
Abstract
This review considers the pathobiology of non-impact blast-induced neurotrauma (BINT). The pathobiology of traumatic brain injury (TBI) has been historically studied in experimental models mimicking features seen in the civilian population. These brain injuries are characterized by primary damage to both gray and white matter and subsequent evolution of secondary pathogenic events at the cellular, biochemical, and molecular levels, which collectively mediate widespread neurodegeneration. An emerging field of research addresses brain injuries related to the military, in particular blast-induced brain injuries. What is clear from the effort to date is that the pathobiology of military TBIs, particularly BINT, has characteristics not seen in other types of brain injury, despite similar secondary injury cascades. The pathobiology of primary BINT is extremely complex. It comprises systemic, local, and cerebral responses interacting and often occurring in parallel. Activation of the autonomous nervous system, sudden pressure-increase in vital organs such as lungs and liver, and activation of neuroendocrine-immune system are among the most important mechanisms significantly contributing to molecular changes and cascading injury mechanisms in the brain.
Introduction
In this review, we focus on blast-induced neurotrauma (BINT), including mechanisms underlying brain damage and challenges imposed by this complex injury from both clinical and experimental perspectives. Whereas we do not consider the broader topic of traumatic brain injuries (TBIs) in the civilian population, there are a number of reviews from the past 5 years that consider this topic in detail, particularly from the perspectives of animal models (Cernak, 2005; Kazanis, 2005; LaPlaca et al, 2007; Manvelyan, 2006; Morales et al, 2005; Potts et al, 2009; Weber, 2007), and the understanding that we have gained from these models with regard to general pathobiology (Bramlett and Dietrich, 2007; Park et al, 2008; Povlishock and Katz, 2005; Werner and Engelhard, 2007), mechanisms of cell injury (Bayir and Kagan, 2008; Mazzeo et al, 2009; Raghupathi, 2004; Robertson, 2004; Sullivan et al, 2005; Yakovlev and Faden, 2004; Zhang et al, 2005), posttraumatic epilepsy (D'Ambrosio and Perucca, 2004; Dichter, 2009; Garga and Lowenstein, 2006; Pitkanen and McIntosh, 2006; Pitkanen et al, 2009; Willmore and Ueda, 2009), axonal injury (Bales et al, 2009; Buki and Povlishock, 2006; Hurley et al, 2004), behavior (Fujimoto et al, 2004; Schallert, 2006), proteomics (Ottens et al, 2007), biomarkers (Kochanek et al, 2008; Kovesdi et al, 2009), and neuroprotection (Bales et al, 2009; Beauchamp et al, 2008; Byrnes et al, 2009; Cook et al, 2009; Dichter, 2009; Dietrich et al, 2009; Forsyth et al, 2006; Gibson et al, 2008; Jain, 2008; Jennings et al, 2008; Kokiko and Hamm, 2007; Mammis et al, 2009; Margulies and Hicks, 2009; Marklund et al, 2006; Mechoulam and Shohami, 2007; Rogers and Wagner, 2006; Schouten, 2007; Schumacher et al, 2007; Stein, 2008; Stoica et al, 2009; Vink and Nimmo, 2009; Wang et al, 2006; Wise et al, 2005; Xiong et al, 2009).
TBIs caused by explosion
Throughout Operation Enduring Freedom and Operation Iraqi Freedom, explosive devices have become more powerful, their detonation systems more creative, and their additives more devastating. According to the Department of Defense ‘Personnel & Procurement Statistics’, over 73% of all US military casualties in Operation Enduring Freedom and Operation Iraqi Freedom are caused by explosive weaponry (Defense Manpower Data Center, 2008). As of January 2008 (Congressional Research Service, 2008), the Department of Defense reported that over 5,500 soldiers had suffered traumatic brain injuries. As a continuing threat to our troops, blast injury, especially BINT, has been called the signature wound of the war in Iraq (Elder and Cristian, 2009). Civilians are also frequent victims of explosive devices such as landmines and unexploded ordnance (Bilukha et al, 2008), or explosive weaponry used in terrorist incidents (Center for Terrorism and Intelligence Studies, 2009). Indeed, terrorists increasingly use suicidal–homicidal bombers who deliberately accompany the explosive device, often wearing it, to ensure maximal harm. The bombers drive or walk into buses, subways, residential areas, shopping malls, and government buildings. In both civilian and military environments, exposure to a blast may cause instant death, injuries with immediate manifestation of symptoms, or latent injuries, which may manifest over and/or after an extended period after the initial blast exposure (Ling et al, 2009). Due to the complexity of injurious environment as well as of the resulting injuries, there is a need for prospective, longitudinal studies to confirm reports of long-term effects of exposure to blasts.
