
Abstract
Introduction
Snakebite envenomation is a significant life-threatening public health problem in Southeast Asia (SEA). In this region, India reported the largest number of snakebite deaths from 2000 to 2019 (1.2 million), with an average of 58,000 deaths yearly.
Methods
This prospective observational study was carried out among snakebite victims at the emergency department (ED) of a tertiary care public sector hospital in eastern India.
Results
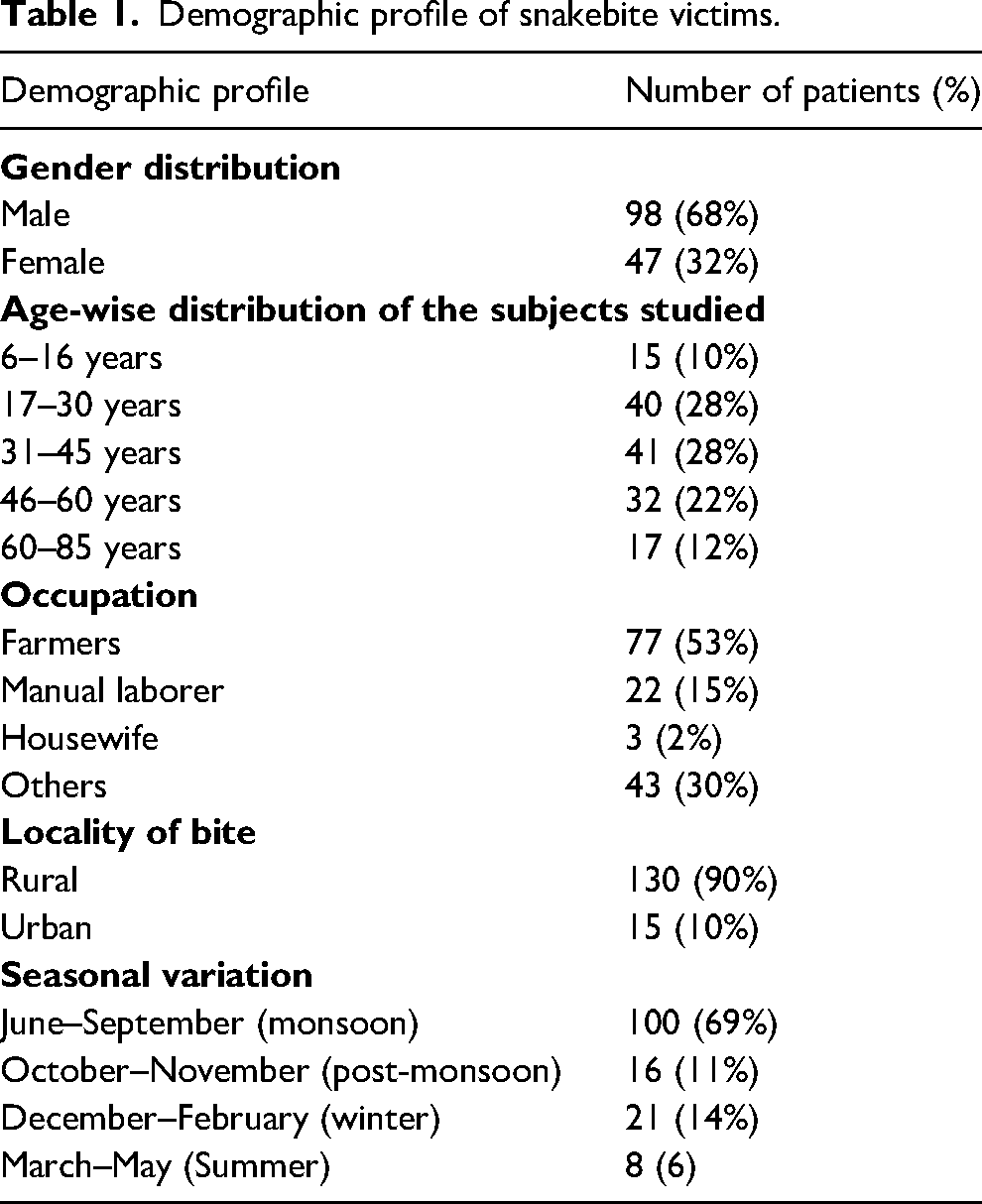
A total of 145 cases of venomous snakebite were investigated. More than half (n = 81, 56%) of the snakebite victims were between 17 to 45 years. Most of the snakebite victims were male (68%) and were farmers (53%) by occupation. The majority of snakebites occurred during the daytime (76%) and while outdoors (67%). Most victims sustained a bite on the lower extremity (71%). The peak incidence of snakebites occurred from June to September (69%). Three-quarters of all patients were unaware of the required first aid measures following a snakebite. Among the 145 venomous snakebites, 48 were presumptively identified as the Indian cobra, 32 by the Indian krait, 56 by the Russel's viper, and 9 by saw-scaled viper. The mean duration from the snakebite to the onset of systemic effects in the Indian cobra was 52 ± 14.28 min, 66 ± 18.35 min in the Indian krait, 42 ± 13.47 min in Russel's viper, and 48 ± 16.38 min in saw-scaled viper. Respiratory failure was the commonly observed complication following an elapid envenomation. The mortality rate was 2.1% among the patients treated with antivenom.
