
Abstract
Sildenafil (Viagra®), a cyclic guanosine monophosphate-degrading phosphodiesterase 5 inhibitor, induces headache and migraine. Such headache induction may be caused by an increased neuronal excitability, as no concurrent effect on cerebral arteries is found. In 13 healthy females (23±3 years, 70.3±6.6 kg), the effect of sildenafil on a visual (reversing checkerboard) and a hypercapnic (6% CO2 inhalation) response was evaluated using functional magnetic resonance imaging (fMRI, 3 T MR scanner). On separate occasions, visual-evoked potential (VEP) measurements (latency (P100) and maximal amplitude) were performed. The measurements were applied at baseline and at both 1 and 2 h after ingestion of 100mg of sildenafil. Blood pressure, heart rate and side effects, including headache, were obtained. Headache was induced in all but one subject on both study days. Sildenafil did not affect VEP amplitude or latency (P100). The fMRI response to visual stimulation or hypercapnia was unchanged by sildenafil. In conclusion, sildenafil induces mild headache without potentiating a neuronal or local cerebrovascular visual response or a global cerebrovascular hypercapnic response. The implication is that sildenafil-induced headache does not include a general lowering of threshold for a neuronal or cerebrovascular response, and that sildenafil does not modulate the hypercapnic response in healthy subjects.
Introduction
Sildenafil (Viagra®) is a selective inhibitor of the cyclic guanosine monophosphate (cGMP) hydrolysing phosphodiesterase 5 enzyme (PDE5). Its primary clinical use is in the treatment of erectile dysfunction (Rosen and Kostis, 2003) and pulmonary hypertension (Michelakis et al, 2003). It has been suggested recently for use in pre-eclampsia (Turgut et al, 2008). Sildenafil induces headache and migraine without immediate changes in cerebral blood flow (CBF) or cerebral artery diameter (Kruuse et al, 2003, 2002). This is in contrast to other headache and migraine-inducing compounds, all of which induce an immediate vasodilator response and immediate mild headache, as well as a delayed headache resembling a genuine migraine attack (Lassen et al, 2002; Thomsen et al, 1994).
Sildenafil prolongs the intracellular clearance of the second messenger, cGMP, and was, therefore, proposed to increase the neuronal excitability (Hoheisel et al, 2005) or a local cerebrovascular response (Rosengarten et al, 2006) to external stimuli. Intracellular cyclic nucleotide levels are regulated by production, degradation and efflux. In this equilibrium, PDEs are the enzymes responsible for degradation and, hence, modulation of the cyclic nucleotide involved signalling (Bender and Beavo, 2006).
The pathophysiology of migraine is not fully understood, but may involve nitric oxide (NO)–cGMP signalling in the neuronal and vascular compartments of the brain (Olesen, 2008). An altered modulation of sensory signals from the trigeminal sensory afferents or a primary brain stem or thalamic dysfunction (Goadsby, 2007), as well as a cortical hyperexcitability, including cortical spreading depression (Pietrobon and Striessnig, 2003), is suggested to be involved in headache mechanisms. We hypothesised that sildenafil may elicit a headache by generally increasing either the excitability of neurons or the cerebrovascular response to external stimuli, or both.
The effect of sildenafil on the response to external stimuli was tested by measuring visual response to checkerboard stimulation in healthy subjects before and after sildenafil administration. The visual response was evaluated using blood oxygen level-dependent (BOLD) imaging and visual-evoked potential (VEP) recordings. The visual system was chosen because earlier neurophysiological studies in migraine patients had shown altered responses to visual stimulations (Cao et al, 2002; Sand et al, 2008; Schoenen et al, 2003). Furthermore, one of the principal accompanying symptoms of migraine is photophobia and, in a subset of patients, migraine can be triggered by visual stimulation concomitant to increased activity in brain stem structures and visual cortex (Cao et al, 2002).
In addition, the possible potentiating effect of sildenafil on the hypercapnic BOLD response was investigated because the vascular response to CO2 may also involve cGMP (Pelligrino et al, 1993; Scheckenbach et al, 2006).
Thus, sildenafil administration and modulation of cGMP breakdown might increase the response to these external stimuli and give rise to an increased or prolonged cerebral response to visual stimulation and hypercapnia. The BOLD response represents the cerebrovascular local and global response, and could be affected by both neuronal and vascular effects, whereas VEP would be affected only by the neuronal effects of sildenafil.
Materials and methods
The study was approved by the Ethical Committee of Copenhagen County KA05069.
Inclusion criteria were female gender, a normal medical examination, no history of migraine, > 4 days of tension-type headache in a month and no first-degree relatives with migraine. Further criteria were right-handedness and normal vision. No medication except contraceptives was allowed.
The subjects were investigated on 2 days at least 1 week apart, when either functional magnetic resonance imaging (fMRI) or VEP investigations were performed. The order of VEP and fMRI investigations was balanced within the group. Investigations were not performed within 5 days before or after the start of menstruation. Placebo was not used because sildenafil caused flushing as a side effect; thus, blinding was not possible, especially during the VEP investigations. As a control, the fMRI and VEP investigations were repeated before the study in four subjects using a similar set-up but without medication.
For both VEP and fMRI measurements, the subjects arrived in the morning, headache free, after 12 h fasting. After 30 mins of rest in the supine position for fMRI, baseline measurements were performed followed by the administration of oral sildenafil of 100 mg. Visual-evoked potential and fMRI measurements were performed at baseline and at both 1 and 2 h after the ingestion of sildenafil. Blood pressure and heart rate were measured every 30 mins.