Protection from blast injuries presents several challenges. Although body armor protects the torso from shrapnel and projectiles, it may intensify the blast wave effect in two ways (Courtney and Courtney, 2009). First, body armor constitutes an improved contact surface for shock-front–body interaction and energy transfer; second, it may also serve as a reflecting surface that concentrates the power of an explosion as the blast wave resonates internally (Phillips et al, 1988). The improved interceptive properties of body armors have increased the survival rate of soldiers by protecting them from penetrating injuries. In parallel with the increased survival rate, however, the rate of severe, debilitating, long-term consequences has also increased (Martin et al, 2008). There are differing findings and anecdotal information about the influence of body armor on the blast load inside the organism. For example, Phillips et al (1988) reported generally higher intrathoracic pressure in sheep protected with cloth ballistic vests. He hypothesized that the ‘likely mechanisms of injury enhancement include an increase in the target surface area and an alteration of the effective loading function on the thorax’. Conversely, Long reported significant reduction of brain pathology for rats protected with soft ‘body armor’ comparable to the cloth ballistic vest protection used by Phillips. There are also opinions that the influence of body armor on the blast energy transfer into the body, thus potential development of blast-induced neurological deficits, depends on the type of the body armor, that is, soft (cloth without interceptive plate) versus hard (with interceptive plate). The lack of sound knowledge of the effects of different types of body armor on non-impact, blast-induced brain damage necessitates well-designed and orchestrated experimental and clinical studies.
Besides being acutely injured, soldiers serving in theater and some military professionals during their daily activity or training are also subjected to repeated low-level blast exposure. The cumulative effects of the exposures could lead to serious short-term and long-term health impairments (Richmond et al, 1981). For those without body armor, the effects of blast are more deadly and the whole spectrum of blast injuries is expected (Champion et al, 2009; Ling et al, 2009). Apart from the injuries caused by blast overpressure (primary blast effects), these soldiers have increased potential for penetrating injuries from shrapnel and other debris (secondary blast effects), and for acceleration and deceleration of the body and head (tertiary blast effects) (Figure 1).
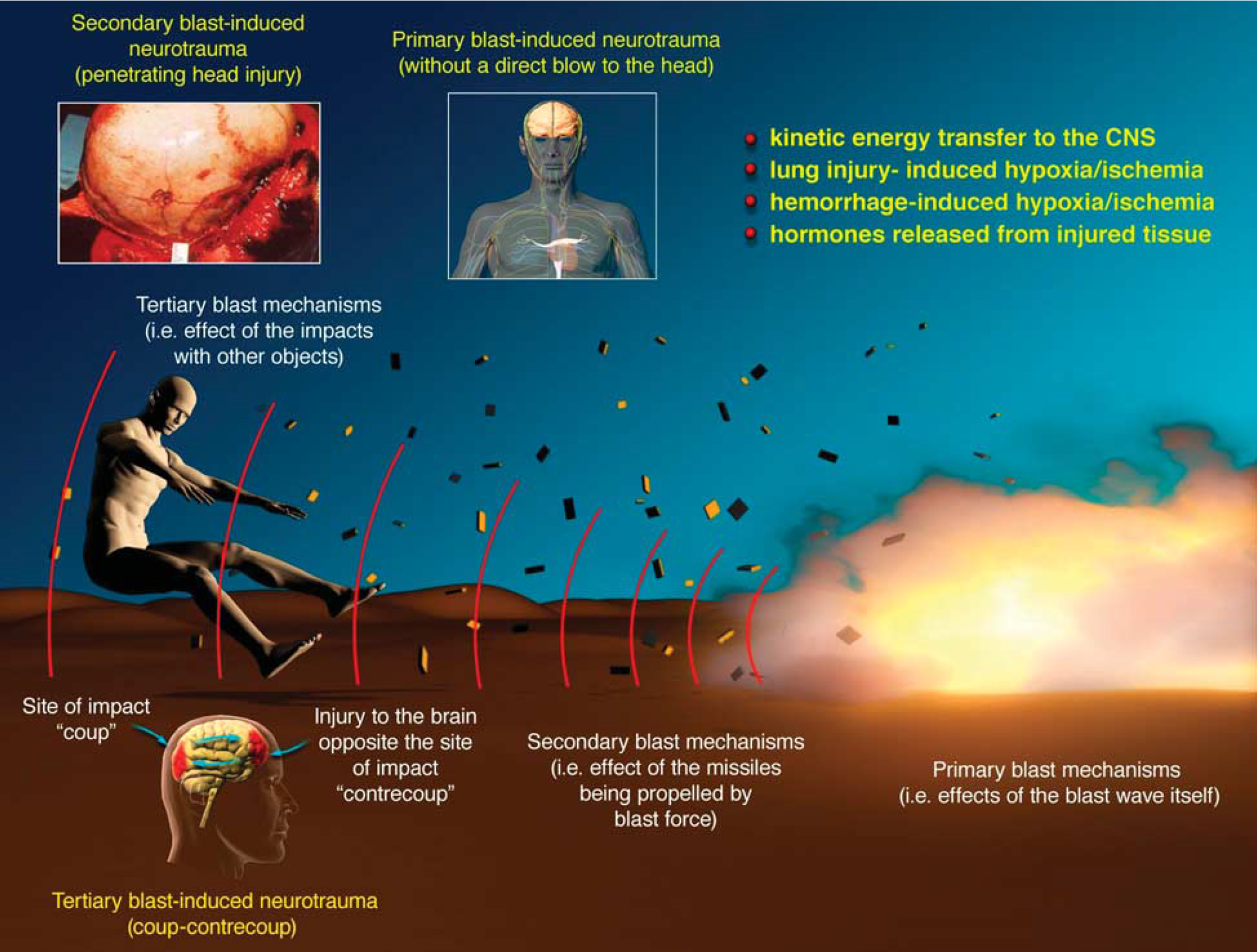
Complex injurious environment because of blast: primary blast effects, that is, effects of the blast wave itself (primary blast injury); secondary blast effects caused by particles propelled by blast-force (secondary, that is, penetrating blast) injury; and tertiary blast effects caused by acceleration and deceleration of the body and its impact with other objects (tertiary blast injury similar to ‘coup–countercoup’).