Conclusions
Snakebite is considered an occupational hazard in India, commonly affecting the young population in their productive period. The peak incidence was during monsoon season, and the majority had neurotoxic envenomation following an elapid bite (55%) that contributed to the increased mortality and morbidity among young adults. Of the 145 patients, the majority (84%) recovered fully with treatment; 16% of the victims developed morbidity viz cellulitis, respiratory failure, acute renal failure, compartment syndrome, local tissue necrosis, intracerebral hemorrhage, and disseminated intravascular coagulation. Appropriate first aid measures and timely medical intervention can significantly improve the treatment outcome following snakebites.
Introduction
Envenomation from snakebite is a significant public health problem in Southeast Asia (SEA), leading to substantial mortality and morbidity (WHO 2016). Among the SEA nations, India reported the largest number of snakebite deaths from 2000 to 2019 (1.2 million), with an average of 58,000 deaths annually. 1 Snakebite victims may endure lasting complications, including musculoskeletal deformities, contractures, impaired renal function, and psychological distress.1,2 In 2017, the World Health Organization (WHO) included snakebite envenoming (poisoning from snakebites) as an overlooked tropical disease requiring high priority. 3 Following this, in 2019, WHO launched a strategy for preventing and controlling snakebites to halve the mortality and morbidity associated with snakebites compared to the 2015 baseline. 4 However, achieving this target would mandate considerable progress in India, which is home to approximately half of the global snakebite mortality cases. 5
Snakebites are reported to be an occupational hazard in India, where farmers, plantation workers, and fishermen become the most common victims, with the envenomation typically occurring while working in the fields and in outdoor activities without appropriate footwear. 6 Indian cobra (Naja naja), Indian krait (Bungarus caeruleus), Russell's viper (Daboia russelii), and saw-scaled viper (Echis carinatus) are the major venomous snakes in India, together known as the “Big Four.” The envenomation by Indian cobra and Indian krait may lead to neurotoxicity, whereas the other two may cause hemotoxicity. The symptom presentation is largely dose dependent. Although anti-snake venom (ASV) remains the mainstay of treatment, most snakebites in rural and tribal areas are managed by traditional faith healers. 7 The practice of unproven traditional methods, inadequate knowledge about snakes, and delayed transportation to a definitive treatment center have potentially increased the mortality rates associated with snakebite envenoming.8,9
Although most of the mortality associated with snakebite envenomation could be prevented, misconceptions and faulty treatment strategies significantly antagonize the progress made in snakebite management. Odisha is a tribal-dominated state in the eastern Indian peninsula, having a thick forest coverage of 37.4% of its land area. It is recognized to be a high-burden state for snakebite mortality in India. 10 Earlier reports highlighted a north-south divide in snakebite envenomation in India regarding the symptom profile and hospital presentation. 11 However, there exists limited data on the clinical and epidemiological patterns of snakebite victims in this part of the country. Hence, the present study was undertaken to investigate the clinical and epidemiological profile and the health-related outcomes of snakebite victims admitted to a tertiary care hospital in eastern India over 1 y.
Methods
This prospective observational study was carried out at the emergency department (ED) of All India Institute of Medical Sciences (AIIMS) in Bhubaneswar, India. This medical center is a tertiary care public hospital in eastern India, which is also the referral center for patients from neighboring states. All snakebite victims admitted to the hospital from June 1, 2021, through May 31, 2022, were advised of the purpose of the study, and informed consent was sought. The patients or their primary caregivers were interviewed in the hospital's ED after the initial stabilization of the patient. The patients who left against medical advice, those who presented to the hospital already deceased, and those who were unwilling to participate in the study were excluded. The information pertaining to the victims’ age, gender, and occupation; locality of the snakebite; date and time of the bite; time of hospital presentation; type of snake; information about any primary treatment provided to the victim; awareness about the first aid measures; the first point of contact; mode of transport and clinical variables such as the site of the bite; local and systemic symptoms; any complications, investigations, treatment given, and duration of hospital stay along with outcome was recorded. The data about previous treatment, including ASV and the number of centers, the reason for the delay in presentation, if any, and the treatment received in the hospital, including critical care support, ED procedures, and the complication developed after envenomation during the course of treatment, were also recorded. The outcome was recorded as recovered, partially recovered with morbidity, and expired. The data was collected on a pre-prepared structured document.
Ethics Statement
The Institutional Ethics Committee approval was obtained before the commencement of the study (IEC No T/IM-NF/Nursing/19/90), and written informed consent was obtained from all the participants. The authors attest that the manuscript adheres to the standards of Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines for reporting observational studies.
Statistical Analysis
The collected data were entered into a Microsoft Excel sheet and analyzed using Statistical Package for Social Sciences (SPSS version 21). Data analysis was carried out after entering the coded information, and tables were generated. The categorical variables are expressed as counts and percentages. The continuous variables are expressed as mean ± SD.
