
Abstract
Intrathecally, triamcinolone acetonide (TCA) was suggested to have neuroprotective efficacy on infarction volume in acute focal cerebral ischemia in rats. In the first dose-finding study, TCA in five different doses or saline was administered into the cisterna magna of 12 rats, each 30 mins after endovascular occlusion of the middle cerebral artery (MCAO). In the second magnet resonance controlled confirmation study, the most neuroprotective dose was compared with controls in each of the 15 rats. Infarction volume was calculated at 24 h by 2.3.5 triphenyl-tetrazolium-chloride staining. Compared with controls (18.2%), infarction volume was significantly reduced using TCA at a dose of 0.012 mg/kg body weight (BW) (13.4%, P=0.04). TCA at doses of 0.03 (17.7%, P=0.84), 0.006 (15.9%, P=0.24), and 0.003 mg/kg BW (14.5%, P=0.11) did not significantly reduce infarction size. TCA 0.3 mg/kg BW resulted in bilateral infarction with increased infarction volume (19.8%, P=0.49). Magnetic resonance imaging confirmed successful MCAO and intrathecal administration. In experiment 2 compared with controls (20.0%), infarction volume was significantly reduced using TCA 0.012 mg/kg (13.4%, P=0.02). Intrathecally, TCA may significantly reduce infarction volume in acute focal cerebral ischemia in rats. Further studies are necessary to define the value of this therapy.
Introduction
Ischemic stroke is a leading cause of death and long-term disability, but its management remains a challenge. Aggressive therapies, such as thrombolysis, decompressive craniectomy, and hypothermia, aim to restore blood flow and reduce post-ischemic brain edema. They have been shown to be beneficial in selected patients (The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group, 1995; Schwab et al, 1998).
For a medical approach, various classes of pharmacological neuroprotective agents have been studied for the treatment of acute ischemic stroke. Despite promising results in the experimental setting, only a few have reached clinically controlled trials, mainly without being able to show a clinical benefit (Broderick and Hacke, 2002; Ginsberg, 2009).
Glucocorticoids, clinically widely established for numerous indications, primarily act as membrane stabilizers, antioxidants, and anti-inflammatory agents (Abraham et al, 2001). They are used empirically to reduce inflammation and edema in the clinical setting, for example, after brain injury and in multiple sclerosis (Hoffmann et al, 2003; Rhodes, 2003). Interestingly, there are a few experimental and clinical studies available on the effects of glucocorticoids in acute cerebral ischemia reporting controversial results (Abraham et al, 2001; Akdemir et al, 2005; Bertorelli et al, 1998; de Courten-Myers et al, 1994; Koide et al, 1986; Lapchak et al, 2000; Limbourg et al, 2002; Norris and Hachinski, 1986; Patten et al, 1972; Slivka and Murphy, 2001; Tuor et al, 1993).
Theoretically, intrathecal corticoid administration might bypass the systemic side effects and simultaneously decrease brain edema and intracranial pressure. A functionally compromised but viable brain may thus be able to survive.
This study was designed to evaluate the effects of intrathecally administered steroid triamcinolone acetonide (TCA) on infarction volume in a rat model of acute focal permanent cerebral ischemia.
Materials and methods
The study was approved by the Institutional Review Board. Male Wistar rats weighing 250 to 350 g were used in this study. Food and water were provided freely before and after surgery.
Animal Preparation
Anesthesia was induced by inhalative isoflurane and maintained by intramuscular injection of ketamine 10% and xylazine 2% (7:3) at a dose of 0.1 ml/100 g body weight (BW). Circulation parameters were monitored continuously during animal preparation. In experiment 2, additional blood glucose was measured with glucose oxidase reagent strips (Accu-Chek Sensor, Roche Diagnostik GmbH, Mannheim, Germany) using a drop of venous blood preoperatively, immediately before, and 2 and 24 h after TCA application.
Focal cerebral ischemia was introduced using an intraluminal suture occlusion model of the middle cerebral artery (MCAO) (Longa et al, 1989). Briefly, the external carotid artery was ligated, the internal carotid artery was isolated, and the pterygopalatine artery was ligated. A 4-0 monofilament nylon suture, whose tip was coated with silicone, was introduced transvascularly through an arteriotomy into the common carotid artery and gently advanced through the internal carotid artery to the origin of the middle cerebral artery, thus occluding its origin.