Functional Magnetic Resonance Imaging Procedure
Visual stimulation was presented with the Eloquence system (Invivo, Orlando, FL, USA), using rear projection from an LCD (liquid crystal display) screen. A fibre optic cable connected the system to a control computer outside the scanner room. The paradigm consisted of rest blocks, where a uniform grey image was shown, alternating with active blocks displaying a black and white quadratic checkerboard reversing at 8 Hz. Starting with a rest block, each block lasted for 45 secs, with six blocks in total. Subjects were asked to fixate on a central fixation cross during the entire scan. The onset of visual stimuli was triggered by the scan acquisition.
For CO2 stimulation, a nose clip was applied and the subject breathed through a plastic mouthpiece connected to a tube. During the three rest blocks, the subjects breathed normal air; and during the two active blocks, the tube was attached to a gas line delivering 6% CO2-enriched air. The block length was 3 mins. The end-tidal CO2 (ETCO2) was monitored and recorded every 10 secs using a capnograph (Datex, Helsinki, Finland).
Functional Magnetic Resonance Imaging Data Acquisition
Magnetic resonance imaging was performed on a 3.0T Philips Intera Achieva scanner (Philips Medical Systems, Best, The Netherlands) using an eight-element phased-array receive head coil. Anatomic images were acquired using a T1-weighted three-dimensional turbo field-echo sequence (170 sagittal slices of 1mm thickness; in-plane resolution 1 × 1mm; repetition time 9.9 secs; echo time 4.6 msecs; and flip angle 8°). Functional imaging used a gradient-echo and echo planar imaging sequence (32 slices of 4.0mm thickness; slice gap 0.1mm; field of view 230 × 230mm; in-plane acquired resolution 2.9 × 2.9mm; repetition time 3.0 secs; echo time 35 msecs; flip angle 90°; and SENSE (SENSitivity Encoding) factor 2). The slices were oriented along a line from the glabella to the posterior part of the foramen magnum. The first four volumes of each run were discarded to avoid saturation effects. For the visual and CO2 stimulation, 90 and 300 volumes were obtained, respectively.
Functional Magnetic Resonance Imaging Data Analysis
A full analysis was performed using BrainVoyager 1.9 (Brain Innovation B.V., Maastricht, The Netherlands). Image pre-processing started with a three-dimensional rigid-body motion correction. After three-dimensional spatial smoothing with a 6-mm full-width at half-maximum Gaussian kernel, the functional images were coregistered to the three-dimensional anatomies, transformed into the Talairach space and re-sampled to isotropic 3mm voxels. A general linear model was used for statistical analysis. The visual block stimulation paradigm convolved with a two-γ haemodynamic response function served as a model time course. For the CO2 stimulation, the measured ETCO2 curve in units of kPa and interpolated to the repetition time of 3.0 secs was used as predictor. In both cases, the time courses of the six motion-correction parameters were added as predictors of no interest in the design matrix. In a second-level analysis of the β-values, a one-way analysis of variance with regard to scan time (before and both 1 and 2 h after ingestion of sildenafil) was computed. The F-test statistic was calculated both voxel-wise and for regions of interest. Subject-specific regions of interest for either stimulation type were defined by joining activated regions at each scan time. The activated regions were determined by requiring P > 0.02 corrected for multiple comparisons using the false discovery rate. For visual stimulation, the activated region was required to be geometrically connected to the primary visual cortex.
The average response curves for visual and CO2 stimulation using the above-defined regions of interest were also computed.
Visual-Evoked Potentials
A visual paradigm similar to that used during fMRI was chosen to correlate the responses. Visual-evoked potentials were recorded during a pattern-reversal stimulation using a black and white quadratic checkerboard with 9mm pattern, 24 × 32 checkers reversing at 2Hz (Keypoint, Alpine Medico Aps, Skovlunde, Denmark). Subjects were placed in a chair 1m in front of the computer screen and instructed to fixate on a central small red cross. Each eye was stimulated with the other covered. Measurement of the P100 latency and maximal amplitude was performed.
Circulation
Blood pressure and heart rate were measured using a noninvasive blood pressure device (Dinamap XL Vital Signs Monitor, Kivex, Hoersholm, Denmark). Both measures were obtained at baseline and every 30 mins until 2 h after dose. Furthermore, continuous heart rate and electrocardiogram were monitored using the pulse oximeter finger clip and the electrocardiogram electrodes supplied with the magnetic resonance scanner.
Headache
Headache intensity was scored on a verbal scale from 0 to 10, where 1 represents a very mild headache (including a feeling of pressing or throbbing), 5, a headache of moderate intensity and 10, the worst possible headache (Iversen et al, 1989). Headache characteristics, location, side effects and intake of medication were recorded. All subjects continued these recordings every hour at home for 12 h after drug administration. The total amount of headache induced was assessed by calculating the time-weighted integral (‘area under the curve‘) of the scores obtained during those 12 h.
Statistics
Haemodynamic parameters were analysed using a repeated-measures analysis of variance (SPSS version 15, SPSS Danmark, Hvidovre, Denmark), with the time after administration of sildenafil and the experimental type (MRI or VEP) as the within-subject factors. Neurophysiologic results from the VEP experiment were similarly analysed with respect to time after sildenafil ingestion. The integral of headache score was compared using a paired t-test. All values are presented as means±s.d., unless otherwise stated. P > 0.05 was considered significant.