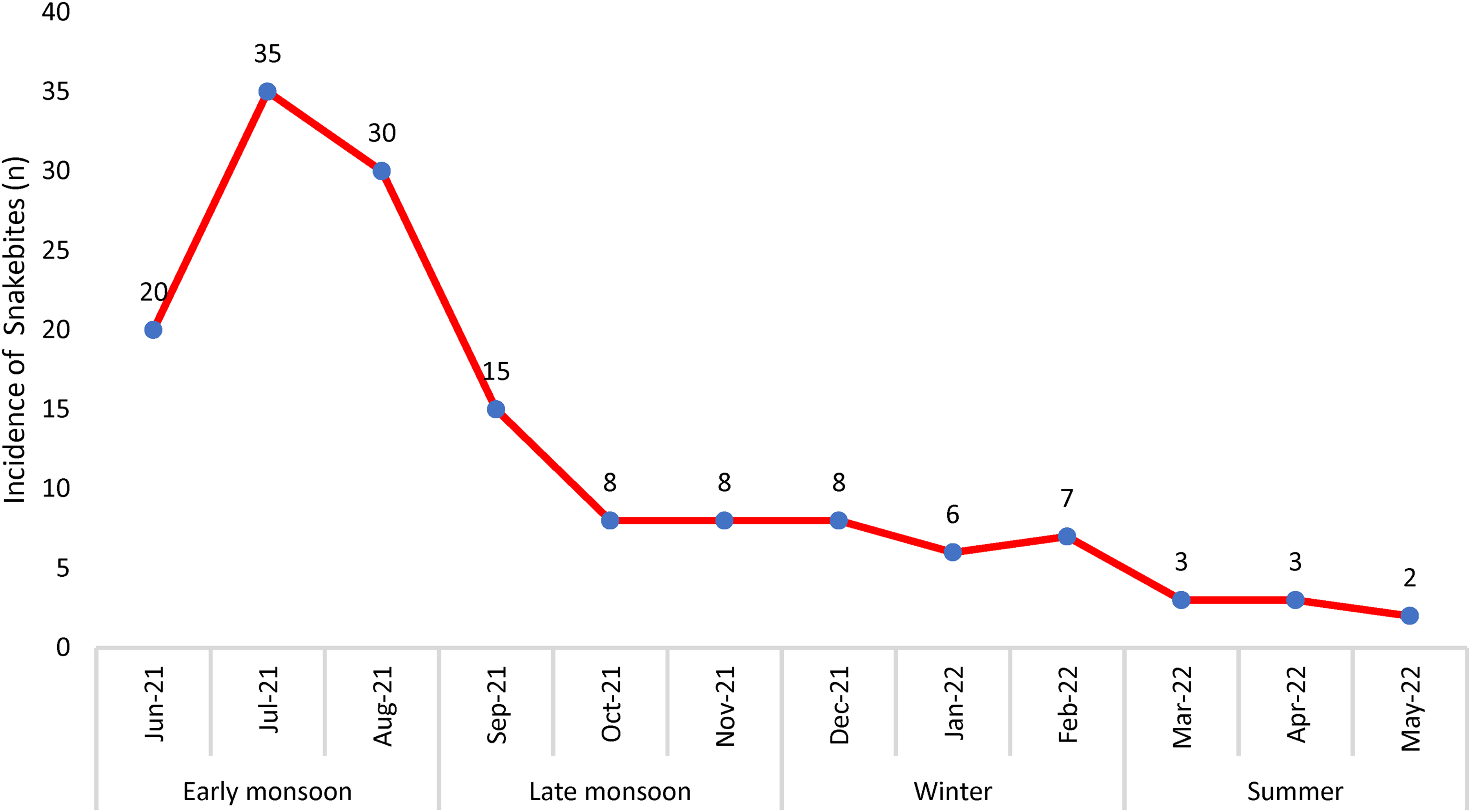
Incidence of snakebite according to season.
Results
A total of 145 venomous snakebite victims were included in the study for final analysis. More than half (n = 81, 56%) of the snakebite victims were between 17 to 45 years. The mean age of the victims was 38.65 ± 17.67 years (range 6 to 85 years). The detailed demographic profile of the snakebite victims is presented in Table 1. Most of the snakebite victims were male (68%). The majority of the bites (n = 110, 76%) occurred during the daytime, while the other 35 bites (24%) occurred after sunset (between 1800 h to 0600 h). More than half of the snakebite victims were farmers (53%), and the peak incidence of snakebites occurred from June to September (n = 100, 69%) (Figure 1). Of the 145 patients, 9 (6%) did not receive a formal education. Most victims (n = 97, 67%) sustained the bite outdoors. Most of the snakebites (90%) occurred in rural areas, and the most frequently bitten site was the lower extremity (71%) (Figure 2). Three victims approached a traditional healer, 1 sought Ayurveda treatment, and the other 141 victims sought treatment from the hospital immediately after the snakebite (Table 2). The majority of the victims (n = 109, 75%) were unaware of the first aid measures to be followed in a snakebite.