Study Design
Experiment 1:
Seventy-two rats were randomly allocated to six treatment groups of 12 animals each. Intrathecal administration was performed with different doses of TCA: 0.3, 0.03, 0.012, 0.006, or 0.003 mg/kg BW, respectively, whereas the control group received equivolumetric saline.
Experiment 2:
To confirm the impact of the most effective dose of experiment 1 (0.012 mg/kg BW) and to exclude possible sources of error as failed MCAO and/or failed intrathecal injection, a second magnetic resonance imaging (MRI)-controlled study was performed. Animals were randomly assigned to 2 groups of 15 animals each. The treatment group received TCA 0.012 mg/kg BW intrathecally, whereas the control group received equivolumetric saline. To confirm successful MCAO and intrathecal drug administration, diffusion-weighted and T1-weighted MRI were performed. Contrast agent (0.14 μl/100 g BW gadolinium-diethylenetriamine-penta-acetic-acid, Magnevist, Schering AG, Berlin, Germany) was added to the drug administered to visualize intrathecal injection in T1-weighted MRI.
Intrathecal Drug Administration
Triamcinolone acetonide (VolonA, Bristol-Meyers Squibb, New York, NY, USA, active ingredient 16α.17-Dimethyl-methylendioxy-9-fluor-11β.21-dihydroxy-1.4-pregnadien-3.20-dion) supplied in sodium chloride solution equivalent to 40 mg TCA/ml was used in this study. Intrathecal drug administration was performed 30 mins after MCAO as a single middle suboccipital injection of 0.075 ml/kg BW volume of either TCA preparation or saline into the cisterna magna, performed slowly using a 23G needle with the animals still under anesthesia.
Solutions for experiment 1 were prepared as follows: 1 ml VolonA and 9, 99, 249, 499, and 999 ml saline, respectively. For the control group, only saline was administered. Solutions of experiment 2 were prepared as follows: 4 ml of solution 1 (1 ml VolonA and 249 ml saline) and 1 ml of solution 2 (1 ml 500 mmol gadolinium-diethylenetriamine-penta-acetic-acid and 10 ml saline). In this way, all animals of experiment 2 received 0.75 μmol/kg BW gadolinium-diethylenetriamine-penta-acetic-acid in addition to that received in experiment 1. For the control group, 4 ml saline and 1 ml of solution 2 were mixed.
Determination of Infarction Size
Twenty-four hours after MCAO, animals were killed, their brains rapidly removed, and the 2 mm coronal brain slices incubated for 30 mins in a 4% solution of 2.3.5 triphenyltetrazolium-chloride (TTC) at 37°C and fixed by immersion in 4.5% buffered formalin solution. Brain slices were photographed from both sides, and the area of infarction was quantified using IMAGE 1.41 (NIH, Bethesda, MD, USA) by an observer masked to the animals' experimental group. As the total brain volume in the different treatment groups varied because of the different BW at baseline, we calculated the relative infarction volumes expressed as a percent of the total brain volume. The average percent infarction volume was calculated for each group.
Magnetic Resonance Imaging
Magnetic resonance imaging was performed within 2 h of MCAO on a 1.5T whole-body MR imager (Siemens Sonata, Erlangen, Germany). Anesthesia was maintained. A standard body coil was used for radiofrequency transmission; the signal was detected with a temporomandibular joint surface coil (Ø = 9 cm). Multislice coronal T1-weighted spin-echo images (TR = 300 ms, TE = 14 ms, matrix 256 × 256, field of view = 40 × 40 cm, slice thickness = 2 mm) and diffusion-weighted spin-echo EPI images (TR = 2000 ms, TE = 77 ms, matrix 128 × 128, field of view = 93 × 93 cm, slice thickness = 2 mm) were acquired with the middle slice positioned at the level of the optic chiasm. Animals without successful intrathecal injection and/or no infarction were replaced.
