
Abstract
We report a new clinically relevant model of neonatal hypoxic-ischemic injury in a 10-day-old rat pup. Bilateral carotid artery occlusion and 8% hypoxia (1 to 15 mins, BCAO-H) was induced with varying degrees of injury (mild, moderate, severe), which was quantified using magnetic resonance imaging including diffusion-weighted and T2-weighted imaging at 24 h and 21/28 days. We developed a magnetic resonance imaging-based rat pup severity score and compared 3D ischemic injury volumes/rat pup severity score with histology and behavioral testing. At 24 h, hypoxic-ischemic injury was observed in 17/27 animals; long-term survival was 81%. Magnetic resonance imaging lesion volumes did not correlate with hypoxia duration but correlated with rat pup severity score, which was used to classify animals into mild (
Introduction
With an occurrence of 3 to 5 cases per 1, 000 births, neonatal hypoxic-ischemic injury (HII) remains a devastating condition with sequelae including cerebral palsy, epilepsy, and cognitive delay (Levene et al, 1986; Rennie et al, 2007). Even newborns with moderate HII are at risk because 30% to 50% develop serious long-term complications (Dilenge et al, 2001). An animal model that adequately mimics the bihemispheric involvement typically seen with human neonatal HII is essential to the development of therapeutic interventions; however, technical limitations have made developing such models difficult. Although the Rice-Vannucci model (RVM) has been the most popular neonatal HII model, it fails to produce the global distribution of injury seen in the full-term newborn (Triulzi et al, 2006).
In modifications of the RVM, other investigators have reported bilateral carotid artery occlusion (BCAO) in P1 and P5 rats, without hypoxia, to model periventricular leukomalacia in the preterm infant (Uehara et al, 1999; Cai et al, 2001). Bilateral carotid artery occlusion has also been used in the P4 rat with 15 mins hypoxia (i.e., BCAO-H) to induce global injury (Cai et al, 2001, 2006). Studies by Fan et al using BCAO-H (10 to 15 mins at 8% O2) in P4 rats correlated injury severity with neurobehavioral performance through 21 days (Fan et al, 2005). Bilateral carotid artery occlusion with hypoxia was performed in rats at an age that corresponded to the preterm infant, resulting in white matter injury with scattered cortical ischemic injury. Bilateral carotid artery occlusion with hypoxia (60 mins at 6.5% or 8% O2) was also used in P7 rats but with severe neocortical infarction and hippocampal neuronal necrosis (Hattori et al, 1989; Hattori and Wasterlain, 1990; Schwartz et al, 1992; Wasterlain et al, 1992, 1993). Currently, a global model of neonatal HII with graded injury similar to the term infant is lacking. This is clinically relevant because the experience with recent hypothermia trials for neonatal HII has shown that stratification of patient injury with careful patient selection is essential, because neonates with moderate HII benefited from treatment whereas those with severe HII did not (Gluckman et al, 2005). An animal model producing graded injury is important because it could determine the treatment that would be most effective for different degrees of injury. This study created a new model of global ischemic injury by exposing P10 rats, the age that correlates with term human neonate to BCAO-H. We hypothesized that varying the degree of injury would lead to magnetic resonance imaging (MRI) and behavioral modifications that would allow stratification of injury severity.
Magnetic resonance imaging is an important tool for assessing the evolution, pathogenesis, and severity of focal and global HII clinically and in animals (Kuenzle et al, 1994; Rutherford et al, 1996; Barnett et al, 2002; Fraser et al, 2007; Yang and Wu, 2008). The Barkovich score was developed to use early (<10 days after birth) MRI data to assess specific patterns of injury that could prognosticate long-term outcomes of asphyxiated term neonates (Barkovich et al, 1995, 1998). This clinical scoring system successfully predicted neuromotor outcome at ages 3 and 12 months and cognitive outcome at 12 months based on a combined basal ganglia/watershed (BG/W) score garnered from T1- (T1WI) and T2-weighted imaging (T2WI). Rutherford and colleagues used a similar MRI score that correlated with locomotor function at 2 and 4 years and neurologic examinations at 9 to 14 months of age (Haataja et al, 2001). This group also showed that abnormal signal in the posterior limb of the internal capsule predicted impairments at 1 year in neonates with HII (Rutherford et al, 1998). Using the BCAO-H model in the P10 rat, we also developed a novel imaging-based rat pup severity score (RPSS) that is easy to use, rapid, objective, designed to aid in the stratification of HII, and substitute for subjective and time-consuming area or volumetric analysis techniques. This simplified scoring system adds to the clinical translatability of the model in which it parallels the Barkovich and Rutherford scoring system (Barkovich et al, 1998; Haataja et al, 2001).
Neurologic outcomes in animal models can be assessed by behavioral testing that defines the range of deficits produced by HII and allow the evaluation of potential therapies. In neonates, pharmacological intervention decreased brain injury with reduced behavioral deficits in P7 rats (Bona et al, 1997) following RVM (100 mins of hypoxia). However, another study showed that neuronal protection does not necessarily lead to functional recovery in gerbils that experienced BCAO without hypoxia (Shuaib et al, 1996). Conversely, environmental enrichment and social interaction improved motor outcomes without affecting lesion size in middle cerebral artery occlusion rats (Ohlsson and Johansson, 1995; Johansson and Ohlsson, 1996). We examined behavioral outcomes in our BCAO-H model to determine whether a gradation of injury would produce a gradation of long-term behavioral deficits.
This study is the first to describe a 10-day-old neonatal model of BCAO-H using MRI to noninvasively describe the (1) temporal extent of injury, (2) development of the clinically relevant RPSS to stratify injury severity, and (3) neurobehavioral measures that showed graded alterations to graded injury severity.
Materials and methods
All protocols were approved by the Loma Linda University Medical Center Institutional Animal Care and Use Committee.
