
Abstract
Puerto Rico (PR) is home to 10 indigenous species of snake. Alsophis portorricensis has traditionally been considered harmless. In 1961, Hageman classified A portorricensis as somewhere between “venomous” and “nonvenomous.” In 1966, Heatwole and Banuchi reported the only case found in the literature of a “venomous” bite from Alsophis portorricensis. Only 6 cases of snakebite were reported to the PR Department of Health from 1998 to 2007; ecchymosis, swelling, and abnormal vital signs were noted in all of the cases. In 5 of these 6 cases, the captured snake was, in fact, identified as Alsophis portorricensis of the Colubridae family; in the remaining case, the description strongly suggests that it was the same species as the others. All bites were inflicted on fingers, which were presented for evaluation from 2 to 24 hours after the event. All documented cases report that the bite lasted from 1 to 4 minutes. All of the victims presented with localized pain and ecchymosis. Localized edema extended from the hand to the elbow in 4 cases, and up to the shoulder in 2 cases. All patients were treated symptomatically, observed at the Emergency Department (ED), and discharged home within 24 hours after the ED evaluation. All patients reported the resolution of symptoms within 1 week. Traditionally, PR has not been associated with any dangerous species of snake. These cases show that the second most abundant snake on the island can inflict a venomous bite, with local and systemic symptoms that warrant adequate preparation by the medical community.
Introduction
There are 10 species of snakes native to Puerto Rico (PR), all of which were popularly believed to be nonvenomous. Rodriguez-Robles defined venom as a mixture of various components (including toxins) that are produced by specialized glands in an animal and then injected, for either feeding or defensive purposes, into another animal by spurs, stings, or fangs. 1 Three families of snake are represented in PR: Typhlopidae, with only one genus (Typhlops); Boidae, also with one genus (Epicrates); and Colubridae, with two genera (Alsophis and Arrhyton). Of the 5 subspecies of A portoricensis, also called the Puerto Rican racer, only 2 of these, A portoricensis portoricensis and A portoricensis prymnus, are found on the PR mainland (Figures 1 and 2). The other subspecies are found on Culebra, La Mona, and Vieques, small islands off the mainland of PR.2,3Alsophis portoricensis is the second largest snake in PR and can reach up to 3 feet (1 meter) in length.

The Puerto Rican racer (Alsophis portoricensis).

The Puerto Rican racer (Alsophis portoricensis).
In 1966, Heatwole and Banuchi 4 reported on the bite of A portoricensis. A 20-year-old male patient was bitten on the left index finger. The patient had initial swelling and pruritus along with a hematoma. The condition became progressively worse, involving the entire arm, including the axilla, and the upper anterior chest muscle. He was seen at the San Juan City Hospital, where he was given penicillin and streptomycin, after which the finger was incised and drained. When evaluated at another institution 3 days later, the patient had developed lymphangitis and cellulitis of the upper extremity. The patient did not have any permanent adverse effects from the snakebite. Since then, there have been no further case reports in the literature, although anecdotal reports of bites passed down for generations on our island. We present a case series of snakebites that were reported to the PR Poison Control Center and Department of Health from 1998 to 2007. The 6 cases are presented below in detail.
Case #1
A 30-year-old man with no history of systemic illness or allergies was bitten for about 2 minutes on the second digit of the left hand 2 hours before arriving at the Emergency Department (ED). The patient's vital signs (VS) were: temperature (T) 37°C, blood pressure (BP) 128/76, heart rate (HR) 76, respiratory rate (RR) 12. A physical examination of the bite showed 2 puncture wounds over the middle phalanx of the second digit, with associated erythema and bullae surrounding the wound. Swelling and ecchymosis extended to include the entire hand, without alteration of motor or sensory functions. Laboratory results, including a coagulation profile, were within normal limits. Intramuscular (IM) tetanus toxoid and ketorolac, and methylprednisolone, 125 mg intravenously (IV), were administered. The patient was discharged home 6 hours later. The patient did not experience any clinical improvement while under observation at the ED. Follow-up 24 hours later revealed swelling and ecchymosis extending proximally to include the forearm but still without motor or sensory deficits; there were no signs of necrosis or long-term tissue loss. Follow-up 1 year later revealed that the swelling had resolved within a 1-week period. No motor or sensory deficit was reported at any time.