Data Analysis
For statistical analysis of all results, commercial software (Analyse-it for Excel, General and Clinical Laboratory statistics, Version 1.68, Analyse-it Software Ltd, Leeds, UK) was used. Infarction volumes were described by an analysis of variance. All values were expressed as mean ± s.d.
Results
Physiological Parameters
No significant differences between treatment groups for any of the physiological parameters monitored were noted. Anesthesia, surgery, and infarction resulted in a similar temporary increase in blood glucose concentration in the control and treatment groups of experiment 2.
Mortality
Experiment 1:
After the intrathecal injection, none of the animals of the 0.006 and 0.003 mg/kg BW, two animals (16.7%) of the 0.3 mg/kg BW, three (25.0%) of the 0.03 mg/kg BW animals, and one (8.3%) of the 0.012 mg/kg BW group died. Two animals in the control group died (16.7%).
Experiment 2:
Two of 15 animals in the control group (13.3%) and none of the animals in the TCA group died.
Infarction Volume
Experiment 1:
Compared with controls (18.2 ± 5.0%), infarction volume was significantly reduced with a dose of 0.012 mg TCA/kg BW (13.4 ± 5.3%, P = 0.04), representing a 26.4% reduction in infarction size. TCA with a dose of 0.3 mg/kg BW resulted in bilateral infarction (Figure 1) with slightly