Bilateral Common Carotid Artery Occlusion With Hypoxia
Global ischemia was induced by bilateral occlusion of the common carotid arteries in unsexed P10 Sprague-Dawley rat pups (Harlan, Livermore, CA, USA) (
Magnetic Resonance Imaging
Magnetic resonance imaging was performed at 24 h (
BCAO-H severity groups, survival and hypoxia durations
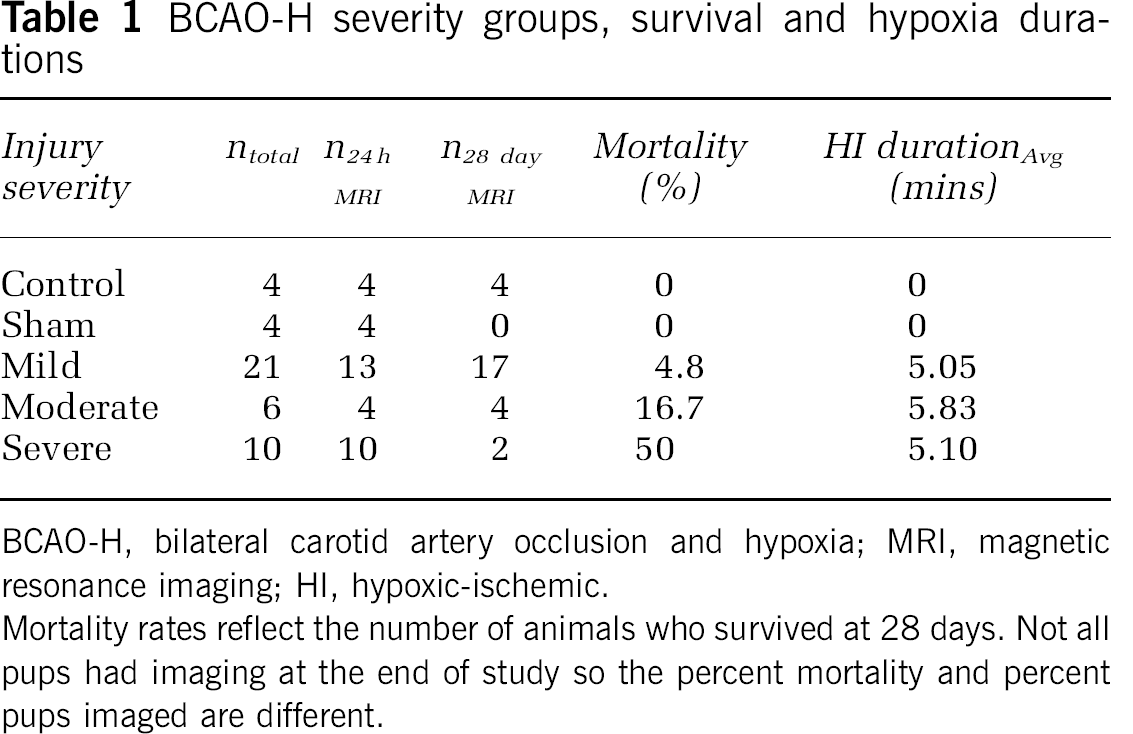
BCAO-H, bilateral carotid artery occlusion and hypoxia; MRI, magnetic resonance imaging; HI, hypoxic-ischemic.
Mortality rates reflect the number of animals who survived at 28 days. Not all pups had imaging at the end of study so the percent mortality and percent pups imaged are different.
Volumetric Image Analysis
Volumetric MR image analysis methods in this study are similar to that in our earlier studies (Ashwal et al, 2006, 2007). Using Amira software (Mercury Computer Systems, Visage Imaging, Inc., San Diego, CA, USA), T2 and DW images were analyzed using regions of hypo- or hyperintensity to delineate the spatial development of the infarct volume. Analysis was performed by an investigator masked to hypoxia duration and included infarct volume (total, cortical, striatal, and hippocampal), noninfarct brain volume, and total brain volume as reported earlier (Ashwal et al, 2007).
Rat Pup Severity Score
The RPSS was developed as an MRI-based method to rapidly evaluate the severity of HII in neonatal rat pups, similar to the Barkovich score (Barkovich et al, 1995, 1998). For each MR slice (anterior to posterior), the image was delineated into four quadrants that were scored (i.e., dorsal/ventral for right and left hemisphere) individually by a blinded investigator (Figure 1). Regions of interest included dorsal and ventral areas of the cortex, BG, and hippocampus. A score of 1 was assigned when abnormal MR signal intensity (bright on T2/DWI) was observed in a region; a score of 0 was assigned when the signal appeared normal. Scores from each slice were totaled and divided by the total number of slices scored to generate the final RPSS.