Results
The study included 13 healthy females, mean age 23±3 years (mean±s.d.) and mean weight 70.3±6.6 kg (mean±s.d.). One subject dropped out after the first day of experiment (fMRI) complaining of severe migraine-like headache without accompanying symptoms 4 h after the ingestion of sildenafil.
Headache
Of 12 subjects, 10 experienced headache on the day of the MRI investigations and 9 on the day of the VEP investigation. Only one subject only did not experience headache at any time on either day. The integral of headache scores was 9.2±8.4 on the day of the fMRI session and 6.0±6.2 on the day of VEP examination; there was no significant difference between day 1 and day 2 or between the day of VEP and the day of fMRI examination. There was a trend towards higher headache scores during the day of MRI (P= 0.08), conceivably because of an interaction with CO2 inhalation. The median peak headache score was 1.5 (range 0 to 4) on the day of fMRI and 1 (range 0 to 3) on the day of VEP examination. Median time to peak headache score was 3.14h on the day of fMRI and 3.44 on the day of VEP examination (see Figure 1).
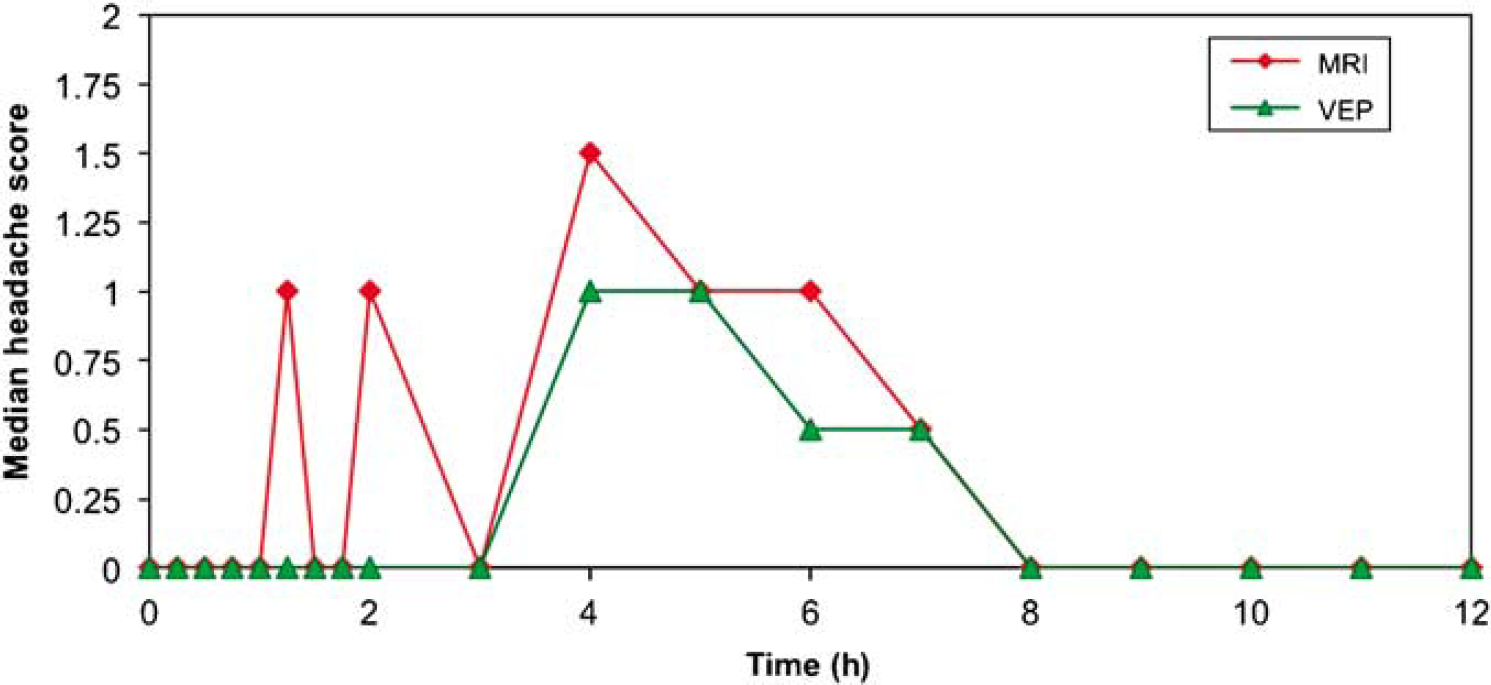
Mean headache score. Mean headache score after the intake of sildenafil is shown for the day of the VEP investigations (filled triangle) and for the day of MRI (filled circle). The two first peaks seen on the day of MRI represents headache at the time of CO2 stimulation; CO2 appeared to temporarily augment the headache response.
Haemodynamic and Respiratory Parameters
Results are shown in Table 1. There was no significant difference in blood pressure or heart rate between the day of the VEP examination and the day of fMRI. When performing a repeated measurement test, including data from both days, a slight decrease in systolic blood pressure was seen at 60 mins after the ingestion of sildenafil relative to baseline (P = 0.026), whereas decreases in diastolic blood pressure reached significance (P > 0.05) at 30, 90 and 120 mins. However, when analysing the days separately, no significant change was seen in systolic blood pressure, whereas diastolic blood pressure remained significantly changed at 30 and 90 mins on the day of fMRI and at 90 mins on the day of VEP (Table 1). There was no significant difference in heart rate relative to baseline.