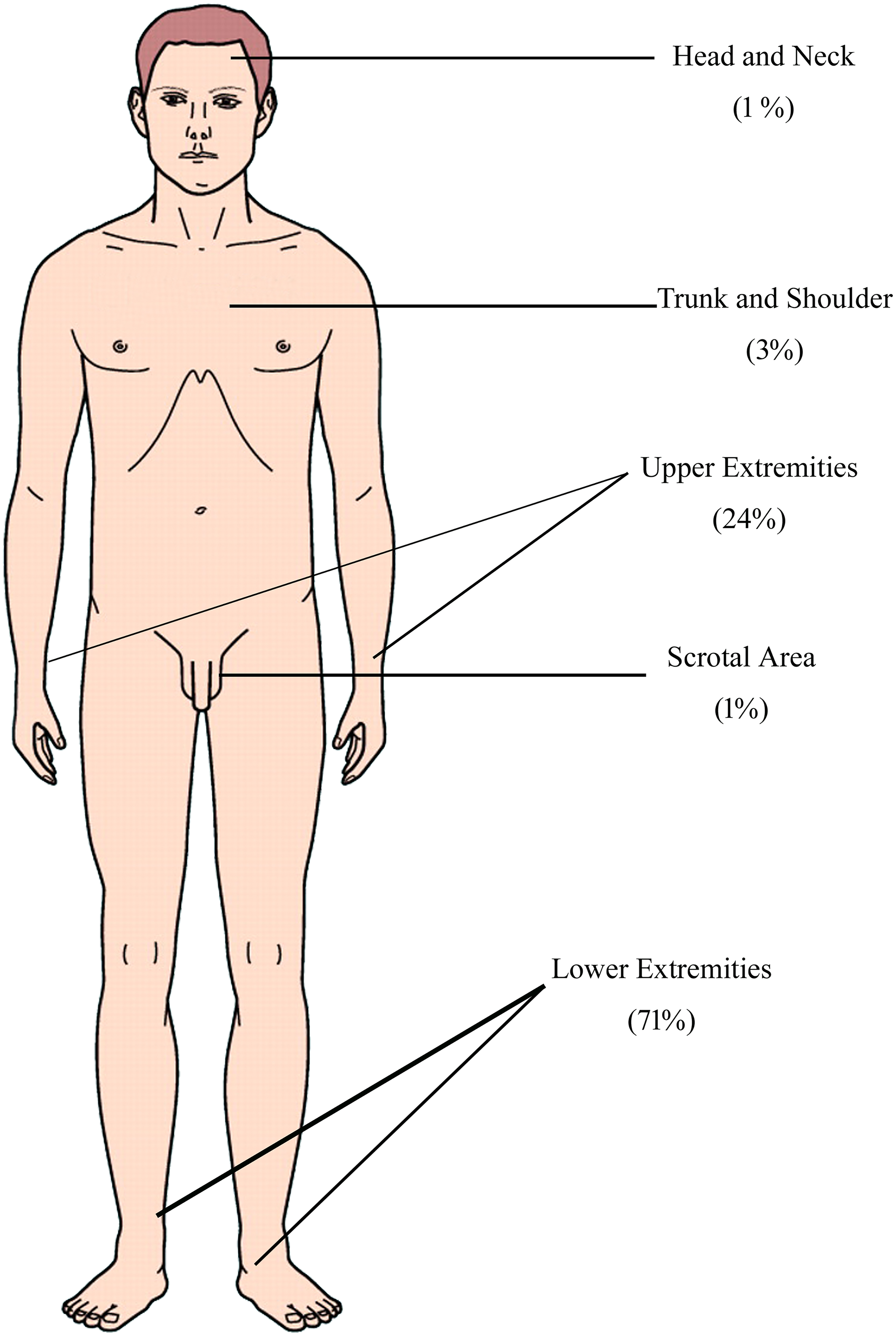
Percentage distribution of snakebite site among the victims.
Demographic profile of snakebite victims.
The time duration between the incidence of snakebite and hospital admission.
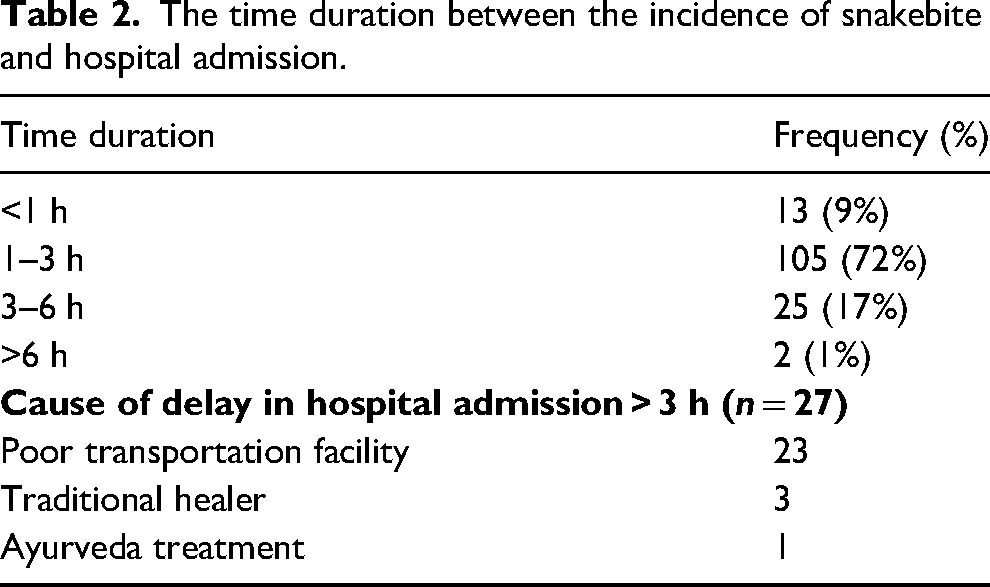
Ninety-seven (67%) patients utilized an ambulance for transport to the hospital, whereas the remaining 48 (33%) used a private vehicle to reach the hospital. Almost 95% of victims (n = 138) had a definitive fang mark over the bitten area. The whole blood clotting test (WBCT) was negative in 61% of the victims (n = 88), while blood was not clotted in the other 57 patients (39%). Only 9% (n = 13) of the victims reached the hospital within 1 h of the bite (Table 2). The mean (±SD) time duration between snakebite to needle time was 3.01 ± 1.35 h with a range of 1–8 h. A poor transportation facility was the most common cause of delay in seeking hospital treatment (Table 2). Even though most people were unaware of first-aid measures following a snakebite (75%), they tried to attempt some measures following the bite to eliminate the venom's effect. Various measures tried were the application of a tourniquet (n = 50, 35%), squeezing of the bitten site (n = 60, 41%), and application of an herbal medicine (n = 5, 3%). However, 30 victims (21%) did not attempt any first aid measures following a snakebite.