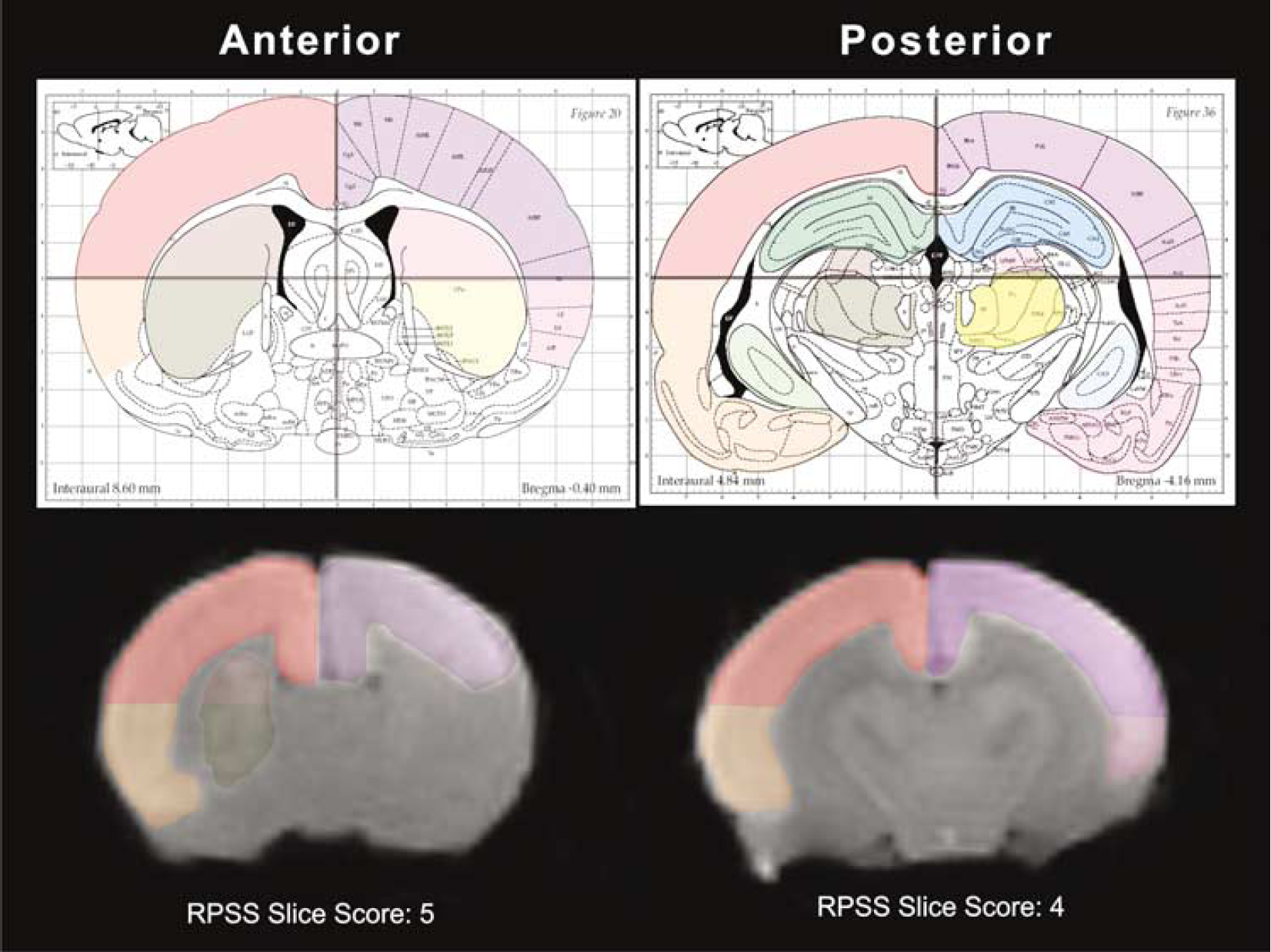
Rat pup severity score. A visual method to quantify the extent of HII in the neonatal rat BCAO-H model. Each T2WI was scored from anterior to posterior and three regions from each hemisphere were scored: (1) dorsal and ventral cortex; (2) subcortical regions (basal ganglia and thalamus); and (3) hippocampus. No injury would have an average RPSS of 0, whereas a severely injured BCAO-H pup could have a score > 5. In this example, an anterior MR slice was scored with 5, whereas a more posterior slice received a score of 4. This animal received a final RPSS of 5.5 and was classified as severe (lesion volume: 45.7%).
Histology
After completion of imaging, animals were perfused intracardially with 4% paraformaldehyde (1 mL/g of body weight, pH 7.3) as described earlier (Ashwal et al, 2007). Postfixation, brain tissue was rinsed 3 × with phosphate buffered saline and cryoprotected in 30% sucrose before being frozen in optimal cutting temperature compound (O.T.C., Tissue Tek, Sakura, Torrance, CA, USA). Coronal cryostat sections (30 μm) containing ischemic brain tissue were obtained from three animals in each severity group in an anterior to superior direction (Leica CM1850, Leica Microsystems GmbH, Wetzlar, Germany). Sections were mounted on gelatin-chrome-alum coated slides. Cresyl violet acetate (0.5%) was used to determine the presence of cellular damage. Slides were permanently cover-slipped using Permount mounting medium (Electron Microscopy Sciences, Hatfield, PA, USA).
Histologic Scores versus Injury Severity
We used a standard histologic scoring system for the pup RVM model to grade injury severity (Muramatsu et al, 2000) and compared this with our RPSS score. Cresyl violet-stained sections were scored as (1) no detectable neuronal cell loss, (2) small focal areas of neuronal loss, (3) columnar damage in the cortex involving predominately layers II to IV or moderate cell loss in the hippocampus or striatum, and (4) cystic infarction and gliosis. Eight brain regions were examined bilaterally and scored (hippocampus: CA1, CA2, CA3, dentate gyrus; anterior and middle regions of the cortex and striatum) and a total score was recorded. This score was compared with pups designated as controls or mild, moderate and severe injure based on the RPSS and 3D volumes.
Behavioral Testing
Behavioral testing began 29 days after surgery (P39) and consisted of a test battery designed to assess a wide variety of behavioral domains (Hartman et al, 2005). Open field, water maze, and rotarod tests were used to assess activity levels, learning and memory, and sensorimotor coordination.
Statistical Analysis
An α-level of 0.05 was used for all tests of statistical significance.
Results
Animal survival at 3 days after BCAO-H was 81%; animals surviving this 3-day window survived until study completion. Average body weight before injury for all animals (
Magnetic Resonance Imaging
Signal abnormalities at 24 h on T2WI and DWI were exhibited in 17 of 27 BCAO-H pups (Figure 2). At 21/28 days, 8 out of 23 animals showed imaging abnormalities on T2WI and DWI. Abnormalities were not observed in naive control and sham animals at either time point. Regional analysis showed that the evolution of injury in the cortex and striatum was similar with no differential anatomic progression. Distribution of HII in the BCAO-H model clearly shows an anterior-posterior extent (Figure 2A). A typical injury distribution in a moderately injured animal included a hyperintense signal that occurred in a majority of the cortex in one hemisphere and spread to the dorsal cortex of the other hemisphere. Hyperintense signals were also present in the anterior striatum, again occurring mainly in one hemisphere with a partial appearance on the other. Hippocampal signal change was observed only in severely injured animals. At 21/28 days, a similar injury pattern was seen on T2WI and DWI but with a reduction in the area of hyperintensity.