increased infarction volume (19.8 ± 5.0%, P = 0.49), given as total infarction volume in proportion of the right hemisphere. Compared with controls, intrathecal administration of TCA in doses of 0.03, 0.006, and 0.003 mg/kg BW reduced infarction size; however, this finding was not significant (17.7 ± 6.9%, P = 0.84; 15.9 ± 4.2%, P = 0.24; 14.5 ± 5.2%, P = 0.11).
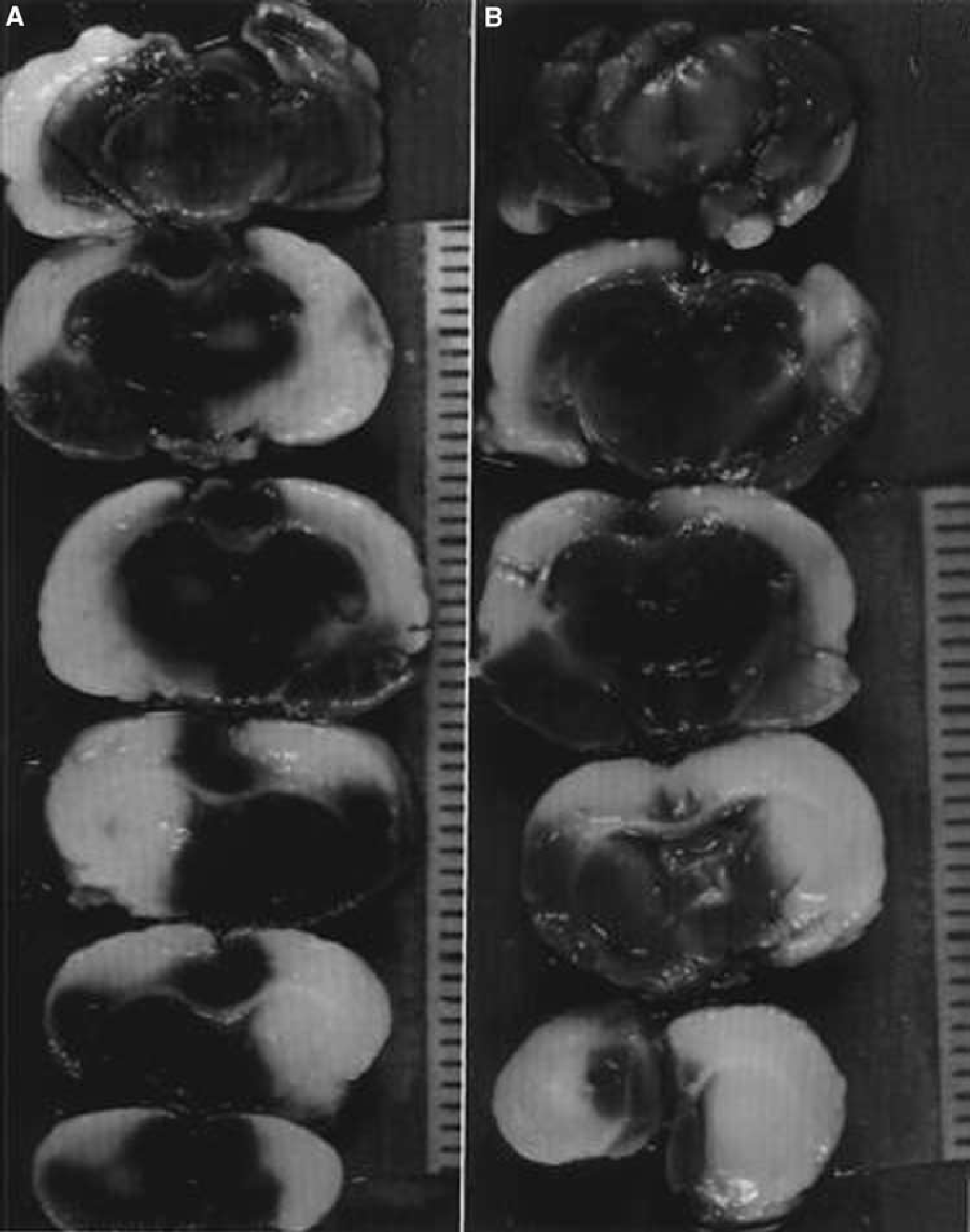
2.3.5 triphenyl-tetrazolium-chloride staining after administration of 0.3 mg/kg body weight triamcinolone acetonide. Note the bilateral infarctions in both animals (
Experiment 2:
In MRI, one animal of the control group showed no infarction. In two animals of the treatment group and one animal of the control group, no successful intrathecal administration could be achieved. These animals were replaced. All evaluated animals had successful intrathecal administration in T1-weighted MRI (Figure 2) and successful MCAO in diffusion-weighted MRI. Compared with controls, infarction volume was significantly reduced in animals treated with TCA 0.012 mg/kg BW (13.4 ± 6.5% versus 20.0 ± 8.0%, P = 0.02), representing a 32.9% reduction in infarction size (Figure 3).
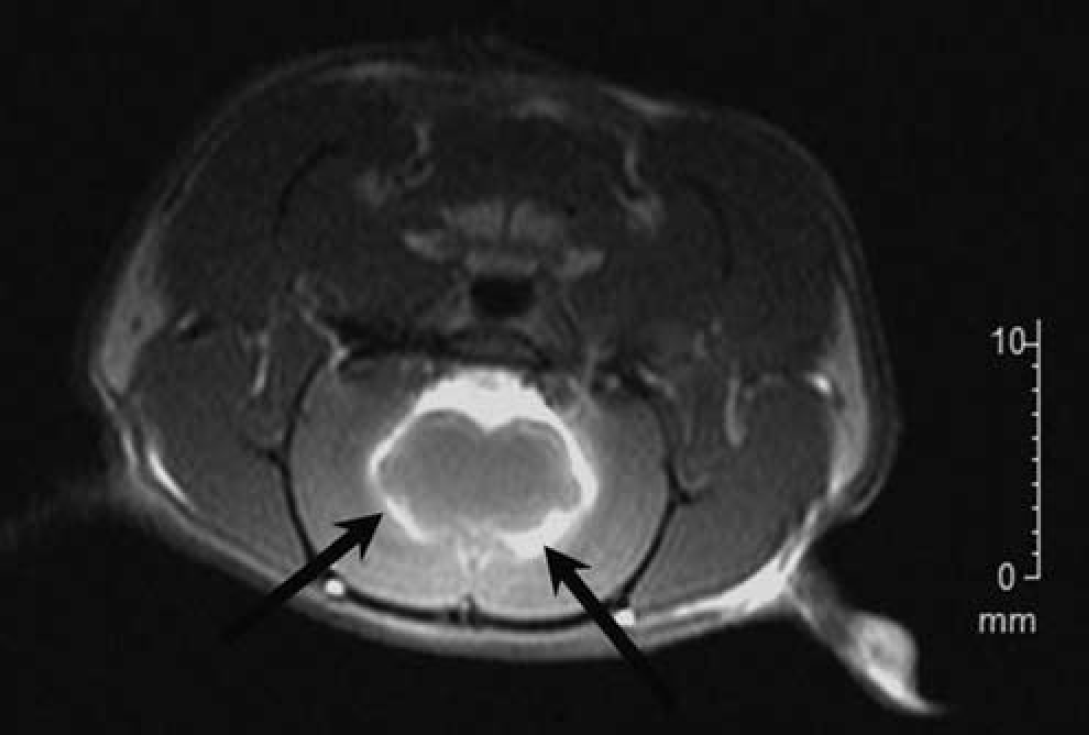
T1-weighted magnetic resonance imaging, coronal view, showing successful intrathecal administration (arrows).