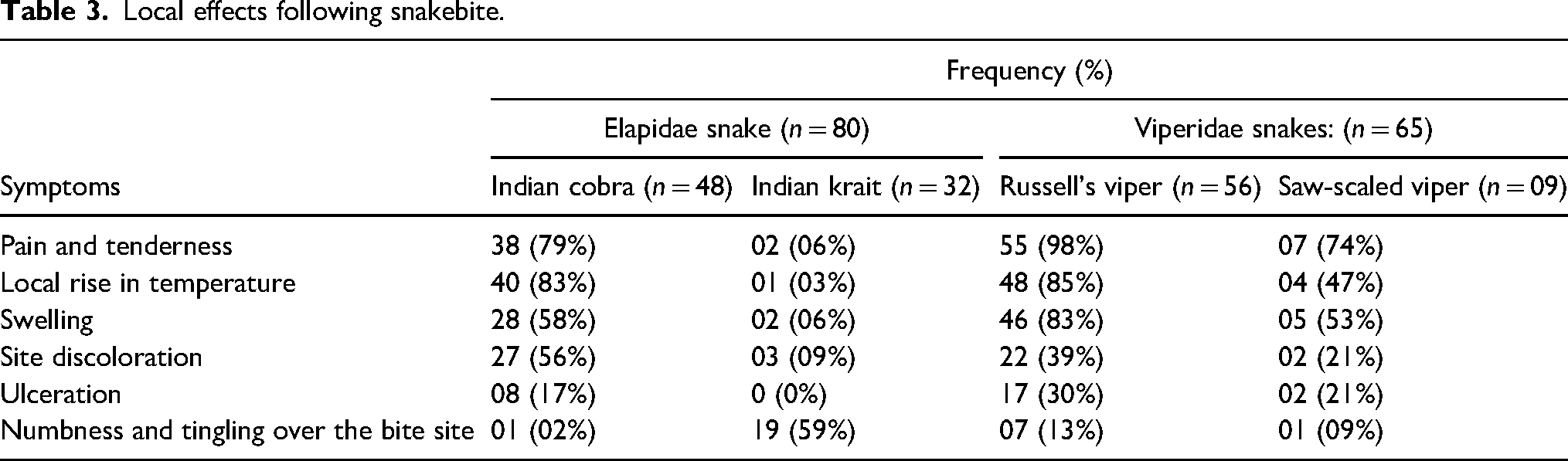
Of the 145 cases of snakebite, 48 victims were believed to be bitten by an Indian cobra, 32 by an Indian krait, 56 by Russel’s viper, and 9 by a saw-scaled viper (Figure 3). The most commonly reported local manifestations were pain and tenderness (70%) over the bitten site. The commonly reported systemic symptoms among victims of snakebite are depicted in Figure 4a and b. The mean duration of onset of systemic symptoms after a bite by the Indian cobra was 52 ± 14.28 min, with a range of 45 to 90 min. The initial systemic symptoms reported were vomiting, dizziness, generalized tiredness, ptosis, abdominal pain, perioral numbness, and dysphagia (Figure 4a). Almost all the patients reported severe local reactions after the initial symptoms (Table 3). The mean time duration from Indian krait bite to the onset of systemic symptoms was 66 ± 18.35 min (range 60–160 min). The earliest systemic symptoms reported were numbness and tingling of the extremities, generalized tiredness, ptosis, perioral numbness, dysphagia, dizziness, and ophthalmoplegia (Figure 4a). There were minimal local symptoms. The mean duration from Russel's viper bite to the onset of systemic symptoms was 42 ± 13.47 min, ranging from 30 to 90 min. The antecedent symptoms reported were nausea, vomiting, head reeling, abdominal pain, dizziness, and bleeding manifestations (Figure 4b). Most of the patients developed severe local reactions following the bite (Table 3). The mean duration of systemic symptom onset after a saw-scaled viper bite was 48 ± 16.38 min (range 45 to 120 min). The initial systemic symptoms reported were nausea, vomiting, head reeling, abdominal pain, and dizziness (Figure 4b). The patients also reported moderate local reactions (Table 3).