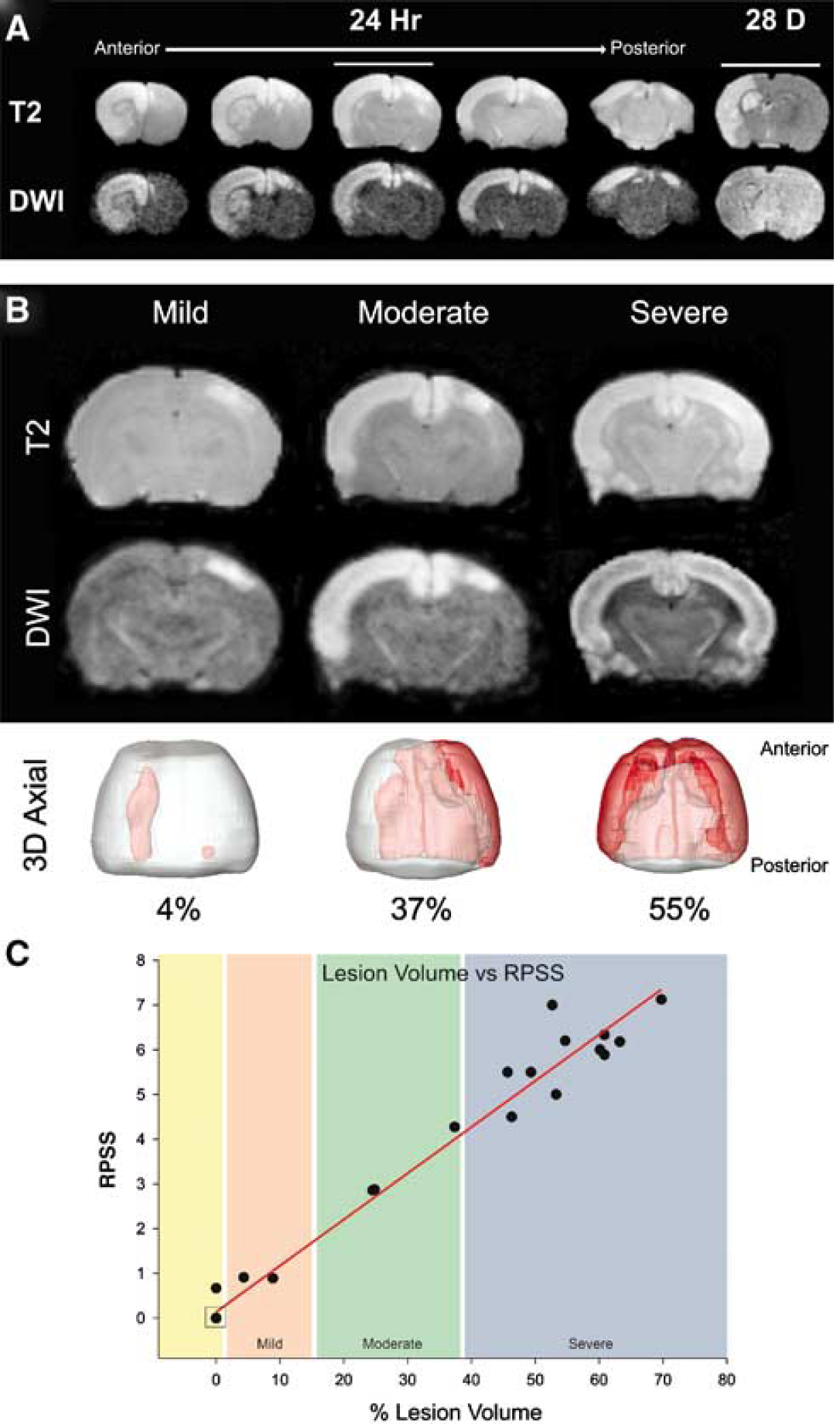
Injury distribution and severity in the BCAO-H model. (
Volumetric analysis from all BCAO-H animals (mild, moderate, severe) showed that average brain lesion volume at 24 h decreased during the subsequent 28 days (6.0% ± 0.5) (
Rat Pup Severity Score
Bilateral carotid artery occlusion with hypoxia was performed with eight durations of hypoxia (1, 2, 3, 4, 5, 8, 10, and 15 min) in an effort to produce a gradation of injury, similar to that observed clinically. We chose these short time intervals in an effort to develop a model with varying degrees of injury severity. The duration of hypoxia was significantly greater (
Histology
Cresyl violet staining revealed neurodegeneration in the moderate and severe BCAO-H injury groups (Figure 3). Cortical regions were affected bilaterally in the severe group, including a near complete loss of tissue, and unilaterally in the moderate group, reflecting recovery in the hemisphere that exhibited the least injury. The frequency of pyknotic cells increased with severity; these cells were detected in cortical regions bordering the lesion area in mild and moderate HII groups (Figure 3A). Animals in the mild group, which did not exhibit MRI visible HII, had mild cortical injuries similar to animals in the mild group with MR visible injuries.