Basic mechanisms of explosive injuries
A blast wave generated by an explosion starts with a single pulse of increased air pressure that lasts a few milliseconds. The negative pressure or suction of the blast wave follows the positive wave immediately (Owen-Smith, 1981). The duration of the blast wave—that is, the time that an object in the path of the shock wave is subjected to the pressure effects—depends on the type of explosive and the distance from the point of detonation (Clemedson, 1956). The blast wave progresses from the source of the explosion as a sphere of compressed and rapidly expanding gases, which displaces an equal volume of air at high velocity (Rossle, 1950). The velocity of the blast wave in air may be extremely high, depending on the type and amount of explosive used. The blast wave is the main determinant of primary blast injury and consists of the front of high pressure that compresses the surrounding air and falls rapidly to negative pressure. It travels faster than sound and in few milliseconds damages the surrounding structures. The blast wind following the wave is generated by mass displacement of air by expanding gases; it may accelerate to hurricane proportions and is responsible for disintegration, evisceration, and traumatic amputation of body parts. Thus, a person exposed to an explosion will be subjected not only to a blast wave but also to the high-velocity wind traveling directly behind the shock front of the blast wave (Rossle, 1950). Compared with a hurricane-force wind that travels about 200km/h and exerts an overpressure of only 1.72 kPa (0.25 psi), a lethal blast-induced overpressure of 690 kPa (100 psi) travels at about 2,414 km/h (Owen-Smith, 1981).
The magnitude of damage from the blast wave depends on five factors: (1) the peak of the initial positive-pressure wave (an overpressure of 690 to 1,724 kPa, for example, 100 to 250 psi, is considered potentially lethal) (Champion et al, 2009); (2) the duration of overpressure; (3) the medium of explosion; (4) the distance from the incident blast wave; and (5) the degree of focusing because of a confined area or walls. For example, explosions near or within hard solid surfaces become amplified two to nine times because of shockwave reflection (Rice and Heck, 2000). Moreover, victims positioned between a blast and a building often suffer from injuries two to three times the degree of injury of a person in an open space. Indeed, people exposed to explosion rarely experience the idealized pressure-wave form, known as the Friedländer wave. Even in open-field conditions, the blast wave reflects from the ground, generating reflective waves that interact with the primary wave and, thus, changing its characteristics. In a closed environment (such as a building, an urban setting, or a vehicle), the blast wave interacts with the surrounding structures and creates multiple wave reflections, which, interacting with the primary wave and between each other, generate a complex wave (Ben-Dor et al, 2001; Mainiero and Sapko, 1996). Previous attempts to define the mechanisms of blast injury suggested the involvement of spalling, implosion, and inertial effects as major physical components of the blast–body interaction and later tissue damage (Benzinger, 1950). Spallation is the disruption that occurs at the boundary between two media of different densities; it occurs when a compression wave in the denser medium is reflected at the interface. Implosion occurs when the shockwave compresses a gas bubble in a liquid medium, raising the pressure in the bubble much higher than the shock pressure; as the pressure wave passes, the bubbles can re-expand explosively and damage surrounding tissue (Benzinger, 1950; Chiffelle, 1966; Phillips, 1986). Inertial effects occur at the interface of the different densities: the lighter object will be accelerated more than the heavier one, so there will be a large stress at the boundary. Recent results suggest a frequency dependence of the blast effects: high-frequency (0.5–1.5 kHz) low-amplitude stress waves target mostly organs that contain abrupt density changes from one medium to another (for example, the air-blood interface in the lungs or the blood–parenchyma interface in the brain), and low-frequency (<0.5 kHz) high-amplitude shear waves disrupt tissue by generating local motions that overcome natural tissue elasticity (Cooper et al, 1991; Gorbunov et al, 2004) (for example, at the contact of gray and white brain matter).
Thus, explosions may cause four major patterns of injury: (1) primary blast injury caused by the blast wave itself; (2) secondary injury caused by the fragments of debris propelled by the explosion; (3) tertiary injury because of the acceleration of the body or part of the body by the blast wind; and (4) flash burns because of the transient, but intense, heat of the explosion (Mellor, 1988). Moreover, the current state-of-the-science suggests that the extent and types of primary blast-induced injuries depend not only on the peak of the overpressure but also on other characteristics, such as the number of overpressure peaks, the lag time and shear fronts between overpressure peaks, their frequency resonance, and electromagnetic pulse generated from the blast.
The complexity of BINT
Potential mechanisms by which blasts cause brain injury include: (1) direct interaction with the head through direct passage of the blast wave through the skull and/or causing acceleration and/or rotation of the head and (2) transfer of kinetic energy from the blast wave through large blood vessels in the abdomen and chest to the central nervous system (Courtney and Courtney, 2009); namely, as the front of the blast overpressure interacts with the body surface and compresses the abdomen and chest, it transfers its kinetic energy to the body's fluid phase. The resulting hydraulic interaction initiates oscillating waves that traverse the body at about the speed of sound in water and deliver the kinetic energy of the blast wave to the brain. Once delivered, that kinetic energy causes both morphological and functional damage to distinct brain structures (Cernak et al, 1999). The two potential ways of interaction do not exclude each other (Bauman et al, 2009). Most recent experimental data suggest both the importance of the blast's direct interaction with the head (Saljo et al, 2008), and the role of shockwave-induced vascular load (Long et al, 2009a) in the pathogenesis of BINT.
