
Abstract
Snake envenomation is a rare incident during pregnancy and potentially challenging to manage. Snakebites in pregnancy may lead to several complications such as teratogenicity, miscarriage, antepartum hemorrhage, and even intrauterine fetal death. Here, we report a case of a pregnant woman who presented to our emergency department with signs of systemic envenomation following an Indian cobra bite on her foot, highlighting the key obstetric and wound management challenges. She complained of severe pain at the site of the bite and progressive swelling, abdominal pain, and multiple episodes of vomiting, which started 45 min after the bite. She received 10 vials of polyvalent antivenom from a primary hospital and was then referred to our center. The patient underwent emergency cesarean section and later fasciotomy with free-flap reconstruction at the bitten site due to local tissue necrosis. The case was successfully managed by a multidisciplinary team consisting of an emergency physician, obstetrician, and plastic surgeon, saving 2 lives and the limb of the patient.
Introduction
Snake envenomation (SE) is a significant public health problem in Southeast Asian countries (SEAC) and accounts for substantial mortality and morbidity.1,2 India alone accounts for nearly 58,000 deaths annually due to SE. 3 SE is a rare incident during pregnancy and potentially challenging to manage, where epidemiological studies from SEAC reported pregnant women accounted for 0.4 to 1.8% of hospitalized snake bite victims.4,5 SE in pregnancy may lead to a number of complications, such as teratogenicity, miscarriage, antepartum hemorrhage, and even intrauterine fetal death. 3 -5 SE in pregnant females is documented to have poor outcomes, with fetal deaths as high as 38 to 43% and maternal deaths of nearly 10%. 4 -6 The definitive treatment for envenomation is the administration of specific antivenom (AV).1,2 There is a risk of an anaphylactic reaction, which can cause detrimental effects on the fetus as well as the expectant mother. 4 -6 Although earlier studies documented a higher rate of fetal deaths among mothers who received AV therapy, risks/benefits must be considered as most moderate to severe bites favor AV administration. 4 -6 The possible anaphylaxis can be treated.
The major venomous snake species in India include Indian cobra (

The spectacled Indian cobra (
Case Report
A 26-y-old woman presented to our ED 4 h after a snake bite on her right foot while sitting outside her home. The snake was identified by the patient as Indian cobra. She complained of severe pain at the site of the bite, progressive swelling, abdominal pain, and multiple episodes of vomiting, which started 45 min after the bite. First, she was taken to a nearby health center 60 min after the bite, where she received 10 vials of polyvalent AV, and then she was referred to our center. The pain in the foot was 10/10 on the numerical rating scale at presentation. Her history revealed gestational age of 34 wk and 3 d by the last menstrual period. Her vitals on arrival at our ED were heart rate 110 beats/min, respiratory rate 18 breath/min, SpO2 98%, and blood pressure 120/70 mm Hg. She denied any loss of consciousness, hematuria, dysphagia, and dyspnea. Her single breath count was 22, and her “broken neck sign” was negative. An obstetric call was made in view of the potential risk of envenomation to the fetus. The right foot examination revealed 2 fang marks on the dorsum of the foot, moderate swelling extending to the ankle, and tenderness (Figure 2A). However, distal pulses (dorsalis pedis artery) were present. Her complete blood count revealed elevated total leucocyte count (13.89 × 103cumm) and neutrophil count (91.7%). Her whole blood clotting test result was negative, and the coagulation profile was within normal limits. The wounds were cleaned and dressed. Tetanus immunization was already received 2 mo prior. She was treated with an additional 10 vials of polyvalent AV and antibiotics. Initially, she received an intravenous injection of paracetamol 1000 mg for local pain in the foot, which had not subsided. Ultrasound-guided selective blocks of the superficial peroneal nerve and sural nerve were given with 3.5 mL of 0.375% ropivacaine, which brought the numerical rating scale score to 2/10.