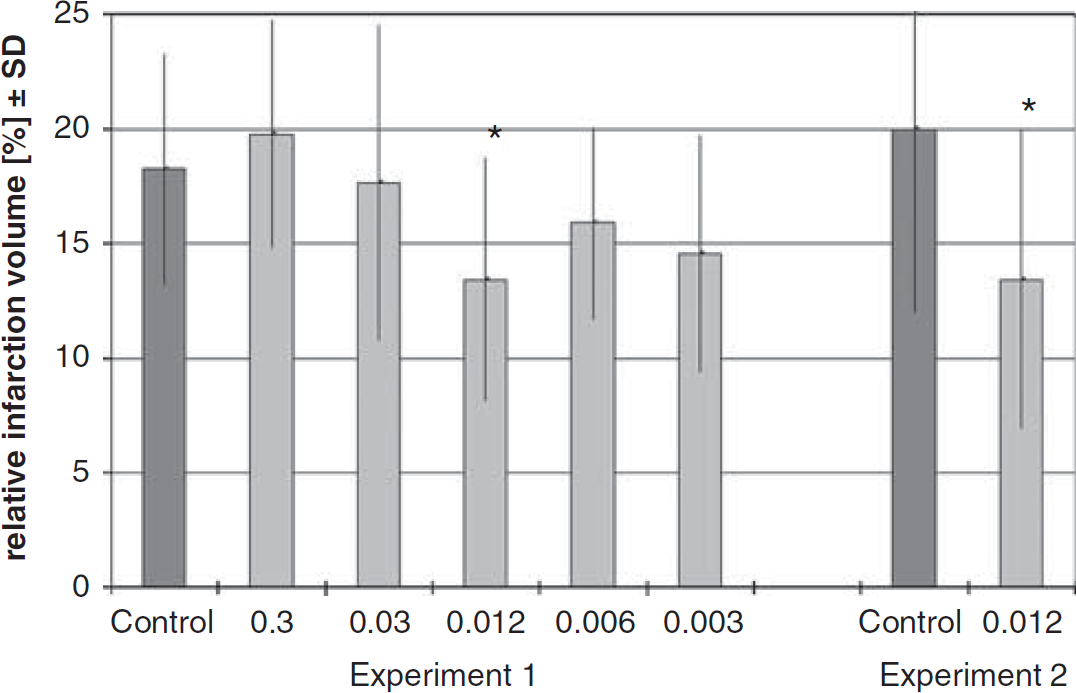
Relative infarction volumes of experiments 1 and 2. *Significant reduction in infarction volume compared with control (P < 0.05).
Discussion
Reducing post-ischemic edema and intracranial pressure, thus preserving collaterals, is one main goal in the acute management of large cerebral infarcts. Post-ischemic brain edema has two components: the early cytotoxic, intracellular edema caused by failure of the ion pumps, starting within minutes after onset of ischemia, and the vasogenic, extracellular edema mainly attributed to an impaired blood–brain barrier, peaking after 3 to 5 days (Ayata and Ropper, 2002). Corticoids are thought to ameliorate the pathophysiological processes in various brain lesions by reducing the associated brain edema and intracranial pressure (Betz and Coester, 1990). The possible mechanisms discussed are membrane stabilization, improved cerebral blood flow, limitation of inflammatory processes, and reduction of blood–brain barrier permeability to large molecules (Ziylan et al, 1988). Comparable mechanisms are discussed in the successful application of glucocorticoids in a rodent model of heart ischemia (Tokudome et al, 2009).