Due to the complexity of the injurious environment, that is, multiple blast effects that interact with the body parallel, BINT represents a unique clinical entity caused by interwoven mechanisms of systemic, local, and cerebral responses to blast exposure (Cernak et al, 1991; Cernak et al, 1996a; Figure 2). Whereas mild BINT, in general, is induced by primary blast, moderate to severe brain injuries because of blast are part of a polytrauma and caused by simultaneously acting primary, secondary, tertiary, and sometimes even quaternary effects of the blast.
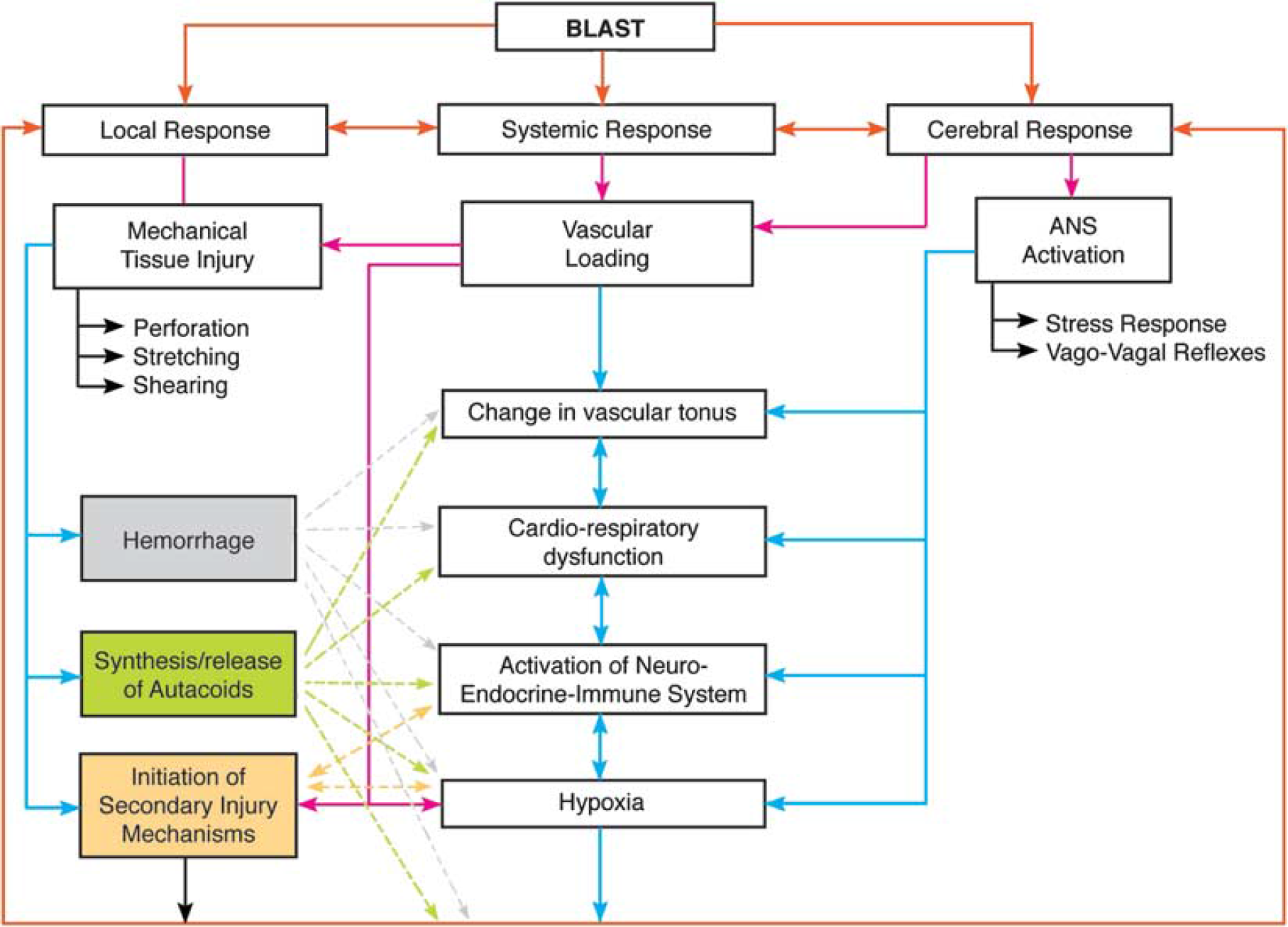
Simultaneous activation of systemic, local, and cerebral responses to blast exposure, and interactive mechanisms causing or contributing to the pathobiology of BINT.