Blood pressure and heart rate during in hospital observation
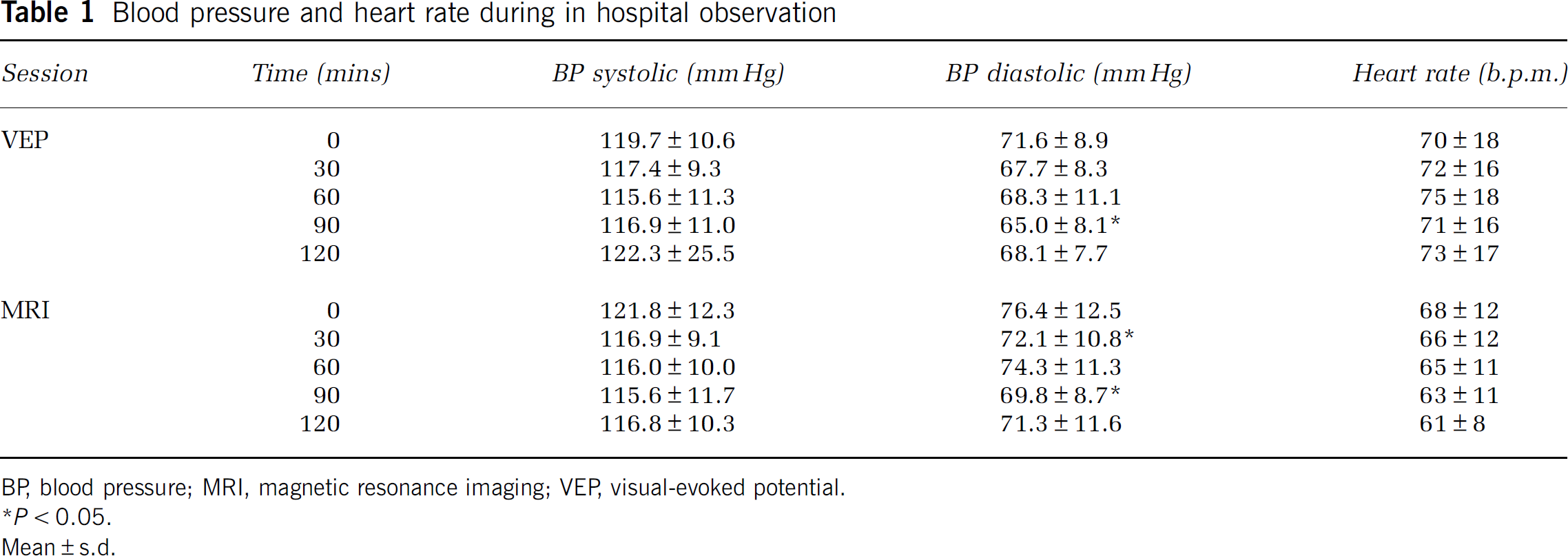
BP, blood pressure; MRI, magnetic resonance imaging; VEP, visual-evoked potential.
P>0.05.
Mean±s.d.
During the hypercapnic experiment, there was an average increase of ETCO2 of about 1.6 kPa in the stimulation relative to baseline periods; average values are reported in Table 2.
BOLD response values and ETCO2 before and after intake of sildenafil
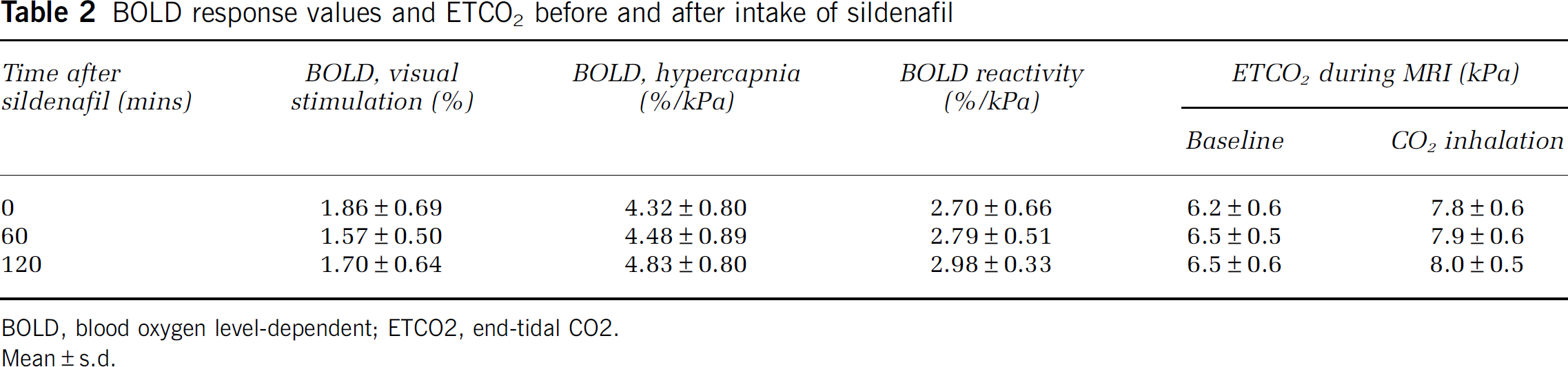
BOLD, blood oxygen level-dependent; ETCO2, end-tidal CO2.
Mean±s.d.
