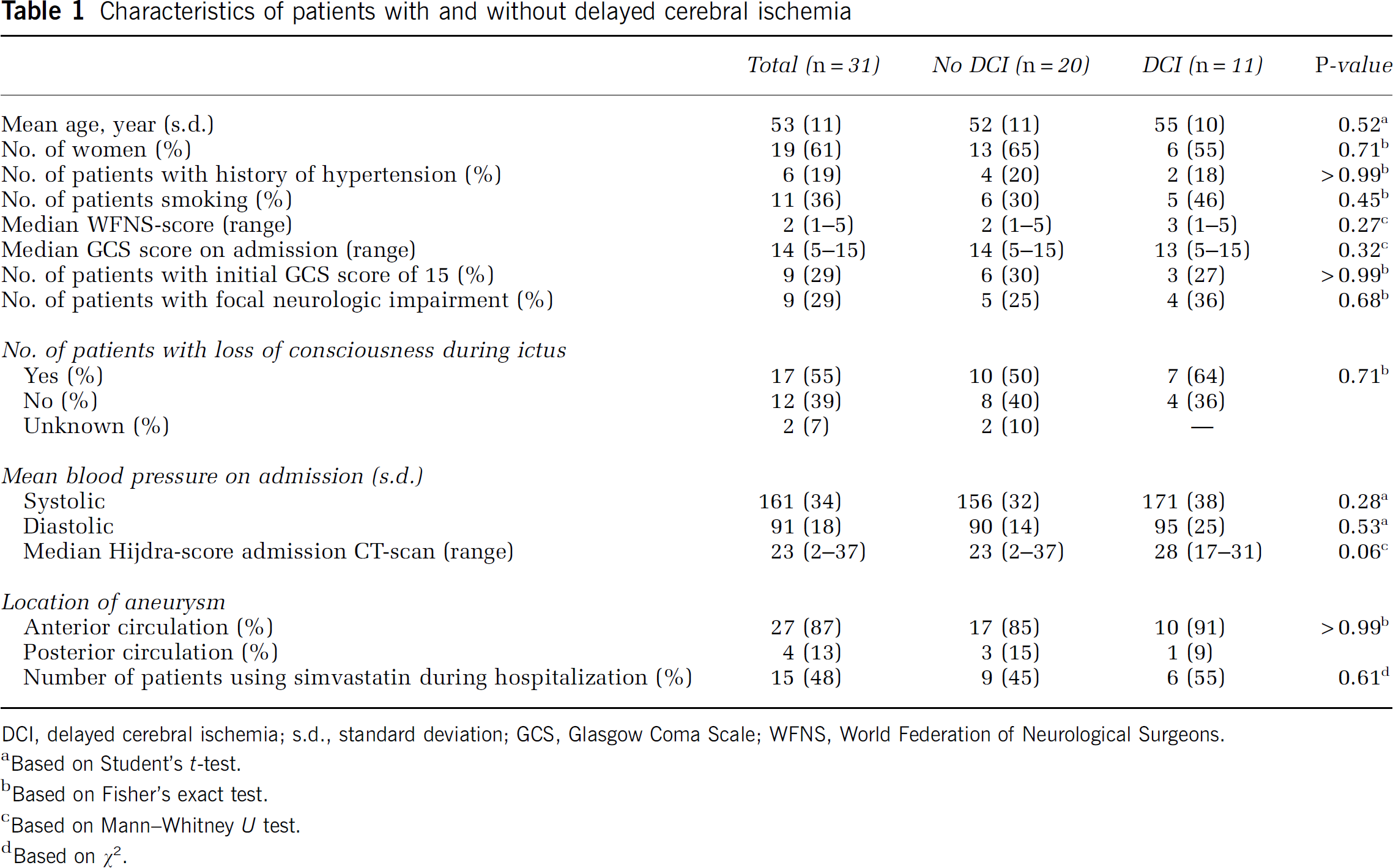
DCI, delayed cerebral ischemia; s.d., standard deviation; GCS, Glasgow Coma Scale; WFNS, World Federation of Neurological Surgeons.
Based on Student's
Based on Fisher's exact test.