In general, primary blast injuries are characterized by absence of external injuries and potential par-enchymal damage, mostly of the lungs (Rossle, 1950; Chiffelle, 1966); thus, internal injuries are often unrecognized and their severity underestimated (Dedushkin et al, 1992). It was hypothesized (Cernak et al, 1996a; Zuckerman, 1940) that blast overpressure may cause sudden hyperinflation of the lungs and subsequent mechanical irritation of juxtacapillary J-receptors located in the alveolar interstitium and innervated by vagal fibers (Paintal, 1969). The stimulation of the J-receptors causes a vago-vagal reflex leading to apnea followed by rapid breathing, bradycardia, and hypotension, which are frequently observed immediate symptoms after blast exposure. Additionally, chemoreceptors located primarily in the left ventricle can be stimulated by hypoxia/ischemia caused by pulmonary vagal reflex, and subsequently trigger a cardiovascular decompressor Bezold–Jarish reflex, which involves marked increase in vagal (parasympathetic) efferent discharge to the heart (Zucker, 1986). This causes reduction of heart rate (bradycardia) and dilatation of the peripheral blood vessels with resulting lowering of the blood pressure, which could further contribute to cerebral hypoxemia (Cernak et al, 1996a). The importance of vagally mediated cerebral effects has been supported by experiments using rabbits (Cernak et al, 1996a) or rats (Irwin et al, 1999) subjected to blast. Bilateral vagotomy has been shown to mitigate bradycardia, hypotension, and apnea (Cernak et al, 1996a; Irwin et al, 1999). It has also been demonstrated that vagotomy prevented excessive metabolic alterations, but did not eliminate other damaging mechanisms (such as oxidative stress, for example) (Cernak et al, 1996a). Clinical experience shows the importance of vagal influence and brainstem involvement in long-term neurological sequels of TBI (Haig et al, 1996; Kox et al, 2008). Conversely, recent studies show beneficial effects of vagus nerve stimulation in reducing TBI-induced cerebral edema (Clough et al, 2007) or improving motor and cognitive function after injury (Smith et al, 2005). Although currently existing knowledge suggests that blast exposure can cause direct brainstem injury/dysfunction, further studies are necessary to identify all underlying mechanisms.
Blast-induced mechanical tissue injury of peripheral soft tissue and/or internal organs because of perforation, stretching, and/or shearing can lead to hemorrhage and synthesis and release of autacoids, which, when released in systemic circulation, activate the neuroendocrine-immune system and contribute to initiation of secondary brain injury mechanisms (Bhattacharjee, 2008; Cernak et al, 1991; Cernak et al, 1996a).
Experimental challenges of BINT
There is limited available scientific knowledge about the pathobiology of BINT. Moreover, the existing literature is often contradictory, with a broad range of experimental animals and models being used. The purpose of experimental models of TBI is to replicate certain pathological components or phases of clinical trauma in experimental animals aiming to address pathology and/or treatment. The design and choice of a specific model should emulate the goal of research (Cernak, 2005). For example, characterization of basic molecular and gene injury mechanisms that are conserved through evolution may use phylogenetically lower species such as lissencephalic rodents, whereas establishing the pathogenesis of impaired higher brain functions would require larger animals with a gyrencephalic brain. Regardless of the research questions to be addressed, clinically and militarily relevant BINT models should satisfy the following criteria: (1) the injurious component of the blast should be clearly identified and reproduced in controlled, reproducible, and quantifiable manner; (2) the inflicted injury should be reproducible, quantifiable, and mimic components of human BINT; (3) the injury outcome established based on morphological, physiological, biochemical, and/or behavioral parameters should be related to the chosen injurious component of the blast; and (4) the mechanical properties (intensity, complexity of blast signature, and/or its duration) of the injurious factor should predict the outcome severity. Unfortunately, because of lack of well-defined criteria for reliable animal models of BINT, the current experimental models used in an attempt to study BINT vary widely, including classical direct impact TBI models such as controlled cortical impact and fluid percussion injury models, air-gun-type compressed air-delivered impact model, shock and blast tube models, and open-field explosion experiments, among others. The lack of understanding of the physics of blast, unfocused rationale of experiments, and the broad variety of methods used to inflict head injury in the context of BINT research makes the comparison of the experimental results extremely challenging.
Experimental studies on primary blast-induced biological effects routinely use either shock tubes (which use compressed air or gas to generate a shockwave) or blast tubes (which use explosive charges to generate a shockwave) (Nishida, 2001; Robey, 2001). Anesthetized animals are fixed individually in special holders designed to prevent any movement of their bodies in response to blast and, thus, to prevent tertiary effects of the shock or blast wave (Wang et al, 1998). Most shock and blast tubes used in current experimental models replicate the ideal blast wave from an open-air explosion, without the capability to generate a non-ideal blast wave with multiple shock and expansion fronts as seen in real-life conditions, thus limiting the extent of comparability of experimental and clinical findings. A small number of studies use open-field exposure of animals to a blast wave generated by detonation of an explosive (Axelsson et al, 2000; Cernak et al, 1991; Richmond, 1991; Saljo and Hamberger, 2004). Although such an experimental setting is more comparable with in-theater conditions, the physical characteristics (such as homogeneity of the blast wave) are less controllable, so a broader range of biologic response should be expected. A wide range of blast overpressure sustained for various durations has been used in single-exposure experimental studies. In most studies, the animals were subjected to a shock or blast wave with a mean peak overpressure of 52–340 kPa (7.54–49.31 psi) on the nearest surface of an animal's body (Cernak et al, 2001a; Chavko et al, 2007; Clemedson et al, 1969; Saljo et al, 2000). Most experiments used rodents (mice and rats) (Cernak et al, 2001a; Long et al, 2009a), but some have subjected rabbits (Cernak et al, 1997), sheep (Cernak et al, 1991), pigs (Bauman et al, 2009), or non-human primates to blast (Bogo et al, 1971; Damon et al, 1968; Richmond et al, 1967; Table 1).