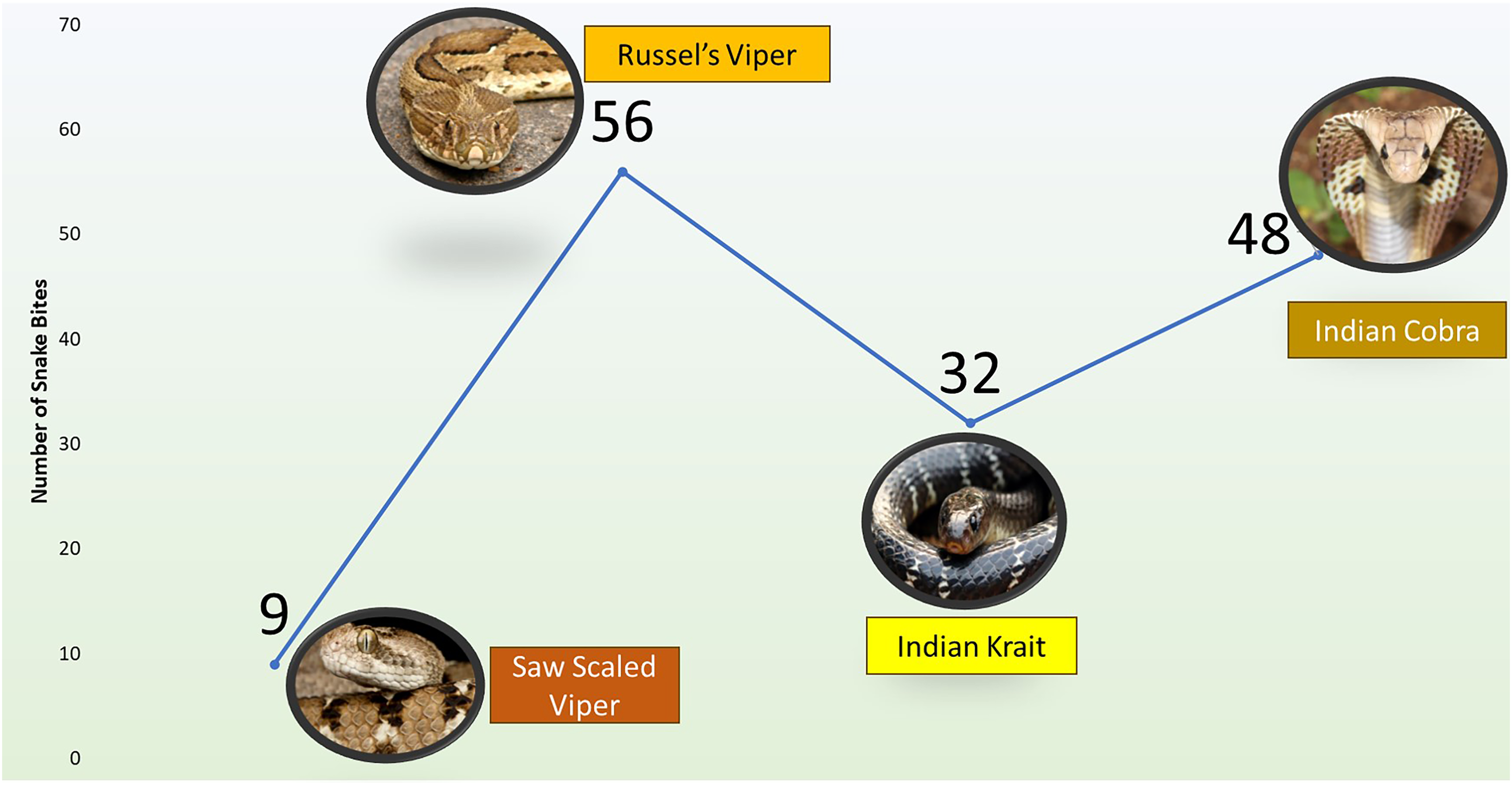
Incidence of snakebite according to the species.