Based on Mann–Whitney
Based on
Eleven patients (35%) developed DCI. Signs of DCI started at a median of 6 days (range 4 to 10 days). No differences were observed in baseline characteristics between patients with and without DCI occurrence, although patients with DCI had, as expected, a higher Hijdra score on admission CT scan (
Patients with DCI showed a stronger decrease of ADAMTS13 in the first few days after SAH (
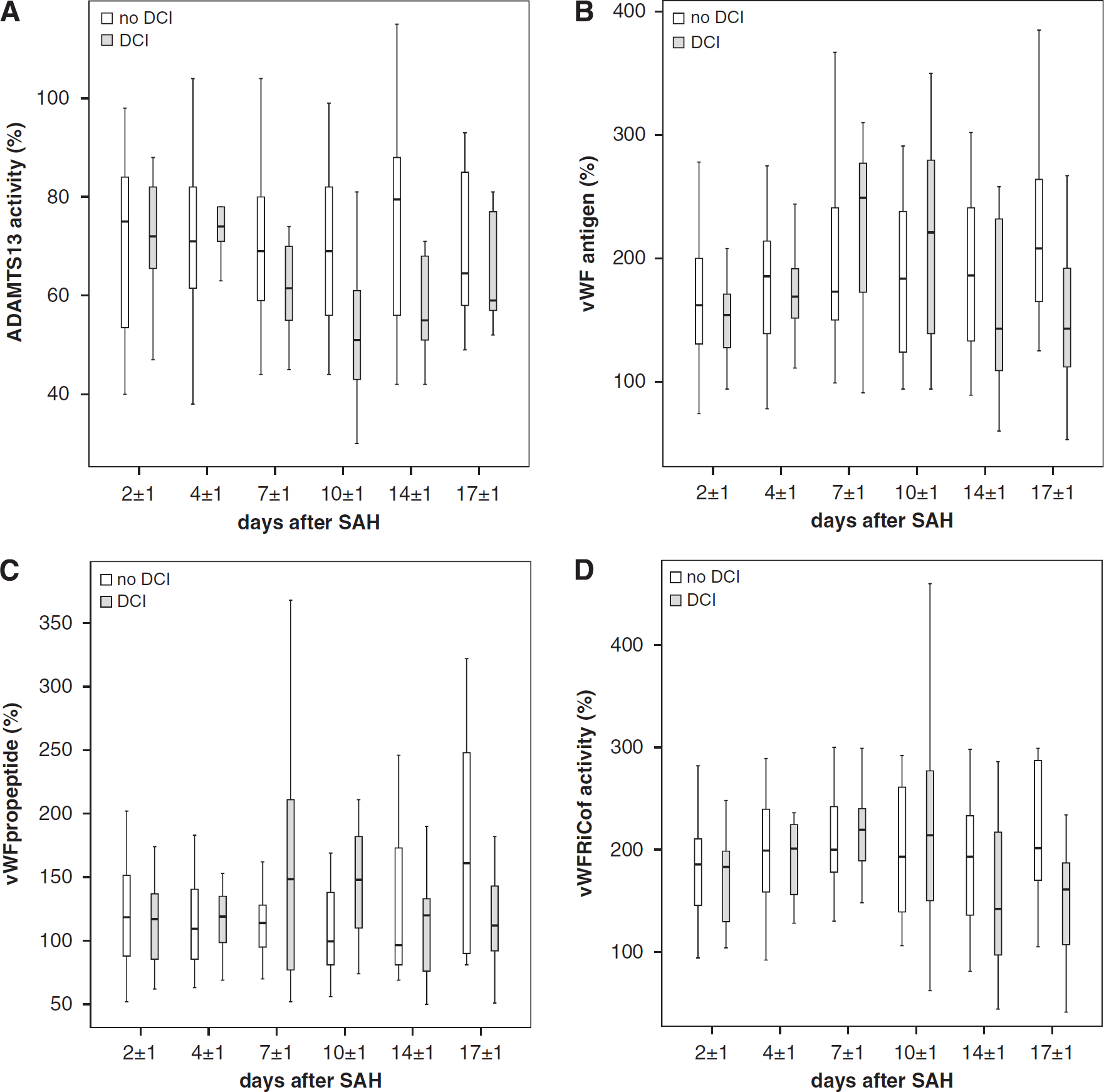
(
Several correlations were investigated. No correlation was found between ADAMTS13 and IL-6 (Spearman correlation coefficient
Discussion
The results of our study show that patients with DCI after aneurysmal SAH have a significantly different development of ADAMTS13 and vWF over time compared with patients without DCI. Patients with DCI had a stronger decrease in ADAMTS13. Interestingly, there was no correlation between vWF antigen and ADAMTS13 activity. In addition, the decrease in ADAMTS13 activity could not be explained as a result of suppression by IL-6, TNF-
ADAMTS13 has never been studied before in patients with aneurysmal SAH. However, some studies investigated ADAMTS13 in ischemic stroke (Bongers et al, 2006; Zhao et al, 2008). In a case–control study of 124 first-ever ischemic stroke patients and 125 age- and sex-matched controls, vWF antigen and vWF activity were associated with the occurrence of acute ischemic stroke (Bongers et al, 2006). This association was not affected by ADAMTS13 activity. As vWF and ADAMTS13 were negatively associated, similar to earlier observations (Mannucci et al, 2004), the question in that study remains whether low levels of ADAMTS13 resulted in higher vWF levels, or whether increased vWF levels resulted in lower ADAMTS13 levels (Bongers et al, 2006). However, in our study investigating DCI after SAH no correlation between vWF and ADAMTS13 was observed. Nevertheless, it cannot be ruled out whether other factors as a result of ischemia decreased ADAMTS13. Recently, a more causal relation between ADAMTS13 and cerebral ischemia was found in an SAH animal model. It was observed that ADAMTS13-deficient mice had approximately 20% larger infarcts after induction of cerebral ischemia (Zhao et al, 2008). Interestingly, infusion of recombinant human ADAMTS13 in ADAMTS13-deficient mice immediately before reperfusion 2 h after occlusion significantly reduced infarct volume with approximately 30% (Zhao et al, 2008).