A summary of major articles and models of BINT
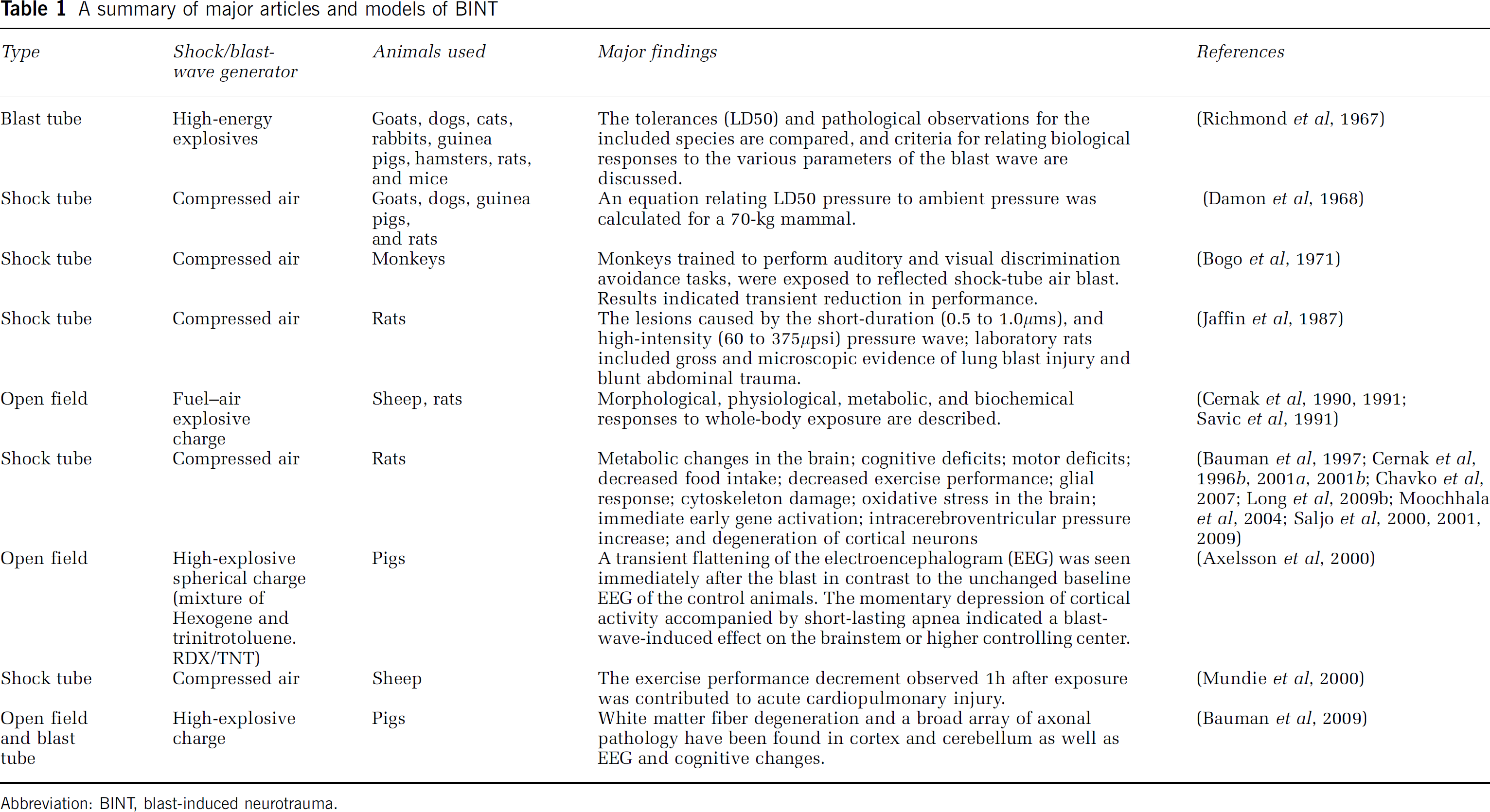
Abbreviation: BINT, blast-induced neurotrauma.
Primary BINT
A number of behavioral, physiological, biochemical, and pathological changes occur as a result of exposure to primary blast in various animal and human studies. Considerable reductions in food intake and exercise performance have been found in rats exposed to low-intensity shockwaves (83 or 1,129 kPa) (Bauman et al, 1997). Similar findings have been reported for sheep (Mundie et al, 2000).
Vasospasm has been identified as a particularly common complication in patients with moderate or severe BINT (Armonda et al, 2006; Ling et al, 2009). The blast-induced vasospasm can develop early, often within 48 h of injury; it can also manifest later, typically between 10 and 14 days after exposure. Interestingly, the emergence of vasospasm has also been demonstrated in experiments with pigs fitted with armor and exposed to a relatively mild-intensity (172.67/25 psi) blast in the blast tube (Bauman et al, 2009).