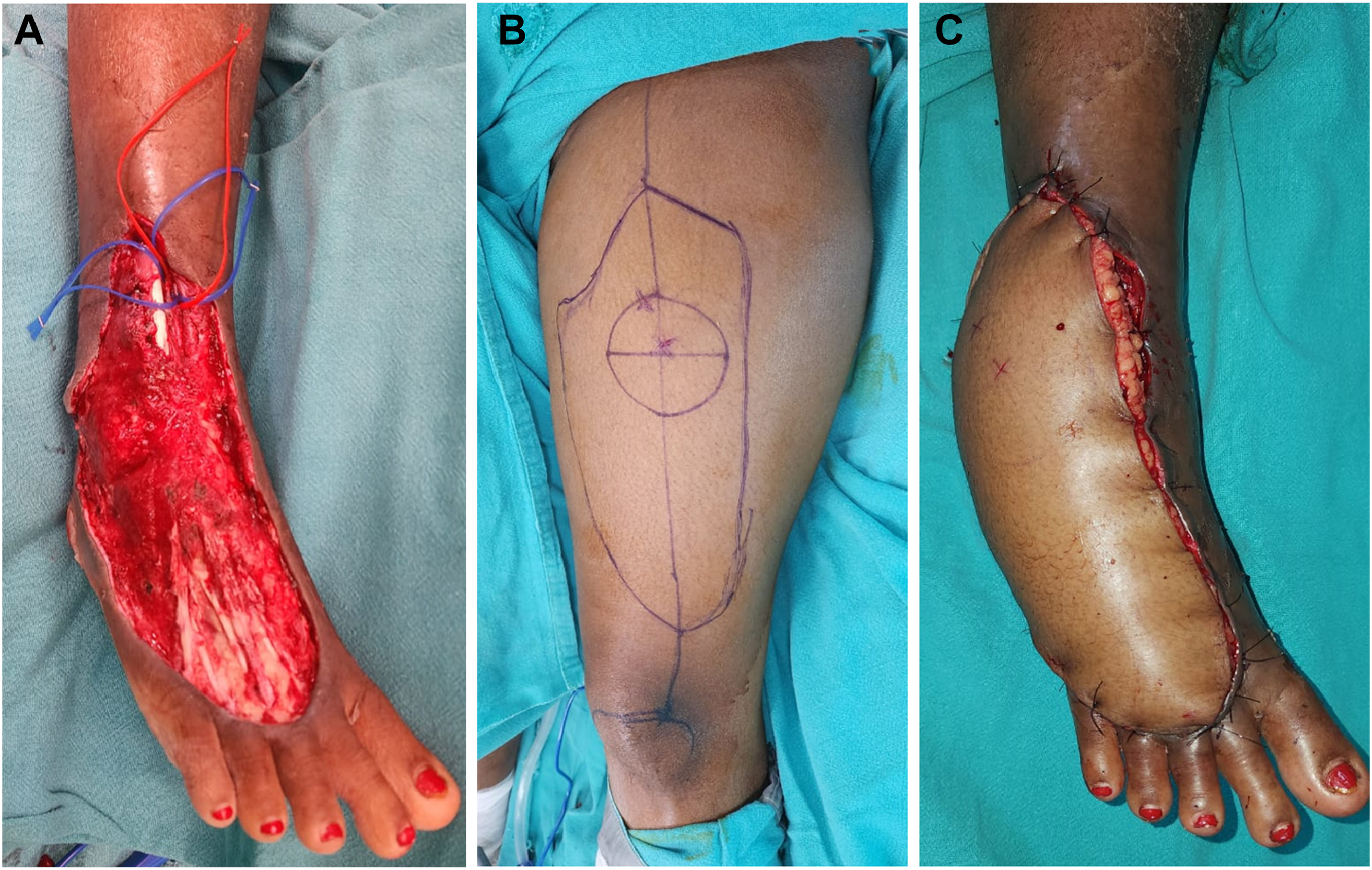
A, The right foot showing 2 fang marks on the dorsum of the foot, moderate swelling extending to the ankle, and tenderness. B, The patient developed blisters and local tissue necrosis over the bitten site on the third day after snake bite. C, Fasciotomy was performed on the seventh day after snake bite owing to the exaggerated risk of compartment syndrome and feeble peripheral pulsations (dorsalis pedis).