The results of this study add to an accumulating body of evidence that DCI cannot be fully explained by macrovascular vasospasm. The results of this study suggest that, besides vasospasm-related hypoperfusion, microthrombosis has a more important function in the pathogenesis of DCI than is generally accepted (Vergouwen et al, 2008). Indeed, in autopsy studies microthrombi have been observed consisting of fibrin and activated platelets (Suzuki et al, 1983; Suzuki et al, 1990). Patients who died from DCI had significantly more microthrombi in clinically ischemic regions and in areas showing cerebral infarction on computed tomographic scan, when compared with patients who died from rebleeding or acute hydrocephalus (Suzuki et al, 1990). Furthermore, in up to 70% of SAH patients microembolic signals can be observed with transcranial Doppler ultrasonography, with a trend toward an increased incidence of microemboli in patients with symptomatic vasospasm (Romano et al, 2002). Interestingly, in the described study the incidence of microembolic signals was lower in vessels with radiologic vasospasm compared with those without vasospasm, although not significantly different, which suggests that microemboli are probably not a direct result of macrovascular vasospasm.
As not all patients with DCI have macrovascular vasospasm, and conversely, not all patients with vasospasm have DCI, cerebral microthrombosis might be a
As vWF is a parameter of endothelium function and an important contributor of thrombus formation, the results of this study suggest that endothelium dysfunction and the hemostatic system are involved in the development of DCI. The mechanism by which ADAMTS13 decreases in patients with DCI remains to be elucidated. A plausible explanation might be that an increased use of ADAMTS13 results from higher vWF antigen levels, however in our study no correlation was found between ADAMTS13 activity and vWF antigen. Earlier it has been shown that thrombin and plasmin potentiate the proteolytic inactivation of ADAMTS13, and therefore another explanation might be that ADAMTS13 activity is suppressed by thrombin and plasmin present in the subarachnoid space after the hemorrhage (Crawley et al, 2005). However, in our study no correlation was found between ADAMTS13 activity and prothrombin fragment 1+2, and therefore it is unlikely that the decrease in ADAMTS13 activity in DCI is caused by thrombin. ADAMTS13 activity might also be suppressed by IL-6, because IL-6 inhibits the cleavage of ULvWF by ADAMTS13 under flow conditions (Bernardo et al, 2004). In patients with aneurysmal SAH increased levels of IL-6 are associated with DCI (Hendryk et al, 2004). However, in our study no correlation was found between ADAMTS13 activity and IL-6. Finally, decreased ADAMTS13 activity might be caused by locally present neutralizing antibodies against ADAMTS13. However as discussed above, although we found a trend toward a correlation between ADAMTS13 activity and autoantibodies, the evidence from this study that autoantibodies are the cause of the decrease in ADAMTS13 activity is weak.