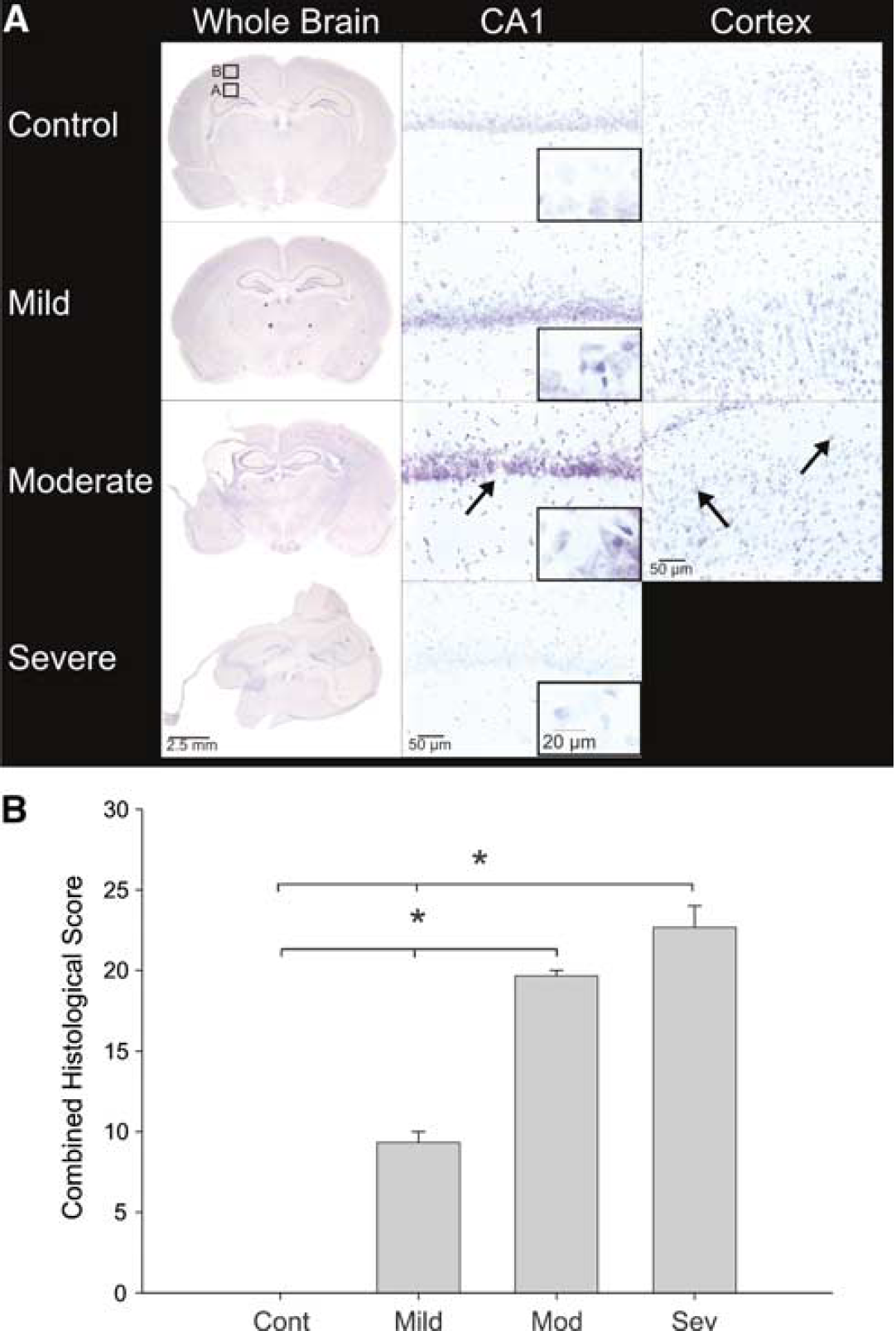
Histology and quantification of neuropathology. (
Within the hippocampus, pyramidal cells in the CA1 layer were greatly affected by HII (Figure 3A). The hippocampus displayed a sparse staining pattern in the mild group with an increasing weakness in staining, indicative of cell loss. Animals in both moderate and severe groups displayed shrunken cells with pyknotic nuclei, indicative of cell death, and decreased cellular organization with sparse staining and breaks in continuity of the tract. In the case of the severe group, the hippocampal CA1 subfield was virtually nonexistent.
Histologic Scores versus Injury Severity
Histologic scores from eight brain regions correlated with BCAO injury severity as shown in Figure 3B. All BCAO-H severity groups had histologic injury scores greater than controls; those with moderate or severe injury had scores greater than those with mild injury (