The patient was transferred to the obstetrics department. On examination, the maternal pulse rate was 110 beats/min. Abdominal examination revealed symphysio-fundal height corresponding to 34 wk of gestation, with a singleton live fetus in longitudinal lie and cephalic presentation. The uterus was relaxed, and the fetal heart rate was 191 beats/min. There was no vaginal bleeding. In view of sustained fetal tachycardia, she underwent an emergency cesarean section, which was uneventful. She delivered a preterm female baby weighing 2140 g. There was no evidence of abruptio placentae. The baby was managed in the neonatal intensive care unit for 48 h in view of mild respiratory distress due to transient tachypnea of the newborn. The patient was monitored for limb swelling and followed up for any other complications.
The patient developed blisters and local tissue necrosis over the bitten site on the third day of the SE (Figure 2B). She was started on broad-spectrum antibiotics and other anti-inflammatory drugs. The foot swelling extended to below the knee, and the blisters ruptured. The distal pulses were recorded at regular intervals along with daily compartment pressure monitoring. Fasciotomy was done on Day 7 owing to the risk of compartment syndrome (compartment pressure, >30 mm Hg) and weak peripheral pulsations (dorsalis pedis) (Figure 2C). The wound dressing was changed every day. The local pain subsided in 1 wk, and the swelling subsided within 2 wk of the SE. On the 21st day, she underwent reconstruction of the foot defect with an anterolateral thigh free flap taken from the front of the thigh region, which was uneventful (Figure 3A–C). She was asymptomatic and doing well at the 6-wk follow-up. Written informed consent was obtained from the patient before the peripheral nerve block and for the publication of clinical images and case details.
A–C, Reconstruction of the foot defect with an anterolateral free flap taken from the front of the thigh.
Discussion
Snake envenomation is a rare incident during pregnancy, and literature about the management of these victims is sparse.
4
The effect of envenomation on the mother and fetus depends on the biochemical and proteomic composition of the injected venom.1,2 Most common venom constituents include various biogenic amines, enzymes, peptides, nonenzymatic polypeptide toxins, digestive hydrolases, hyaluronidase, and activators or inactivators of physiological processes.1,2 Wong et al
7
reported that the major constituents in the venom of Indian cobra (
Antivenom is the definitive treatment for SE, along with other supportive therapies.1,2 Although SE and AV administration pose unique challenges with respect to the health of both mother and fetus, there exist no specialized guidelines for SE during pregnancy to date. 8 The treatment should be directed by a multidisciplinary team, including an obstetrician, emergency physician, neonatologist, toxicologist, and general or plastic surgeon. 8
Literature documented a high incidence of spontaneous abortion following SE during pregnancy. 4 -6 Various mechanisms have been proposed for the occurrence of fetal death or abortions following SE, such as direct venom toxicity on the fetus leading to fetal anoxia, premature uterine contraction, hemorrhagic manifestations to the placenta or uterus, maternal shock, cytokinin release, and anaphylactic reaction from the AV.9,10 Seneviratne et al, 5 in their study from Sri Lanka, documented that the major factors associated with the risk of adverse fetal outcomes are systemic envenomation and a gestational period of 18 wk or less. Our case was in the third trimester of pregnancy and nearly full term. The fetal tachycardia started while the patient reported to the ED, which prompted the treating team to proceed with an emergency cesarean section to prevent further envenomation to the fetus and the risk of AV anaphylaxis reactions. Although AV is the definitive treatment for envenomation, there is a risk of anaphylactic reactions and negative fetal outcomes following treatment with adrenaline, as adrenaline may compromise placental circulation. 5 The AV administration is recommended if the benefits to the mother and fetus outweigh the risk. Seneviratne et al 5 studied SE during pregnancy in Sri Lanka and reported the prevalence of abortion and fetal malformation to be as high as 60% in the case of systemic envenomation. Langley, 4 in his review, reported the rate of maternal deaths to be 2.1% and the rate of fetal death to be 30.2% among pregnant women who received AV treatment, in contrast to the maternal death rate of 6.6% and fetal death rate of 11.3% among those who did not receive AV. This is mostly attributed to the fact that the patients treated with AV are systemically envenomated and are seriously ill compared to the patients who did not receive AV. The rate of maternal death here is lower with AV, and the rate of fetal death is higher with AV. The explanation that patients who received AV are more critically ill would explain the higher rate of fetal death in patients receiving AV but does not explain why maternal mortality is lower.