Visual-Evoked Potential
In general, there was no significant effect of sildenafil on the latency (P100) or maximal amplitude of VEP. However, a minor increase in latency at 60 mins was significant (P = 0.018). Results are shown in Table 3. In control experiments, no effect over time was found.
Visual evoked potentials: latency and amplitude values before and after the intake of sildenafil
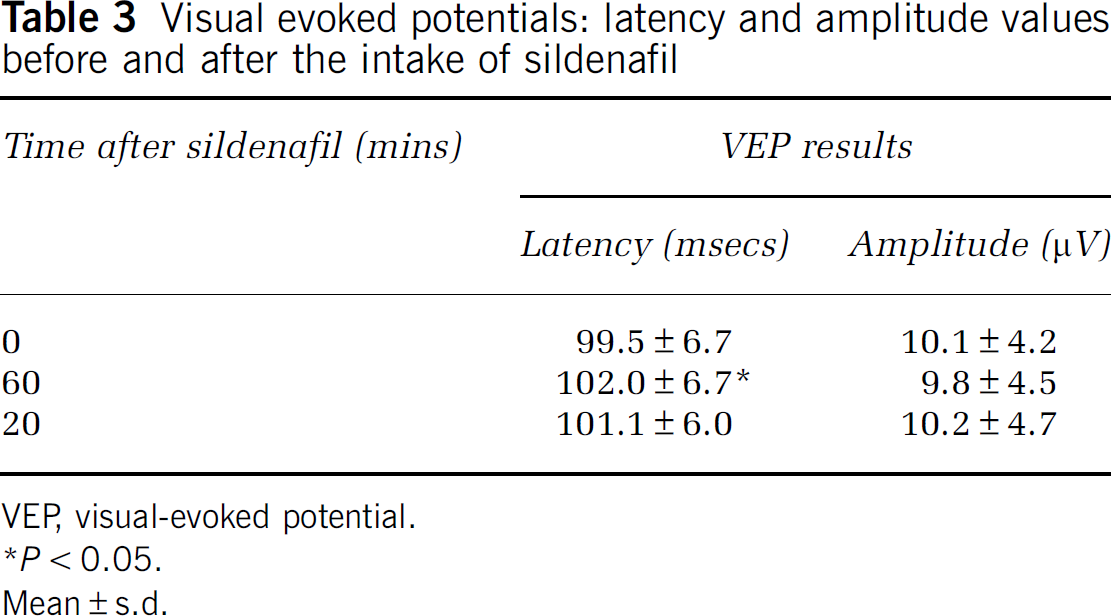
VEP, visual-evoked potential.
P>0.05.
Mean±s.d.
Blood Oxygen Level-Dependent Response
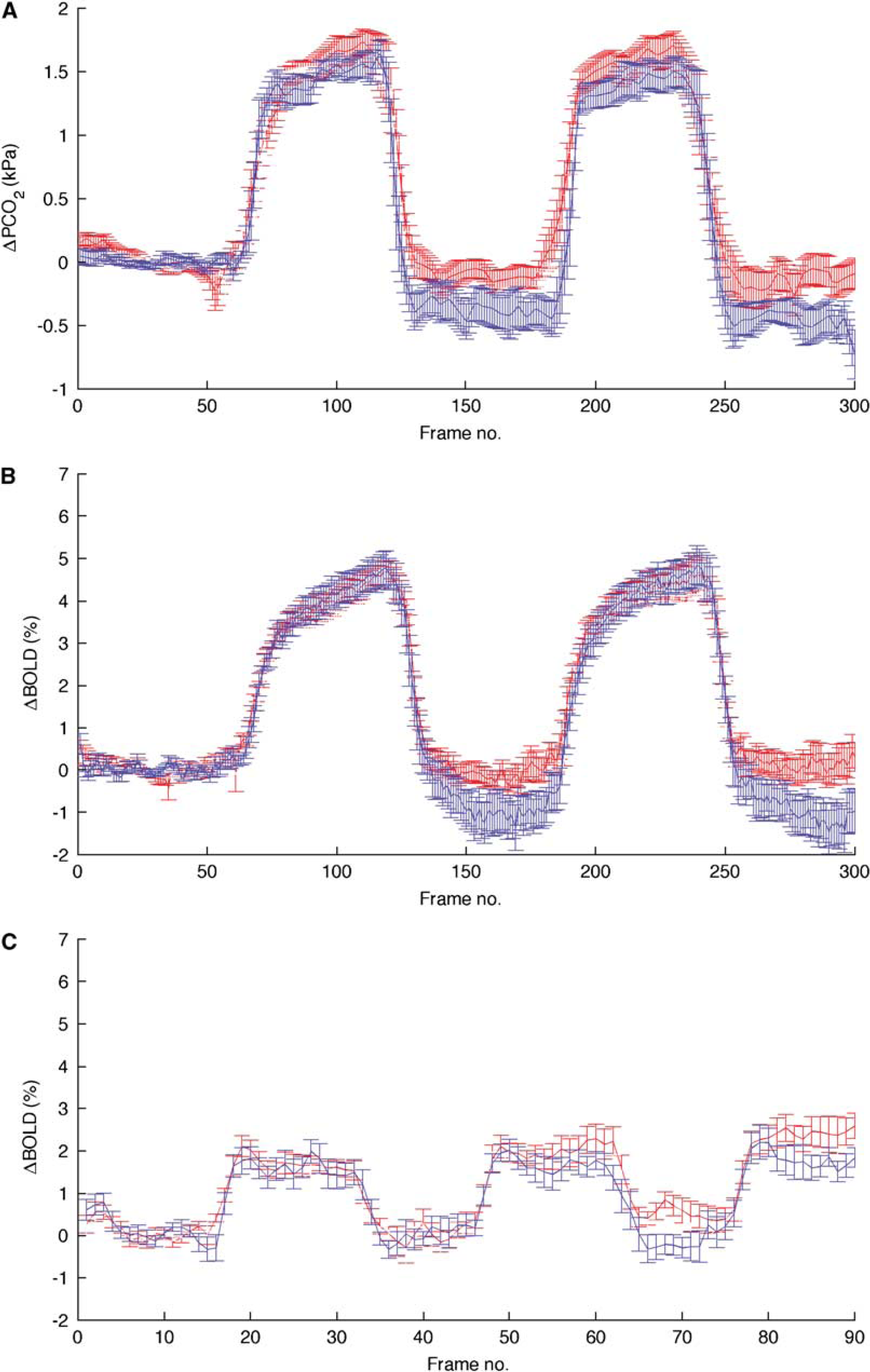
Both hypercapnia and visual stimulation elicited strong and consistent responses in each volunteer (see Figure 2 for an illustration of the average BOLD response distribution). However, the second level analysis did not reveal any areas of significant interaction between time (after sildenafil ingestion) and stimulation. To optimise sensitivity, a region of interest-based analysis was also performed. This confirmed that the BOLD response to visual stimulation or CO2 inhalation did not change after sildenafil administration (the average response magnitudes are given in Table 2). Signal time courses from the regions of interest are shown in Figures 3B and 3C; an apparent session difference between the ingestion of sildenafil and subsequent sessions is also present in the average ETCO2 curve and, therefore, did not give rise to any significant difference in CO2 reactivity. No effect over time or of repeated stimulation was found in control experiments.
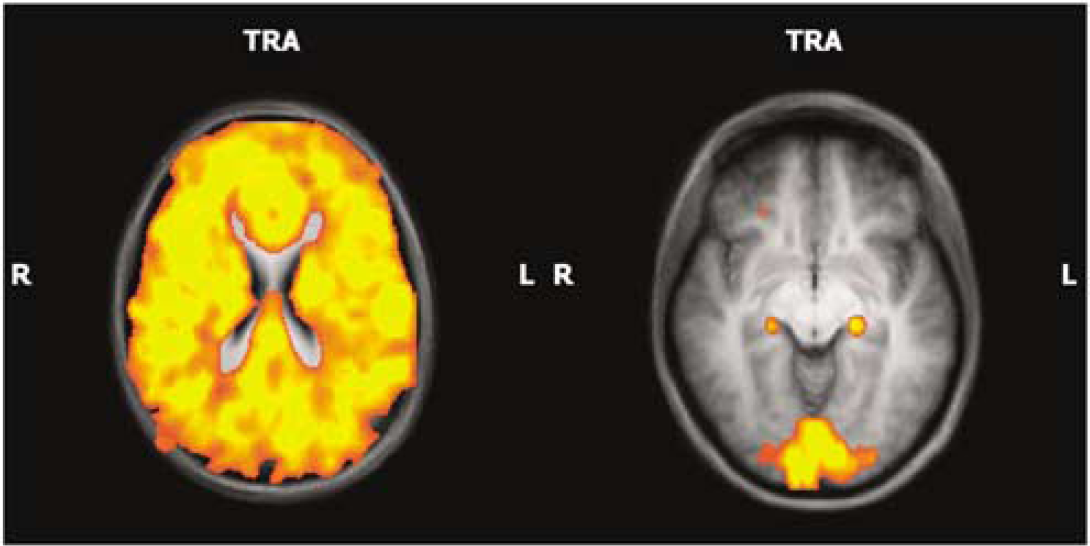
Blood oxygen level-dependent imaging during visual stimulation and CO2 inhalation. Colour coding shows response magnitude in areas with a significant response to hypercapnia (left panel) or visual stimulation (right panel); threshold at FDR>0.02.