Rats exposed to different charges of a plastic explosive (pentaerythritol tetranitrate), intended to generate a blast wave of 220 or 350 kPa (32 or 51 psi) in a blast tube, demonstrated significant decreases in amplitude and frequency of the brain's electric activity measured with electroencephalography (EEG) continuously during 30 min after the blast (Risling et al, 2002). Those changes were more profound in rats exposed to 350 kPa (51 psi) or in those exposed repeatedly to 220 kPa (32 psi). Similarly, transient flattening of the EEG was seen in pigs immediately after an explosive blast that generated a free-field waveform with a peak of approximately 241 kPa (35 psi), in contrast to the unchanged baseline EEG in control animals. Momentary depression of cortical activity accompanied by brief apnea indicates a blast-wave-induced effect on the brain-stem or on higher controlling center (Axelsson et al, 2000). Disruption of the EEG waveforms have been found in pigs in which the head, but not the whole body, was inserted into an explosive-driven blast tube and exposed to an approximately 413-kPa (60 psi) blast (Bauman et al, 2009). Dose-dependent increase in intracranial pressure and inverse relationship between the level of blast and the time of the intracranial pressure onset have been found in rats exposed to low-intensity (10, 30, or 60 kPa, for example, 1.45, 4.35, or 8.7 psi) blast (Saljo et al, 2008). Increased intraparenchymal pressure in the brain has been also observed in pigs exposed to approximately 413 kPa (60psi) (Bauman et al, 2009).
Rhesus monkeys exposed to approximately 207 kPa (30 psi), 276 kPa (40 psi), or 345 kPa (50 psi) had significant, albeit transient, memory and performance deficits (Bogo et al, 1971). Considerable and persistent memory deficits have been shown for rats subjected to moderate- and low-intensity blast waves generated in an air-driven shock tube (Cernak et al, 2001a; Long et al, 2009a; Saljo et al, 2008). Neurological dysfunction had been demonstrated also in pigs exposed to open-field blast (Bauman et al, 2009).
Blast exposure has been reported to cause brain edema and considerable metabolic disturbances in the brain: significantly decreased glucose, magnesium, and ATP concentrations; increased lactate concentration and lactate:pyruvate ratio (Cernak et al, 1996a); as well as impaired function of the Na+, K +, ATPase pump (Cernak et al, 1997). Those changes clearly suggest energy failure or imbalance between energy demand and available energy, shift of glucose metabolism from the aerobic toward the anaerobic pathway, and impairment in neuronal cell membrane permeability. Swelling of neurons, an astroglial response, and myelin debris in the hippocampus have been found after moderate blast injury in animals (Cernak et al, 2001a). Immunohistochemical analyses have shown significant damage to the neuronal cytoskeleton in layers II to IV of the temporal cortex, in the cingulate gyrus and the pirifom cortex, in the dentate gyrus, and in the CA1 region of the hippocampus over 7 days after blast exposure (Saljo et al, 2000). White matter fiber degeneration and a broad array of axonal pathology have been found in the cortex and cerebellum of pigs exposed to 379 kPa (55 psi) or 538 kPa (78 psi), respectively (Bauman et al, 2009).
Oxidative stress, changes in antioxidant–enzyme defense systems (Cernak et al, 2001a), and later cognitive deficits (Cernak et al, 2001a) have also been seen. Nitric oxide production in the brain structures of rats exposed to 339 kPa (49 psi) shockwave was determined by measuring the total nitrite/nitrate concentration, and by the expression of inducible nitric oxide synthase mRNA (Cernak et al, 2001b). The results showed significant elevation of total nitrite/nitrate levels comparable with the changes in the expression of inducible nitric oxide synthase and reduction in cognitive performance. Activation of glial fibrillary acidic protein, an indicator of astrocytosis, was evident in the hippocampus of rats 21 days after a single exposure to a 234 kPa (34 psi) burst of overpressure (Saljo et al, 2001). Astrocytosis has also been shown in the cortex and dentate gyrus of pigs exposed to a peak overpressure of 276 kPa (40 psi) (Bauman et al, 2009).
Studies of the effects of repeated low-level (29–62 kPa, for example, 4.2–9 psi) blast exposures demonstrated accumulating pathological alterations involving multiple organs or organ systems (Elsayed and Gorbunov, 2007; Yang et al, 1996), with activation of the hypothalamic–pituitary–adrenal axis and significant biochemical and hormonal changes in the brain (Mazurkiewicz-Kwilecki, 1980). Moreover, repeated exposures to low-intensity (20 kPa, for example, 2.9 psi) blast caused significant motor and cognitive deficits as well as degeneration of cortical neurons in rats (Moochhala et al, 2004).
BINT versus civilian TBIs: parallels and differences
Recently Margulies and co-workers (Margulies and Hicks, 2009) reviewed the early pathobiological events that accompany TBI, based on experimental models that mimic diffuse and focal TBIs. It is clear that many of the features seen in these animal models likewise accompany BINT, including vasospasm and barrier disruption, EEG abnormalities, oxidative stress, and elevated intracranial pressure, metabolic disturbances, and energy failure (Table 2). Although some studies suggest different temporal and spatial profiles or frequency of pathological changes (for example, vasospasm) in BINT compared with TBI induced by injurious factors other than explosion (Armonda et al, 2006; Ling et al, 2009), other reports emphasize the lack of strong evidence that blast is categorically different from other TBI mechanisms, at least with regard to cognitive sequelae (Belanger et al, 2009). Thus, further experimental and clinical studies are required to identify injury mechanisms generalizable for both BINT and civilian TBI, as well as those specific for BINT.