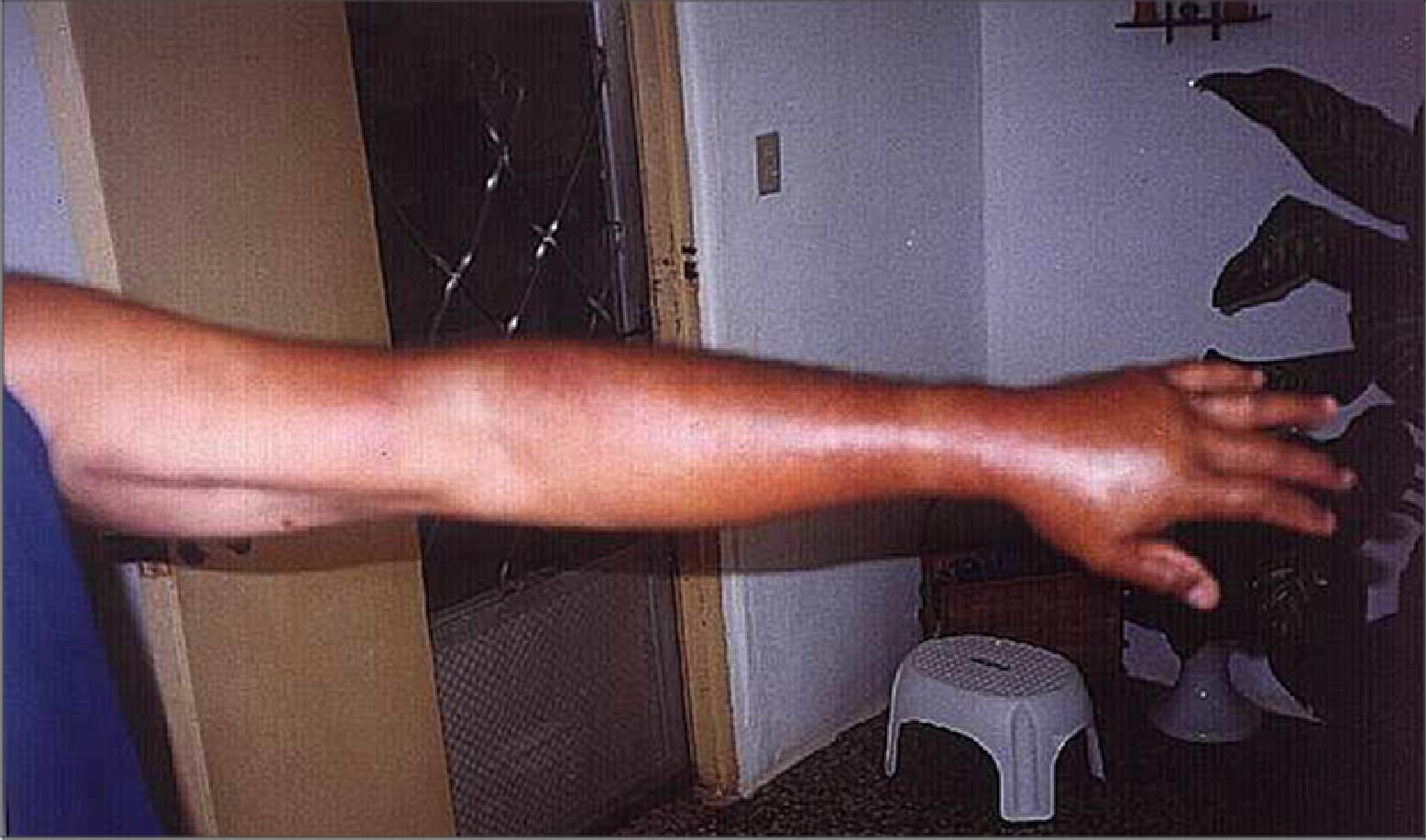
Case #2 (Figure 3)
A 65-year-old man with no history of systemic illness presented to the ED 12 hours after sustaining a snakebite to the first digit of his left hand. The patient reported that the duration of the bite was about 3 minutes. VS: T 37°C, BP 145/80, HR 87, RR 14. The first digit, distal phalanx, presented with 2 puncture wounds associated with erythema and ecchymosis extending towards the forearm (Figure 3). Treatment consisted of IM ketorolac, tetanus toxoid, and IV methylprednisolone. The patient reported referred pain along his hand and up to the shoulder. No neurovascular deficit was noted. A follow-up phone call 1 year later revealed clinical improvement within a 2-week period, though the patient admitted to occasional cold sensitivity in the area of the wound.