(
Discussion
Sildenafil induced a mild headache in almost all subjects, similar to that seen in earlier studies in healthy subjects (Kruuse et al, 2002). In general, the headache was initiated within the first hour of administration and the pain-intensity peaked 3 h thereafter. A slight decrease in diastolic blood pressure but no change in heart rate was induced.
Despite the headache-inducing effects, sildenafil had no significant effect on the visual BOLD response or the BOLD response after hypercapnia. Sildenafil administration did not influence the duration or amplitude of the VEP response, except for a minor increase in latency after 1 h. This is the first report on cerebrovascular reactivity after sildenafil intake in healthy subjects, and the first study to use the technique of BOLD imaging in establishing the possible effects of sildenafil on visual stimulation and hypercapnia.
Blood oxygen level-dependent imaging reflects the coupling between neuronal activity and vascular response in brain tissue, and represents a balance between the supply and metabolism of oxygen in the tissue investigated (Logothetis and Wandell, 2004). Owing to the effect of extravascular field distortions, the BOLD effect is generally considered more sensitive than perfusion imaging. Several factors affect the BOLD signal (Logothetis and Wandell, 2004). The limitations of BOLD arise when increases in metabolic rate and CBF occur concomitantly and to the same extent. Conceivably, a change in the BOLD signal because of an increased flow response may be offset by a larger increase in oxygen metabolism. So far, however, there is no report of sildenafil affecting tissue metabolism, and our study seems to support these findings, as we did not see any change in the BOLD response.