The results of this study imply that antithrombotic or anticoagulant drugs might be beneficial in the prevention of DCI. However, earlier attempts to influence procoagulant activity in SAH patients were not successful or inconclusive. A randomized controlled trial investigating the effect of aspirin was stopped prematurely, after an interim analysis showed that the probability of a beneficial effect was negligible (Van den Bergh et al, 2006). Explanations provided were that a dose of 100 mg once daily might not be appropriate, or that aspirin might not be the right antiplatelet drug for the prevention of DCI. Another explanation could be that the effect of aspirin is too selective by only inhibiting platelet function. A Cochrane analysis investigating the effect of antiplatelet therapy showed a strong trend toward a decreased incidence of DCI and poor outcome, but because the results were not statistically significant and antiplatelet therapy was associated with an increased risk of intracranial hemorrhagic complications, the conclusion was that antiplatelet use could not be recommended in SAH patients (Dorhout Mees et al, 2007). Earlier, in a single-blind controlled trial no effect of dipyridamole on the incidence of postoperative ischemic deficits was observed (Shaw et al, 1985). Two randomized controlled trials investigating the effect of enoxaparin showed contradictory results, and therefore it remains unknown whether enoxaparin is effective (Wurm et al, 2004; Siironen et al, 2003). In conclusion, earlier studies showed that investigated drugs influencing the coagulation pathway were inconclusive, and therefore large, well-powered, randomized controlled trials are needed to investigate the effects of these drugs on the incidence of DCI.
A possible limitation of our study is that only systemic levels of biomarkers were assessed instead of local levels from the cerebral circulation. Therefore, the results might not be a good representation of pathophysiological processes in the cerebral circulation. However, our results may also be interpreted as diluted values of locally increased levels, and therefore an underestimation of the local pathophysiological processes. Another limitation is that our study was not designed to measure ADAMTS13 and vWF levels at the days of clinically manifest DCI. Therefore, many blood samples were not taken on the day of first signs of DCI, and our data only indicate that ADAMTS13 decreases and vWF antigen level increases in the time period that DCI develops. Furthermore, this study was a
As in this study no explanation was found for the decrease in ADAMTS13 activity in patients with DCI, and the role of ADAMTS13 and vWF in the development of DCI should be further investigated, we conclude that the results of this study have an important translational aspect, from bedside to bench. Little is known about the factors that increase coagulation activity in the pathogenesis of DCI. The role of Weibel–Palade bodies in the vascular endothelium needs further investigation. Weibel–Palade bodies are storage sites in both the microvascular and macrovascular endothelium, which can rapidly respond to changes in its microenvironment by the release of various substances. Well-known stimulators of Weibel–Palade bodies are (among others) thrombin, complement factors, and epinephrine. In patients with SAH, Weibel–Palade bodies are probably activated by thrombin, present in the subarachnoid space as a direct result of the hemorrhage, inflammatory reactions, or from the stress response. After stimulation, Weibel–Palade bodies release substances such as vWF, endothelin, tissue plasminogen activator, P-selectin, and IL-8. Recent studies indicate that substance release from Weibel–Palade bodies can be selective (Babich et al, 2008). Therefore, in patients with DCI only procoagulatory substances might be released, and not substances such as tissue plasminogen activator, which is profibrinolytic. The fact that substance release from Weibel–Palade bodies can be selective might also explain why macrovascular vasospasm does not always result in clinical signs and symptoms of DCI, and vice versa, not all patients with DCI have vasospasm. For instance, in patients with macrovascular vasospasm without symptoms of DCI, endothelin might be released from Weibel–Palade bodies in the macrovascular endothelium, resulting in vasospasm, without release of procoagulatory substances. In patients with symptoms of DCI without macrovascular vasospasm procoagulatory substances are released without release of endothelin from the macrovascular endothelium. In the latter group of patients it could also be that endothelin is released from the microvascular endothelium, resulting in microvascular vasospasm. In patients with both macrovascular vasospasm and symptoms of DCI both endothelin and procoagulatory substances are released.
Although it would be interesting to further investigate the role of Weibel–Palade bodies in the pathogenesis of DCI, it is currently not an easy scenario, because it is not possible to study Weibel–Palade bodies
We conclude that patients with DCI after aneurysmal SAH show a stronger decrease in ADAMTS13 activity and a more profound increase of both vWF antigen and vWF propeptide levels within the first days after the hemorrhage compared with patients without DCI. Although the results of this study do not prove a causal relationship between decreased ADAMTS13 activity and the pathogenesis of DCI, our results suggest that microthrombosis has a role in the pathogenesis of DCI.
Footnotes
The authors declare no conflict of interest.