In a study of experimental focal cerebral ischemia in rats, Slivka and Murphy (2001) found that the methylprednisolone concentration in the infarcted right hemisphere reached only 61% of the concentration in the normal left hemisphere. Considering that the concentration in the infarcted tissue and immediately adjacent brain after intraarterial application was very low, we chose the intrathecal route of drug administration to bypass the impaired blood supply in infarcted tissues and to avoid the negative systemic effects of glucocorticoids. Akdemir et al (2005) found comparable neuroprotective effects after intraventricular glucocorticoids in a model of temporary global cerebral ischemia in rats. Our method of intrathecal injection without need of trepanation seems to be more convenient in daily practice.
Experiment 1 was performed as a dose-finding study. Intrathecal administration of TCA 0.012 mg/kg BW turned out to be most effective with a significant reduction in infarction size compared with controls. In contrast, intrathecal administration of TCA 0.3 mg/kg BW resulted in ‘toxic effects’ with a rather increased infarction volume in the right hemisphere plus infarction extending to the left hemisphere, a phenomenon we had never observed while working with this animal model for nearly two decades. Preliminary testing in a small number of healthy non-ischemic rats with intrathecal administration of high doses of TCA (up to 0.5 mg/kg BW) and gadolinium-diethylenetriamine-penta-acetic-acid (up to 4.4 μmol/kg BW) did not show any alterations on TTC images 24 h after administration. To confirm the neuroprotective findings, we performed a second MR-controlled experiment with TCA at a dose of 0.012 mg/kg BW. T1-weighted and diffusion-weighted images were acquired to eliminate possible sources of error such as failed MCAO and/or intrathecal injection. Experiment 2 confirmed the findings of experiment 1, with a significant reduction in infarction size compared with controls.
Corticosteroids as neuroprotective agents administered systemically have been evaluated in a few experimental and clinical studies in cerebral ischemia with heterogeneous results. This may reflect differences in ischemia duration, agents, dosing regimes, route of administration, and outcome measurements (Akdemir et al, 2005; Bertorelli et al, 1998; de Courten-Myers et al, 1994; Koide et al, 1986; Lapchak et al, 2000; Slivka and Murphy, 2001; Tuor et al, 1993).
We observed beneficial effects of TCA with a significant reduction in infarction size at a dose of 0.012 mg/kg BW and slight but nonsignificant reduction of infarction size with TCA 0.03, 0.006, or 0.003 mg/kg BW. Our results are consistent with previous studies reporting a reduction in infarction size after corticoid administration in focal cerebral ischemia (Akdemir et al, 2005; Bertorelli et al, 1998; de Courten-Myers et al, 1994; Limbourg et al, 2002; Slivka and Murphy, 2001; Tuor et al, 1993). Aview of the literature reveals the heterogeneous effects of glucocorticoids in stroke, reflecting the heterogeneous features involved in neurodegenerative and neuroprotective processes (Abraham et al, 2001).
Akdemir et al (2005) found neuroprotective properties of cyclosporine A and methylprednisolone administered intraventricularly in a global temporary ischemia within reperfusion after 30 mins. Using a model of permanent cerebral ischemia in rats, Bertorelli et al (1998) showed dexamethasone administered intraperitoneally 10 mins after infarction onset to decrease infarction size by up to 50%. de Courten-Myers et al (1994) showed administration of intravenous methylprednisolone at high doses 30 mins after onset of cerebral ischemia to significantly reduce infarction volume and cerebral blood flow drop in cats surviving 4 days. In a double-blind, randomized, controlled patient trial, high-dose dexamethasone administered within 48 h after onset of stroke resulted in no significant difference in outcome. However, the authors stated that steroid administration might prevent death in patients harboring massive infarcts (Norris and Hachinski, 1986). In other studies, administration of glucocorticoids resulted in no or even detrimental effects on infarction size (Koide et al, 1986; Slivka and Murphy, 2001). Koide et al (1986) found that glucocorticoids administered intraperitoneally did not improve (acute pretreatment and post-treatment) but even aggravated (long-term pretreatment) infarction size in transient focal forebrain ischemia in rats. High-dose methylprednisolone decreased infarction volume after temporary, but not permanent, focal ischemia in rats (Slivka and Murphy, 2001).