Singh and Mohanty 8 reported a patient with vasculotoxic SE at 29 wk of gestation who received 15 vials of polyvalent AV and later successfully delivered a healthy baby at 36 wk of gestation. However, the fetal outcome was grave in a patient with SE at 26 wk of gestation who presented to the hospital with an abruptio placentae, as reported by Mittal et al 9 from north India. The authors attributed the untoward outcome to the delay in AV administration that resulted in bleeding manifestations, including abruptio placentae and, later, disseminated intravascular coagulation. 9 Notably, our patient received 10 vials of polyvalent AV within 2 h of SE before presenting to our center. Adewole et al 10 reported a patient with SE at 32 wk of gestation from Nigeria who presented with bleeding manifestations, including per-vaginal bleeding, and underwent spontaneous normal vaginal delivery during the course of emergency treatment by the multidisciplinary team, wherein both the mother and fetus had a favorable outcome.
The local tissue injuries following SE were another concern in the present case, wherein blisters and local tissue necrosis started from the third day of SE, along with ascending limb edema. Fasciotomy was required for the case to prevent the risk of compartment syndrome. Singh and Mohanty 8 also reported the need for fasciotomy in a woman with vasculotoxic SE at her 29th wk of gestation. Although most soft tissue damages after SE can be managed conservatively, some cases require debridement and flap reconstruction if there is an exposure of tendon, bone, or neurovascular structures. The present study’s patient also underwent free flap reconstruction at the fasciotomy site after 3 wk, which was uneventful. Lee et al 11 earlier reported an average time interval of 24 d from injury to flap surgery in their series of SE wound management that had a favorable outcome.
Conclusion
To conclude, SEs are rare incidents during pregnancy. Factors such as degree and type of envenomation, gestational age at presentation, timing, and quality of treatment determine the maternal and fetal outcome following SE during pregnancy. Specific guidelines for managing SE in pregnancy will help patient management and improve maternal and neonatal outcomes. The guidelines should specify the dose of AV for pregnant women, the timing of administration of AV, the plan of follow-up for women with SE in each trimester of pregnancy, and complications to be anticipated after SE. The risks/benefits must be considered in most moderate to severe SE for AV administration. Early administration of AV and other supportive treatments by a multidisciplinary team are paramount to have a favorable outcome.
Footnotes
Acknowledgment
We are thankful to Shri Suvendu Mallick, Head, Odisha Snake Helpline, for providing us with the image of an Indian cobra (
Author Contributions: conceptualization (lead), methodology (lead), software and investigation (lead, equal), formal analysis, writing—original draft (lead, equal), supervision, project administration (CRM and RP); methodology (lead), software and investigation (support), formal analysis, writing—original draft (lead), supervision, writing—review and editing (SS); methodology (support), investigation (support), data curation, writing—original draft (lead), writing—review and editing, visualization (RVR); software (support), writing—review and editing, visualization (IMS); software (support), writing—review and editing, visualization (AVP); software and investigation (support), writing—review and editing, validation, visualization (AR); overall supervision of the whole study (CRM); all authors made a substantial contribution. All authors have read and agreed to the content of the final manuscript.
Financial/Material Support: None.
Disclosures: None.