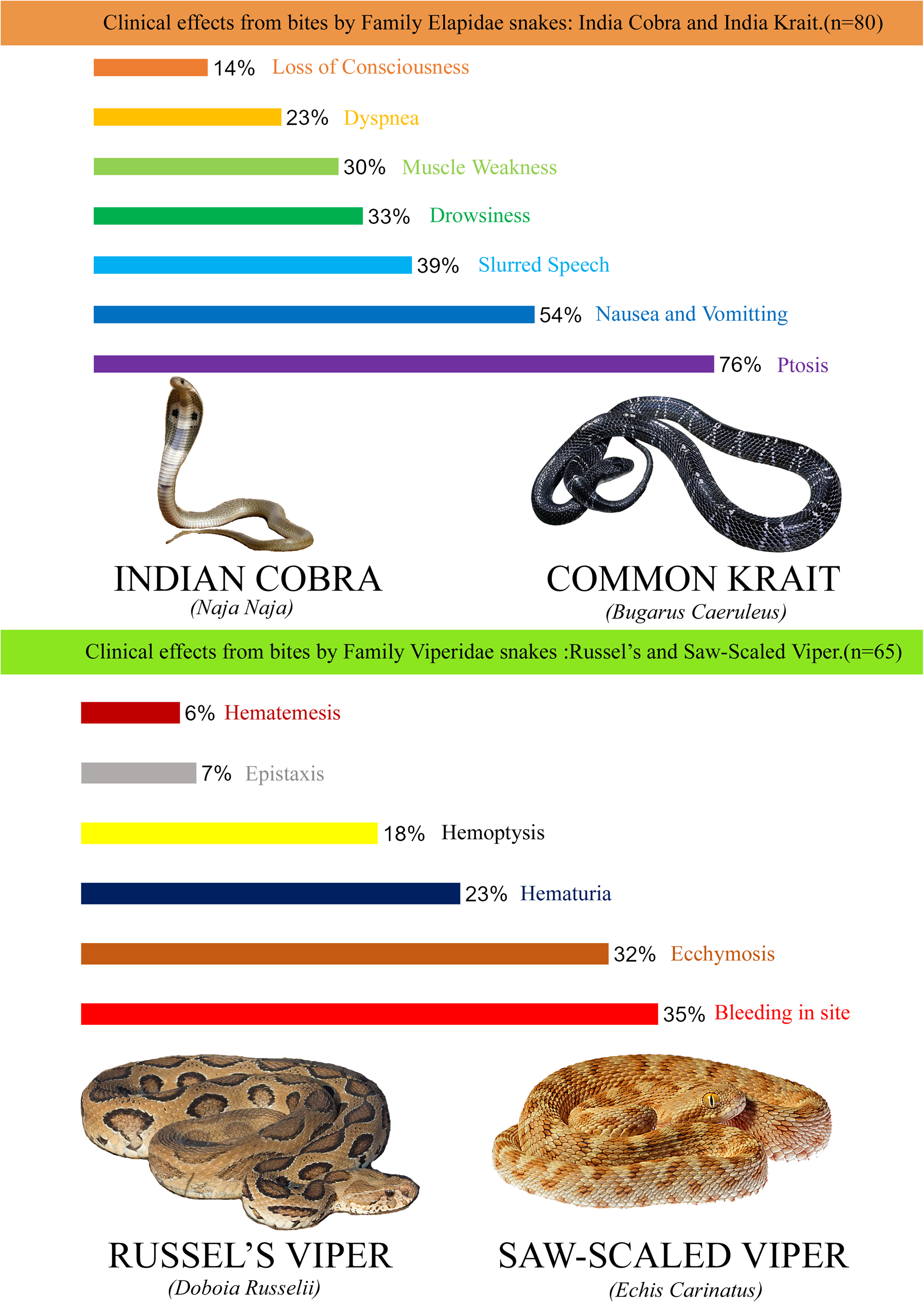
Clinical effects from bites by families Elapidae and Viperidae snakes.
Local effects following snakebite.
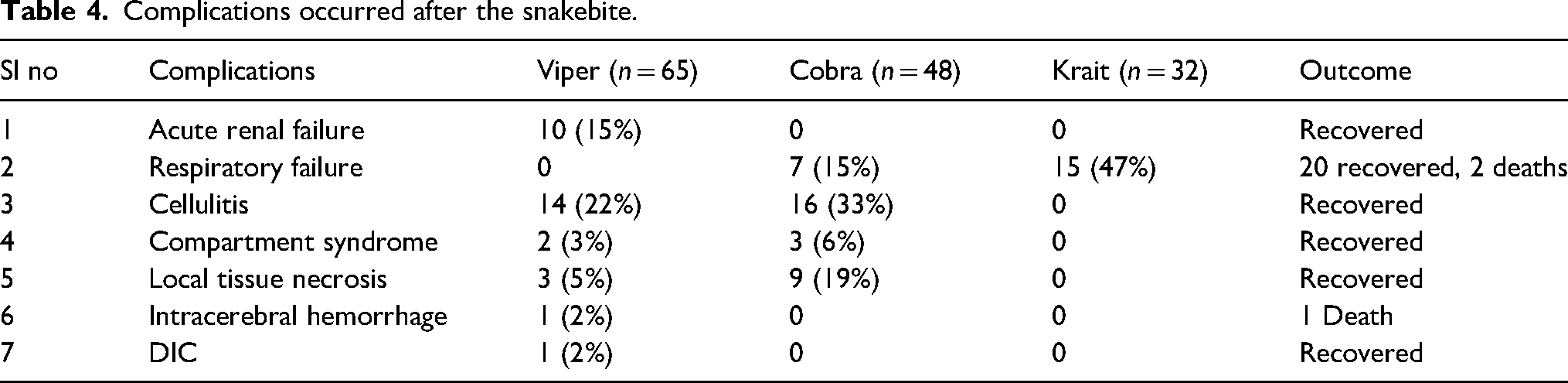
All the venomous snakebites were treated with equine polyvalent anti-snake venom (ASV) BENOMTM, manufactured by Biological E. Limited, Telangana, India. The mean dose of ASV received by Elapid bite victims was 16.77 vials (range 3-40), and those with Viperidae bite was 18.49 vials (range 5–40). Allergic reactions to ASV were observed in 6 (4%) victims (4 elapid bite victims and 2 Viperidae bite victims), which were symptomatically managed. Four patients developed urticaria, and 2 patients developed flushing that was symptomatically treated with antihistamines and steroids. None of the victims developed an anaphylaxis reaction. Among the 80 elapid snakebites, 22 (15%) victims developed respiratory failure and required rapid sequence intubation and mechanical ventilation (Table 4) during the course of ED treatment. Sixteen patients developed cellulitis, out of which 2 developed compartment syndrome, which required fasciotomy. Of the 65 Viperidae snakebite cases, 10 patients (7%) developed acute renal failure (ARF), out of which 6 were managed by hemodialysis and 4 were managed conservatively. Fourteen patients developed cellulitis, out of which 3 patients developed compartment syndrome, which was managed with fasciotomy. Among study participants, 3 patients (2 after a krait bite and one after Russel's viper bite) died during the course of treatment, contributing toward an overall mortality rate of 2.1%. The patients who were treated appropriately with ASV within 6 hours of the snakebite survived.