Clinically, elevation of blood glucose levels by systemic, particularly long-term glucocorticoids is reported to be detrimental and is associated with increased short- and long-term mortality in acute cerebral ischemia (Gilmore and Stead, 2006; Kagansky et al, 2001; Williams et al, 2002). In animal models, the results are less consistent (Dietrich et al, 1993). In our study, blood glucose levels stayed within normal values. We found a physiological intraoperative increase in blood glucose values in all animals, with no further increase after corticoid injection and normalization more than 24 h.
In malignant brain tumors, the corticoid-induced decrease in perifocal edema and subsequent intracranial pressure is mainly based on stabilization of tight junctions (Skjoeth and Bjerre, 1997). The hypothetical effect of steroids on acute cerebral ischemic edema might be partially comparable with the impact seen in malignant brain tumors.
Corticosteroids administered intraperitoneally and administered within 2 h of transient cerebral ischemia in mice increased endothelial nitric oxide synthase activity, leading to nitric oxide-dependent vasodilatation, with an increase in regional cerebral blood flow by up to 50%, and reduction of infarction size by 32% (Limbourg et al, 2002). Cytokines have an important role in infarct development. The production of tumor necrosis factor-α, interleukin-1β, and interleukin-6 was decreased under dexamethasone treatment for pulmonary disease (Bessler et al, 1999). The anti-inflammatory potential of corticoids might be an additional mechanism in the reduction of infarction size.
Owing to the known high mortality of hemispheric middle cerebral artery infarction within the first 3 days because of massive brain swelling and subsequent herniation, we confined our experimental protocol to 24 h after vessel occlusion and did not attempt longer survival periods. Accordingly, survival was not long enough to allow significant inflammatory response (Danton and Dietrich, 2003). Furthermore, the relatively short survival period may not assess final infarction volume. It could be argued that we simply postponed the development of ischemic brain damage and that the final infarction size might be unaffected. Therefore, further studies focusing on long-term effects and clinical outcome are necessary to validate the therapeutic value, which are already planned as part two of the recent study design.
However, even if intrathecal TCA only delays the onset of permanent neuronal damage, it may well increase the therapeutic benefit of other therapies such as additional pharmacological neuroprotection, reperfusion, or craniectomy or at least expand their time window, particularly because experimental studies suggested that a combination of therapies is more effective than each of them alone (Culmsee et al, 2004).
There are some limitations when trying to extrapolate our results to the clinical situation. The time course of cerebral ischemia in rats is different from that in humans, and the quality of leptomeningeal collateral blood flow also differs substantially. TCA distribution might depend on diffusion effects. Rat brain has a great surface in relation to its size, and the agent has not to diffuse as deep as it would have to in human brains. A neuroprotective effect only on the surface could be possible. Deeper, moreover not collateralized, infarcted areas may not benefit from intrathecal TCA in humans. Studies in infarction models with greater brains would be informative.
We found a significant reduction in infarct volume of 30% on average with TCA 0.012 mg/kg BW administered intrathecally 30 mins after MCAO in rats. Intrathecal drug administration might improve the access of the drug to underperfused brain tissue, permit a lower dose of glucocorticoids to be effective, and eliminate the systemic side effects. Intrathecally administered TCA may act as an early secondary prevention to limit the further evolution of cerebral ischemia.
Future studies focusing on intrathecal drug administration at later time points, refined formulas and stroke models, and combined therapies are needed.
Footnotes
Acknowledgements
This study contains excerpts from the doctoral thesis of Sophia L Goericke. This study was awarded with the prize for medicine 2008 endowed by the Sparkasse bank of Essen, Germany, and remunerated with 5000€.
The authors declare no conflict of interest.