A comparison of the general features seen within the first 24 h in experimental models that mimic civilian TBIs, as recently reviewed by Margulies
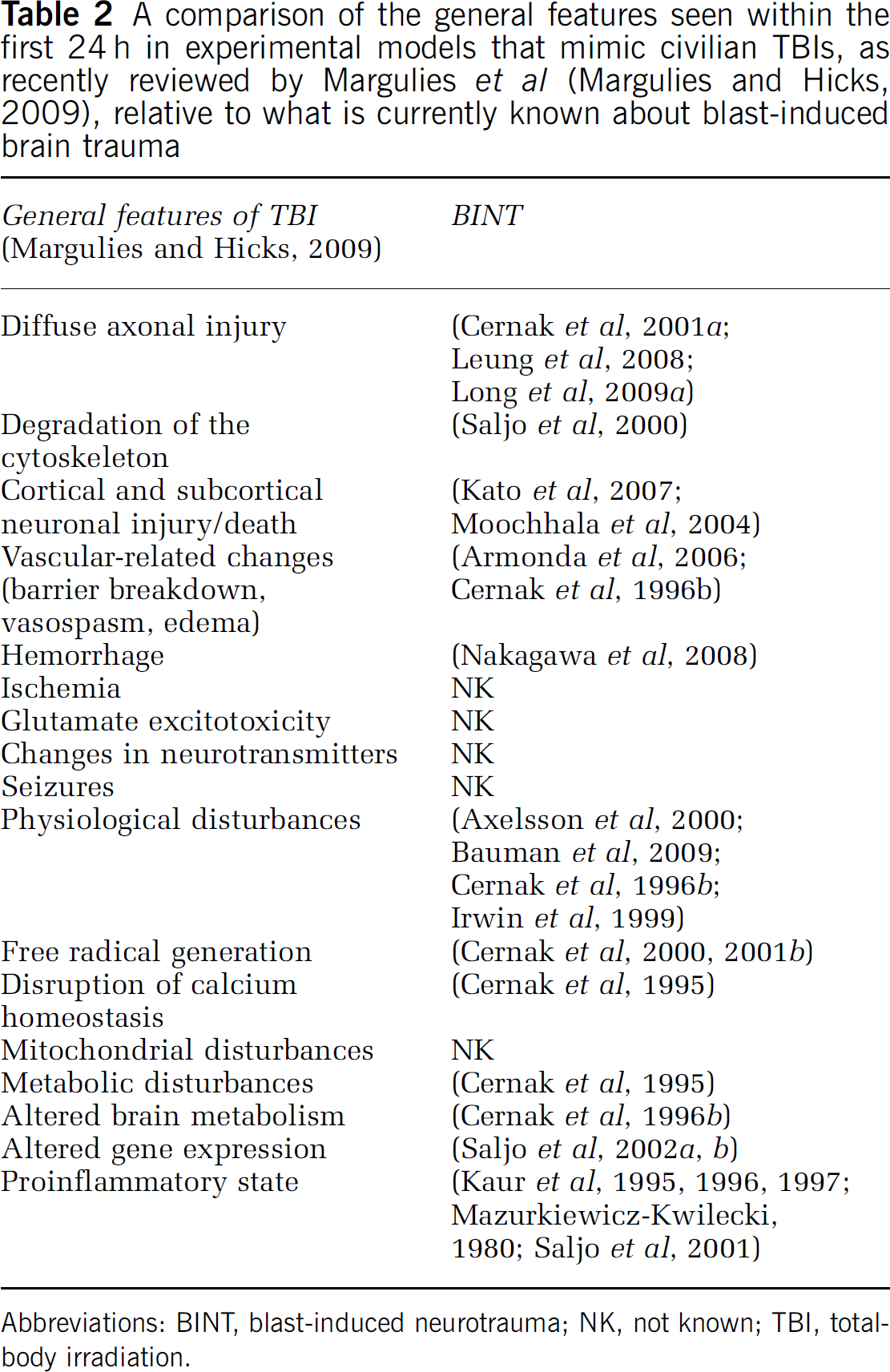
Abbreviations: BINT, blast-induced neurotrauma; NK, not known; TBI, total-body irradiation.
Conclusions
The problem of BINT and related long-term neurological deficits has been gradually increasing with the progress of military warfare, and the pathological experience of returning veterans of Operation Enduring Freedom/Operation Iraqi Freedom has triggered more intensified attention of researchers toward clarifying the vital mechanisms underlying blast-induced brain damage. Nevertheless, because of the lack of understanding of the complex injurious environment generated by an explosion, and deficient knowledge of shockwave physics among medical researchers, the currently available literature is contradictory and often misleading. There is an obvious need for a well-coordinated, multidisciplinary research approach to clarify injury tolerance levels; to develop reliable, militarily, and clinically relevant experimental models; and to define the injury mechanisms underlying acute and chronic consequences of blast exposure(s). These challenging tasks can only be achieved with a unified front of physicists, military scientists, biomedical researchers, and clinicians applying out-of-the-box thinking and novel research approaches.
Footnotes
Acknowledgements
This work was supported by a contract from the US Department of Veterans Affairs to the National Academy of Sciences, Institute of Medicine, and NIH/NINDS NS050159.