Case 2.
Case #3 (Figure 4)
A 21-year-old man with no history of systemic illness, allergic to aspirin, presented to the ED 24 hours after receiving a snakebite to the middle phalanx of the second digit of his left hand. The patient reported that the snake kept its grip for approximately 2 minutes. VS: T 36°C, BP 120/82, HR 64, RR 12. The left hand presented with 2 puncture wounds on the middle phalanx associated with erythema, pain, and ecchymosis around the bite and swelling up to the elbow (Figure 4). No neurovascular deficit was noted. No laboratory tests were ordered; the patient was given morphine sulfate IV, tetanus toxoid IM, and methylprednisolone 125 mg IV. The patient was discharged home after 10 hours of observation in the ED. A follow-up phone call 12 hours later revealed no change in the patient's condition. A follow-up phone call 1 year later revealed that there had been clinical improvement within a 1-week period. No neurovascular deficit was noted.
Case 3.
Case #4
A 13-year-old boy with no history of systemic illness was taken to the ED 24 hours after being bitten by a snake on the index finger of his right hand. The patient reported that the snake held its bite for 3–4 minutes. In addition, he said that he had vomited 2 times before arriving at the ED. VS: T 37°C, BP 100/76, HR 64, RR 12. Visual examination of the affected extremity confirmed a pair of puncture marks on the middle phalanx and edema of the hand. The patient also had pain running up to his shoulder and complained of paresthesia of the involved forearm without any focal deficit. Laboratory results revealed only leukocytosis. Treatment was oral ibuprophen, methylprednisolone IV, and tetanus toxoid IM. A follow-up phone call 8 hours later determined that the patient had been transferred to another institution for surgical evaluation to rule out compartment syndrome. Six hours after the surgical evaluation, the patient was discharged home; by that time, the edema and ecchymosis had diminished. Both resolved completely within a 1-week period.
Case #5
A 15-year-old boy with a history of diabetes mellitus was taken to a local ED 2 hours after sustaining a snakebite on the 5th finger of his left (dominant) hand. The patient reported that the bite lasted about 1 minute. VS: T 37.4°C, BP 103/69, HR 70, RR 14. On examination, 2 puncture wounds were observed on the distal phalanx with associated localized edema. The patient reported having pain up to the forearm, some paresthesias, but no focal motor deficit. He was treated with methylprednisolone IV, diphenhydramine, 25 mg IV, and cefazolin, 1 g IV. Laboratory studies revealed a blood sugar of 144 μg/dl and a WBC count of 15.3 × 103. The patient was transferred to a tertiary institution for a pediatric and surgical evaluation. He was observed for 8 hours, in which time, the edema improved; the patient received oral cefadroxil and was discharged. No follow-up was done.
Case #6
An 18-year-old man with no history of systemic illness was taken to a local ED 7 hours after sustaining a snakebite on the third finger of his right hand. The patient reported that the bite lasted about 3.5 to 4 minutes. VS: T 36.6°C, BP 113/79, HR 60, RR 14. Two puncture wounds were observed on the middle phalanx of the affected hand; associated localized ecchymosis and edema up to the elbow were also noted. The patient reported pain up to the biceps area, some paresthesia, but no focal motor deficit; he was treated with methylprednisolone, 125 mg IV, diphenhydramine, 50 mg IV, ketorolac and tetanus toxoid IM. Laboratory studies revealed a WBC count of 17.1 × 103. He was observed for 12 hours and then discharged on oral cefadroxil after a documented improvement of the edema. The patient returned to the ED for a follow-up appointment 72 hours after the episode. The examination revealed a slight decrease in both the edema and the paresthesia. In a follow-up phone call 2 weeks later, the patient confirmed that there had been a resolution of all symptoms 10 days after the event.