Sildenafil, used for treatment of erectile dysfunction and pulmonary hypertension, is a compound that specifically affects the cGMP signalling by inhibiting one of the enzymes responsible for cGMP breakdown, PDE5. The action and signalling of cGMP is, therefore, prolonged and/or potentiated by this PDE5 inhibitor (Corbin and Francis, 1999). It is a lipophilic molecule that passes the blood–brain barrier (Milman and Arnold, 2002; Pagani et al, 2005). Sildenafil can thus be used as a specific tool to modulate the NO–cGMP pathway in cerebral circulation and brain signalling. The presence of PDE5 enzyme is described in cerebral arteries (Kruuse et al, 2005), trigeminal ganglion and in several areas of the brain (Giordano et al, 2001; Kruse et al, 2006; Van Staveren et al, 2003).
As sildenafil had no effect on CBF or large cerebral or extracerebral arteries, it was hypothesised earlier that cGMP and sildenafil may exert its headache-inducing effects by modulating neuronal or neurovascular reactivity to intrinsic or extrinsic stimulation (Kruuse et al, 2003, 2002). In erectile dysfunction, sildenafil inhibitors of PDE5 only elicit their erectogenic effects when subjects are sexually aroused (Rosen and Kostis, 2003). Sildenafil thus enhances an intrinsic vascular and neuronal response related to the NO–cGMP signalling in penile tissue (Ballard et al, 1998; Rosen and Kostis, 2003). An effect of sildenafil on cerebrovascular reactivity was not investigated in the earlier CBF studies, as no external stimulus was applied to the subjects during CBF acquisitions.
Nitric oxide–cGMP signalling is involved in the headache mechanisms, although the exact role remains to be elucidated (Olesen, 2008). The augmentation of intracellular cGMP levels has been suggested to increase neuronal excitability, thus modulating either the peripheral or the central parts of the pain signalling (Barnstable et al, 2004; Levy and Strassman, 2004).
Sildenafil could induce headache by altering neurovascular reactivity or by decreasing the threshold for either peripherally or centrally mediated neuronal activation in general. Normal sensory impulses, such as artery pulsation or light, may thus be perceived as painful. It could also be speculated that an impaired neurovascular coupling could facilitate the development of headache based on the hypothesis that limitations in substrate supply and washout of metabolites and signalling molecules in activated brain regions could facilitate the induction of headaches in nonmigraine volunteers. In a recent study, a posterior hypoperfusion was detected during attacks of migraine without aura, which proceeded after pain relief (Denuelle et al, 2008). Earlier studies in migraine patients had also shown altered responses to visual stimulations (Cao et al, 2002; Schoenen et al, 2003).
The NO–cGMP signalling has for long been suggested to be crucial in several neuronal and cerebrovascular signalling pathways (Pelligrino et al, 1993). Nitric oxide and cGMP are known to be involved in neurotransmission (Garthwaite, 2008; Moncada et al, 1991). The modulatory role of NO and cGMP appears to vary between brain regions, between neurons and between pre- and postsynaptic events, being either excitatory or inhibitory depending on location (Barnstable et al, 2004; Levy and Strassman, 2004). Cellular cGMP may affect downstream signalling through the activation of cGMP-dependent protein kinases, activating cyclic nucleotide-gated ion channels (Barnstable et al, 2004) or by feed-back signalling on other PDEs (Bender and Beavo, 2006). Cyclic guanosine monophosphate is associated with N-methyl-
Whether sildenafil affects local or global CBF as a response to various stimuli is debatable. In healthy subjects, oral sildenafil of 100 mg, which is the highest dose recommended for humans, has so far been reported to have no effect on global or regional CBF (Arnavaz et al, 2003; Kruuse et al, 2002). In patient studies, reports are varied as are the techniques for measuring blood flow changes (Diomedi et al, 2005; Kruuse et al, 2003; Rosengarten et al, 2006). In animal studies, only effects on normal rats have been investigated. Oral administration of sildenafil (2 mg/kg) significantly increased local CBF, measured by laser Doppler, up to 70 mins after dose compared with controls (Zhang et al, 2002).
This discrepancy between healthy subjects and animals could be owing to species difference, difference in dosage between humans and rats or in the techniques chosen for CBF measurements, or any combination thereof.
This study found no change in the BOLD response (in either the duration or intensity) to hypercapnia or visual stimulation after sildenafil administration to healthy subjects. The headache response to sildenafil was similar to that reported earlier (Kruuse et al, 2002), suggesting that sildenafil did have effects relative to the dose given. It can be noted that two subjects reported an increase in headache intensity during hypercapnia.
The pain-sensing structures of the brain are the proximal parts of the large cerebral arteries, the dura mater in close proximity to the arteries and the venous sinuses. Mechanical stimulation of these areas induces referred pain in areas that are also reported to localise pain during migraine attacks (Ray and Wolff, 1940). This peripheral afferent pain signalling involves the ophthalmic branch of the pseudo-unipolar trigeminal nerve. The cell bodies of the trigeminal nerve are located in the trigeminal ganglion having peripheral synapses at the arteries and dura, and central synapses on the second-order neurons in the trigeminal nucleus caudalis and the upper cervical dorsal horns. This is termed as the trigeminovascular system. The signals convey centrally to the third-order neurons of the thalamus, and onto the somatosensory cortex where pain is perceived (May and Goadsby, 1999). Activation of the trigeminal nerve may induce vasodilatation by the peripheral release of neuropeptides, such as calcitonin gene-related peptide, pituitary adenylatecyclase-activating polypeptide and substance P. The central part of the pain signalling is subject to modulation by brain areas, such as the periaquaductal grey, the dorsal pons or the hypothalamus. In the brainstem, the trigeminal nucleus caudalis may activate the superior salivatory nucleus and parasympathetic efferent through the sphenopalatine ganglia projecting to the dural arteries, thus promoting a reflectory vasodilatation by the peripheral release of NO, acetylcholine and vasoactive intestinal peptide (May and Goadsby, 1999; Pietrobon and Striessnig, 2003). The trigeminal signalling is thus part of the extrinsic innervation of brain vessels (Hamel, 2006).