Behavioral Testing
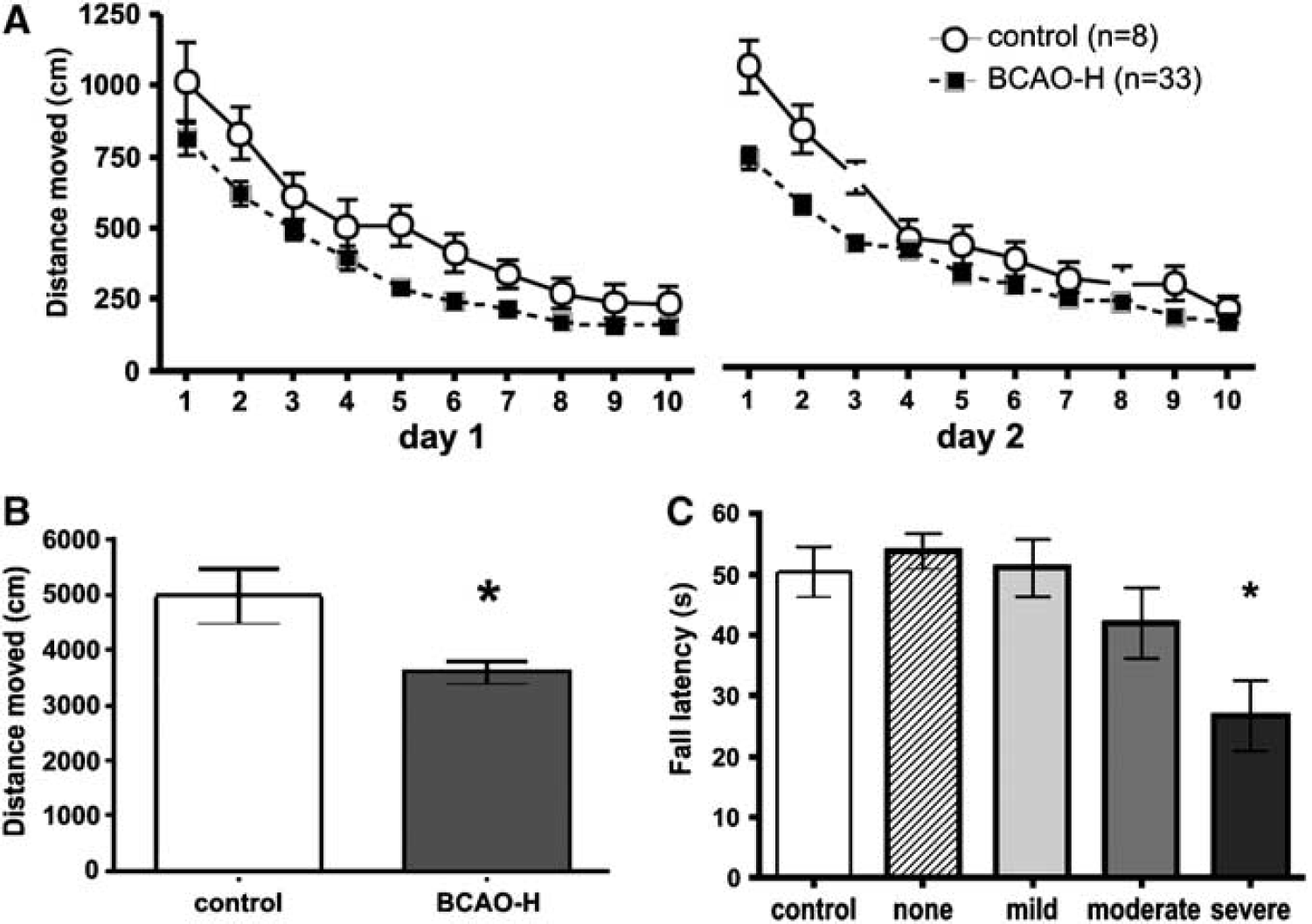
BCAO-H caused activity and sensorimotor coordination deficits. BCAO-H groups moved significantly less than control rats but did not significantly differ from each other. (
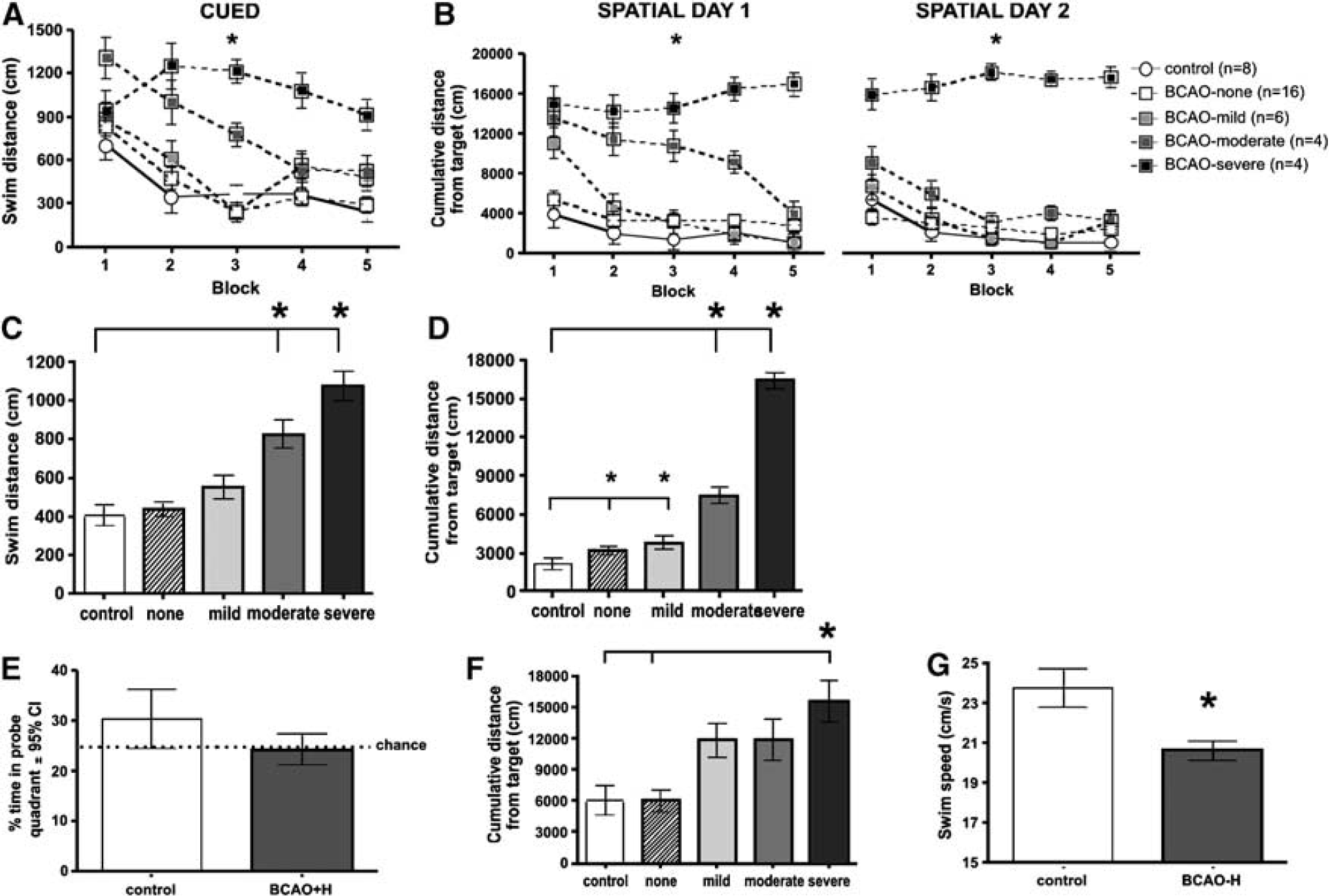
BCAO-H caused water maze performance deficits. (
The overall spatial learning performance of sham and mild BCAO-H rats was similar to control rats but moderate and severe injured rats performed significantly worse (
Water maze probe trials provided a measure of 24-h spatial memory (Figure 5C). Group differences were not significant, and probe trial performance suggests that, for these test parameters, 24 h represents the threshold of spatial memory for control rats.