Discussion
Although popularly considered nonvenomous, some colubrids are at least mildly venomous, and a few can even cause human fatality. 5 Literature also presents the isolation of alfa-colubritoxin, a neurotoxin in some colubrids.6,7Alsophis portoricensis has been classified as having Duvernoy's gland secretions of intermediate venomous properties. This snake can become very aggressive when it senses danger, and it—much like the cobra—raises the ventral part of its body and expands the skin of its neck when it is ready to attack. Although Alsophis has no venom glands or venom-injecting apparatus, when its sharp teeth penetrate the skin and its saliva reaches the blood, a venomlike reaction follows, causing inflammation and pain. Two large teeth surrounded by a fleshy ridge in the rear of the upper maxillae appear to be modified for the administration of saliva. 3 ,8,9 Many colubrid snakes have Duvernoy glands, which discharge secretions to the base of posterior maxillary teeth.8,9 These glands are regarded as a characteristic unique to colubrid snakes. 1 According to Hegeman, Alsophis exhibits a degree of anatomical specialization that moves it in the direction of adaptation of the truly venomous species. 3 Based on the total protein content and the hyaluronidase, proteolytic, and hemolytic activities of Duvernoy's gland secretion, A portoricensis's venom can be classified as an intermediate between that of rattlesnakes and the harmless Nexis species. 8 ,10,11 The secretions also aid in the digestion of prey by immobilizing and slowly predigesting the food prior to swallowing. The release of venom is facilitated by repetitive mechanical jaw movements that the snake performs while maintaining a tight grip on its prey. These movements are not used for swallowing the prey, but presumably only for venom release.9,10 In contrast, lethally venomous snakes have complex and highly specialized mechanisms that enable them to deliver lethal doses of venom to their victims. Highly venomous snakes, such as crotalids, have frontal fangs specialized for injecting venom into their prey. 9 ,10,12
Many similarities can be found in the 6 cases presented. Most of the symptoms were localized to the affected extremity and included erythema, pain, and swelling and, systemically, nausea and vomiting. No permanent deficits resulted from the snake bites in any of the cases. Most of the patients reported a resolution of their symptoms within 2 weeks of the incident. It should be noted that the snake was attached to the bite site on the victims for extended—yet varying periods of time “1 to 4” minutes. Future research might ask whether the severity of symptoms correlates with the “venom-draining time” from the Duvernoy's glands. This case series poses an intriguing question regarding a bite from A portoricensis: Does the severity of the symptoms correlate with the duration (in minutes) of the bite? Since the venom apparatus is rudimentary, it would be reasonable to suspect that the duration of the bite could correlate with the severity of envenomation. The secretions from A portoricensis's Duvernoy's glands contain enzymes of intermediate activity compared to those found in crotalids. These enzymes cause localized pain, edema, and ecchymosis but lack the coagulopathic effects characteristic of many crotalid snake venoms.
In conclusion, A portoricensis can inflict a venomous bite causing painful local symptoms but without any serious sequelae or chronic complications. Although all of the patients' symptoms completely resolved over time, one has to consider the possibility of more serious symptoms developing (i.e., synovitis, cellulitis) if the bites are not treated properly. The severity of the bite depends on the ability of the snake to inject the victim with its secretions. In spite of previous popular belief, A portoricensis can inflict a venomous bite which, though not lethal, is far from harmless. In conclusion, although there have been very few documented snakebites on the island of PR, it is worth noting that emergency physicians should indeed take these bites seriously. Adequate follow up at fixed intervals until resolution of symptoms is obtained should be considered (i.e., 1, 3 days), as well as closer observation in the ED at the time of arrival up to 12 hours. Adequate pain control and immunization status should be addressed. More importantly, ED workers should appreciate that the bite of A portoricensis can produce a clinical envenomation under certain circumstances and proper caution should be practiced when treating patients bitten by this species.
Footnotes
Acknowledgments
The author wants to recognize Dr. Andres Britt Larregui, Director of the Puerto Rico Poison Center, for the photographs, his collaboration, and support.