If sildenafil induced a general hyperreactivity or hyperexcitability, it may also be reflected in the trigeminal system. However, no activation of brain regions other than those involved in visual stimulation was detected. It would appear that the headache-inducing effects of sildenafil are mediated through mechanisms other than an overall hyperreactivity to external stimuli, whether regional (visual stimulation) or global (hypercapnia). The headache-generating mechanism may be confined either to the peripheral part of the pain-sensing system, that is, the trigeminal nerve endings and trigeminal ganglia, or perhaps to the brain-stem level. The finding of PDE5 mRNA and protein in the trigeminal ganglion, as well as the spinal trigeminal nucleus, may support evidence for this theory (Kruse et al, 2006). Alternatively, sildenafil may selectively affect the central sensory processing in the hypothalamus or the thalamus, which was not detected by the set-up of BOLD during visual stimulation alone. Investigation of this hypothesis requires further studies in which experiments with specific stimulation of the trigeminal pain system (Borsook et al, 2006) should be performed, preferably on migraine patients. Activation in the brainstem was not detected in this study, which could be owing to the level of physiologic noise present in this area masking minor changes (Harvey et al, 2008).
This study's findings regarding cerebrovascular reactivity in healthy subjects differ from earlier studies, which have mainly included nonhealthy subjects (Diomedi et al, 2005; Rosengarten et al, 2006). An increase in the cerebrovascular reactivity, measured by the breath-holding index, has been reported in patients suffering from endothelial dysfunction (Diomedi et al, 2005). Furthermore, in patients suffering from pulmonary hypertension, an augmentation of occipital CBF velocity response to visual stimulation was described (Rosengarten et al, 2006). However, whether this is owing to a direct effect on vasculature or to neuronal signalling is not known. The aforementioned two studies (Diomedi et al, 2005; Rosengarten et al, 2006), however, measured only the blood flow velocity, not CBF. No effect on CBF was detected in migraine patients by 133Xenon inhalation and single-photon emission computerised tomography (Kruuse et al, 2003). As a result, it remains unclear as to whether sildenafil, in patients with a proposed defect in NO signalling or a dysfunctional endothelium, changes the overall or local CBF. Comparison of these findings with the studies of patients with diseases affecting endothelial function may indicate that sildenafil has an effect only when a dysregulation of the NO–cGMP system is present. In pulmonary hypertension, a decreased NO drive appears to be present, which sildenafil may be able to improve. Similarly, with endothelial dysfunction, the NO production appears to be attenuated and sildenafil normalises the endothelial response (Vlachopoulos et al, 2004). With regard to animal models of neurologic diseases, the effects of sildenafil on the rat stroke model were recently investigated. In the rat stroke embolus model, where an embolus is generated in the middle cerebral artery, sildenafil is not found to influence the ischaemic lesion size. In spite of this, sildenafil improves functional recovery, local angiogenesis and possibly regional CBF at a later stage in the ischaemic boundary region (Li et al, 2007). There are a few case reports of sildenafil inducing cerebral stroke or cerebral haemorrhage, and the administration of sildenafil to stroke patients is so far contraindicated. This is partly based on the risk of not only creating a steal phenomenon (shunting blood from the infarcted area to the normal area, thus increasing the infarct size) but also on the risk of increased bleeding because of the mild antithrombotic effect of PDE5 inhibitors. In the light of the positive effects of sildenafil in the rat stroke model, together with the findings that sildenafil does not affect normal cerebral arteries, CBF or BOLD responses in healthy subjects, the risk of inducing a cerebral steal phenomenon in stroke appears less likely.
In relation to the basic physiologic mechanisms in the cerebrovascular response to hypercapnia, cGMP levels alone do not appear to be an enhancing factor. Rather, cGMP may play a permissive role in the increased BOLD level seen in healthy subjects, essential for development of a response but with no effect on the duration or magnitude thereof. In patients with cerebrovascular diseases involving NO–cGMP signalling, concentrations of cGMP may be lower, to the point of becoming a limiting factor on which PDE5 inhibition may have an effect.
Conclusion
This study's data suggest that sildenafil in healthy subjects neither potentiates a neuronal or local cerebrovascular visual response nor influences a global cerebrovascular response to CO2 inhalation. Sildenafil did induce a mild headache similar to earlier studies, but a generally increased neuronal response or an increased vascular reactivity appeared not to be involved in the pain process. The data further imply that sildenafil, and subsequent augmentation of intracellular cGMP, does not in itself modulate the hypercapnic response in healthy subjects.
Footnotes
Acknowledgements
The authors thank Britta Riege Jensen, Anne Grønkjær-Nielsen, Marjut Lindhart and Bente Sonne Møller for their technical assistance.
The authors state no conflict of interest.