As the location of the platform is unknown on the first trial of each spatial test day, performance differences on these trials most likely reflect different search strategies. Control sham rats generally found the platform within 60 secs by systematically searching the pool. Severe BCAO-H injured rats performed significantly worse than control and sham rats (
Discussion
The neonatal rodent BCAO-H model produces global hypoxic-ischemia that more closely resembles HIT in the term infant's brain than unilateral occlusion models such as the RVM. The novel findings of this study are (1) bilateral cortical and striatal involvement in neonatal pups with moderate/severe BCAO-H, (2) use of noninvasive imaging to temporally follow the evolution of BCAO-H injury, (3) graded injury subtypes that are essential for future therapeutic investigations, (4) an RPSS that strongly correlates with the volume of injury, and (5) behavioral deficits corresponding to the severity of global injury.
Bilateral Carotid Artery Occlusion and Hypoxia : Comparison to Other Neonatal Models
The RVM has been the standard model for induction of focal HII and is well characterized (Ashwal and Pearce, 2001; Vannucci and Vannucci, 2005). In P7–10 rats, the approximate developmental age of a 32 to 34 week to term human neonate, the common carotid artery is permanently and unilaterally ligated and pups are exposed to hypoxia (90 mins) (Vannucci and Vannucci, 2005). Pups are usually allowed a 90 to 120 mins recovery after surgery before hypoxia induction. The RVM induces only unilateral injury that has been shown to affect cortical and striatal regions (Ashwal et al, 2007). An extension of the RVM can be achieved by bilaterally ligating the common carotid arteries in P4 rat pups, mimicking the clinical condition of periventricular leukomalacia in preterm neonates (Fan et al, 2005; Cai et al, 2006). Bilateral carotid artery occlusion at this age affected neurobehavioral performance at 3 weeks after injury that was worse with increasing hypoxia duration and had bilateral injury similar to that observed in preterm neonates (Barkovich et al, 1995, 1998, 2006; Rutherford et al, 1998; Haataja et al, 2001).
Although an appropriate model for HII in preterm neonates, the P4 BCAO model has limited clinical relevance for term neonates. Clinically, periventricular leukomalacia is observed in preterm neonates, whereas injury to the BG, thalamus, and cortex is most often exhibited in the full-term newborn (Triulzi et al, 2006). The BCAO-H model in the P10 pup induces predominantly gray matter injury (BG and cortex) when there is mild and moderate injury with the addition of hippocampal injury in severely affected animals. This is similar to the diffuse gray matter injury in mild to moderate HII and involvement of thalamus and hippocampus in severe HII in human newborns (Triulzi et al, 2006). With similar injury distributions to that seen clinically in mild, moderate, and severe HII and a scoring system (RPSS) that correlates to the Barkovich and Rutherford scores, we believe the BCAO-H model more accurately represents the clinical condition of HII in human term neonates.
In our model, permanent ligation of both carotid arteries was performed to create a ‘bilateral RVM.’ One question is whether the BCAO-H models chronic hypoperfusion and is thus not truly representative of what occurs clinically (i.e., cerebral blood flow (CBF) may be restored after cardiac function and blood pressure improve). In the RVM, CBF during the period of hypoxia-ischemia ranges between 15% and 41% of control values within the ischemic hemisphere, returns to control values at 30 min, 4 and 24 h after recovery and then at 3 and 6 days decreases again to 23% and 29% of control animals (Vannucci and Vannucci, 1997). This reduction in CBF is attributed to a dramatic reduction in cerebral metabolic rate because of postischemic neurodegeneration as opposed to primary loss of blood flow as a consequence of carotid artery ligation. Two recent papers have examined issues related to changes in CBF after BCAO. A review by Farkas and colleagues revealed that changes in CBF had been studied in adult models between 2.5 h and 6 months after BCAO (without hypoxia) in which the greatest reduction in CBF (35% to 45% of control values) was in cortical and white matter areas (Farkas et al, 2007). These reductions in CBF values start to recover by 1 week but were still lower than control values at 4 weeks. At 6 months after injury, CBF was indistinguishable from controls (Farkas et al, 2007). Choy and colleagues showed that at 6 months after neonatal BCAO, CBF was normal compared with sham animals (Choy et al, 2006). However, there are no published data on CBF in neonatal BCAO animals but RVM data and adult data suggest that blood flow eventually normalizes.
Evolution of Bilateral Carotid Artery Occlusion and Hypoxia Injury
Based on T2WI and DWI, 55.6% of animals exposed to BCAO-H exhibited some form of visible injury on MRI at 24 h. The duration of hypoxia (1 to 15 mins) are significantly shorter than those used in RVM models and the discrepancy is likely because of the reduced oxygen delivery that occurs when CBF is limited by occlusion of both carotid arteries (Uehara et al, 1999; Cai et al, 2001, 2006; Fan et al, 2005). The range of BCAO duration was similar to that reported by Fan et al (2005).
In this study, the duration of hypoxia did not correlate with the severity of injury. There are a number of potential reasons for this surprising finding. We were able to monitor body temperature, but, because of the small size of the rat pups, we were unable to monitor arterial blood pressure, blood glucose, or hematocrit levels. Alterations of these variables could explain the lack of correlation. In addition, 50% of the severe animals died within the first 3 days effectively reducing the power of the correlation. Interestingly, careful review of the literature on adult rodent models of global hypoxia-ischemia found no studies that have addressed the critical issue of developing models of graded injury severity (Ginsberg and Busto, 1989; Traystman, 2003). Thus, we were unable to determine whether there are developmental differences in the range of severity of HII in the adult but not in the rodent pup. If so, this may have important clinical implications in how we manage and assess newborns after HII.
The distribution of injury differed by severity group: mild animals exhibited unilateral cortical involvement, moderate animals exhibited bilateral involvement of the cortex and the striatum that was more extensive in one hemisphere, and severe animals had involvement of nearly all cortical and striatal regions with occasional hippocampal injury. It has been suggested that the first artery ligated would cause more injury in that hemisphere, which might, thereby, explain the asymmetry of injury in our mild and moderate animals. However, this is unlikely in our case because ligation was performed < 5 secs apart and animals had approximately 90 mins to recover before hypoxia. Total injury volume from all experimental animals, as visualized on T2WI, decreased at 28 days as we have reported earlier (Ashwal et al, 2006, 2007).
Comparison of the histologic and MRI results revealed that in the BCAO-H animals there was excellent agreement in cortical and striatal regions at the 28 days time point. Interestingly, the hippocampal neuropathology visible on histology at 28 days was often not seen readily (~50%) with MRI at this time point. DeLaPaz and colleagues reported similar findings in a model of cerebral ischemia in rabbits in which MRI consistently underestimated the extent of ischemic neuronal injury, especially in low-grade histologic changes (DeLaPaz et al, 1991). It is conceivable that slowly progressive neuropathology maybe more difficult to detect by MRI, but mild ischemic changes might be detectable by apparent diffusion coefficient measurements, but this was beyond the scope of our study (DeLaPaz et al, 1991).
Rat Pup Severity Score
We also developed a novel MRI scoring system, the RPSS, for rapid injury assessment. Volumetric analysis is important for injury stratification, with lesion volumes at 2 weeks in adult stroke correlating with motor impairment and reports of health and life satisfaction at 1 year (Saunders et al, 1995; Schiemanck et al, 2005). However, as volumetric analysis is time-consuming and subjective, especially for the diffuse injury patterns seen in clinical cases of HII, we developed a simplified scoring system similar to the Barkovich score that would allow for rapid and objective stratification of injury severity in the rat pup at 24 h after injury.
Clinically, poor neurologic outcomes are associated with MR correlates of cortical highlighting, loss of gray/white differentiation, loss of signal in the posterior limb of the internal capsule, and diffuse injury, as well as involvement of watershed, thalamic, and BG regions (Kuenzle et al, 1994; Rutherford et al, 1996; Barnett et al, 2002). The Barkovich score uses the first-echo T2WI to obtain a BG/watershed score that could predict outcome; patients were given a score of 0 if tissue appeared normal, 1 if there was abnormal signal in BG or thalamus, 2 if there was abnormal signal in the cortex, and 3 or 4 for a combination or increased area of involvement. The RPSS uses a similar numerical score that includes regional (cortical, striatal, and hippocampal) and range of injury (dorsal/ventral, right/left hemisphere) to stratify animals into three severity groups. This score correlated well with the volumetric analysis and had the ability to score an animal in < 1 mins, compared with the >30 mins necessary for volumetric analysis. The RPSS assesses injury severity even when the animal is in the MRI, and could therefore be used for rapid assessment of injury severity. We found excellent correlation between the RPSS and volumetric injury measures.
Behavioral Outcomes
Our findings suggest that even mild unilateral BCAO-H injury detected by MRI at 24 h is associated with learning deficits late in adolescence. Thus, MRI during the acute phase of neonatal brain injury represents a clinically relevant approach to determining the need for further therapeutic intervention.
Global cerebral ischemia in neonatal P10 rats, induced by BCAO-H, produced graded brain lesions that correlated with graded motor and cognitive deficits in adolescent P39 to P51 rats. Overall, BCAO-H rats were hypoactive, exhibiting less activity in an open field test and swimming more slowly in the water maze. Slower swim speed and longer swim distance to find the platform in the water maze task were also exhibited by P10 RVM mice (McAuliffe et al, 2006). Severely BCAO-H injured rats exhibited significant sensorimotor coordination deficits on the rotarod task.
Neonatal BCAO-H induced a number of deficits in water maze performance in adolescence. Subtle differences in spatial learning performance were observed in BCAO-H rats with only minor or no visible brain damage as determined by 24-h MRI. BCAO-H rats with moderate brain damage were significantly impaired on both the cued and spatial tasks, but eventually attained control-like performance on both. BCAO-H rats with severe brain damage never learned either task. Thus, it would appear that mild and moderate BCAO-H animals can learn to compensate for their injuries, whereas severely injured animals do not.
In contrast to our study, BCAO in P4 rat pups (preterm neonate model) resulted in retarded physical development and a host of graded neurobehavioral deficits, including transient hyperactivity, until P21 (weaning age). Damage to both gray and white matter was observed, and 15 mins of hypoxia produced more severe damage than 10 mins (Fan et al, 2005). Furthermore, behavioral tests were only administered up to the age of weaning, whereas we waited until adolescence to assess behavior. Interestingly, a study using P7 RVM mice assessed similar behaviors (water maze, open field, rotarod) at similar ages (7 and 9 weeks after injury) to our study and observed similar behavioral deficits (reduced open field activity and graded rotarod and water maze deficits) (Ten et al, 2004).
As the cued water maze required swimming to a visually salient escape platform in a pool of water, differences in cued performance exhibited by the BCAO-H moderate and severe rats most likely involve sensorimotor deficits (e.g., vision, swimming ability), impaired simple/general learning ability, and/or motivational differences. Our findings indicate that moderate and severely injured rats were highly impaired on the spatial task. As finding a submerged platform is much more difficult than finding a visible platform, these deficits are not surprising. Of greater interest is the finding that sham and mild BCAO-H rats were impaired on the spatial, but not cued, tasks. Generally, this pattern of performance would suggest the presence of ‘true’ spatial learning deficits. However, it is possible that the sham and mild deficits may simply represent subtle manifestations of the sensorimotor, motivational, and general learning and strategic deficits observed in the moderate and severe groups.
In summary, the BCAO-H model represents a clinically relevant model of global hypoxic-ischemia in the term neonate and produces variable degrees of brain injury that correlate with later cognitive and motor deficits. Similarly, the MR observed distribution of injury is similar to those seen clinically. The results of this and other studies (Sie et al, 2005; Haku et al, 2006) suggest that MRI can be used during the early phases of hypoxic-ischemia to predict later brain damage and behavioral deficits. Future studies will attempt to identify the factors that lead to gradation of injury, the areas of the brain associated with eventual motor versus cognitive deficits, and therapeutic agents that can prevent or reduce the behavioral sequelae associated with neonatal HII.