Complications occurred after the snakebite.
Two patients with krait bite presented to our ED after 7 h of envenomation in an unresponsive state. Cardiopulmonary resuscitation (CPR) was given to those patients for 30 min to 1 h, determined by the individual's clinical condition and the clinician's discretion regarding the continuation or cessation of CPR. Throughout this process, all patients underwent immediate intubation within 5 min of commencing CPR. All these patients received adrenaline, ASV, and additional drugs during resuscitation depending on blood gas parameters. Even though these patients achieved return of spontaneous circulation (ROSC) after 5 cycles of CPR, they were hemodynamically unstable. Furthermore, these individuals exhibited severe metabolic acidosis (with a pH below 7) and hypotension. In an attempt to address their condition, sodium bicarbonate infusion was administered alongside noradrenaline and adrenaline IV infusions and adequate intravenous fluid replacement. Unfortunately, despite these interventions, both patients experienced cardiac arrest and succumbed to death within 2 h of ED presentation. Another patient with Russel's viper bite presented to our ED after 32 h of envenomation with complaints of oliguria, petechiae, altered sensorium, and swelling over the bite site. Blood investigation revealed elevated creatinine level, hyperkalemia, elevated prothrombin time (PT), elevated international normalized ratio (INR), and the computerized tomography scan revealed intracerebral hemorrhage. The patient was managed symptomatically, including ASV, rapid sequence intubation, mechanical ventilation, and other supportive measures. However, the patient developed cardiac arrest and succumbed to death within 3 h of ED presentation. The complications reported in our study are illustrated in Table 4. The common complications reported were cellulitis (21%); respiratory failure (15%), which was followed by ARF (7%); and compartment syndrome (3%). The patients with respiratory failure were managed with endotracheal intubation and mechanical ventilation, injections of atropine (0.6 mg) and neostigmine (1.5 mg stat), followed by neostigmine 0.5 mg with atropine 0.6 mg for 5 doses repeated every 30 min. Of the 22 patients with respiratory failure (7 cobra and 13 krait), 8 patients shifted to ICU, 12 patients were treated in ED due to the unavailability of ICU beds, out of which 20 recovered, and 2 succumbed to death. Out of the 10 patients with ARF, 6 patients required hemodialysis, and others were managed by conservative measures, including ASV. All 30 patients with cellulitis were managed with broad-spectrum antibiotics and glycerin magnesium sulfate dressing, out of which 5 patients developed compartment syndrome requiring fasciotomy. One patient with DIC was managed with ASV, fresh frozen plasma, platelet-rich plasma transfusion, and other symptomatic management measures.
Discussion
The WHO designated envenomation by snakebite as a neglected tropical disease in 2017. 12 In India, the eastern state of Odisha lies on the coast of the Bay of Bengal and is considered the third snakebite-prone state in India, with a proportional mortality rate of 5.2 per 1000 snakebites. 13 The factors contributing to this increased prevalence are (i) the 4 most common varieties of poisonous snakes (kraits, Russell's vipers, saw-scaled vipers, and cobras) are found frequently in Odisha; (ii) some snakes won’t cause much pain when biting a human, potentially resulting in delayed recognition of the envenomation; and (iii) the delay in reaching a health care facility after the envenomation. 13 In India, the commonly found poisonous snakes of the elapid family are Indian cobra and krait, whereas those found in the Viperidae family are Russell's viper and the saw-scaled viper. An elapid envenomation paralyzes the limb-girdle, bulbar, and eye muscles, whereas bleeding from the mucocutaneous sites, hemolysis, acute kidney injury, and shock can occur after a viper bite. The present study attempts to determine the clinical and epidemiologic profile and health-related outcome of patients with a snakebite over 1 year.
The male predominance of snakebite victims in this study might be due to males’ intensified involvement in outdoor activities as compared to females’. A similar finding was observed in other studies.14,15 The younger population (21–40 years) was often affected, possibly due to their more ambulant nature. 16
Farmers (53%) and manual laborers (15%) constituted most of the snakebite victims, reiterating that snakebite is an occupational hazard in India. They have to work in the field, usually barefoot, and this might contribute to the increased incidence of snakebites. The finding is congruent with the study results of Halesha et al. 16 In the present study, snakebites predominantly occurred in rural areas (90%) and outside the home environment (67%). Many studies from India and other SEA nations also support this finding.17–20
The present study reported an incidence of 69% snakebites from June to September (Figure 2), which is the monsoon period in Eastern India. The flooding can wash away the snakes to lowlands, where there is an increased population density. 21 The habitats of snakes and their prey can become flooded during monsoon season. Moreover, the natural prey of snakes like frogs, rats, and mice may relocate toward the proximity of the human environment in monsoon season. Snakes in search of their prey may be encountered by humans, and a bite can occur. 16 A study by Kulkarni et al 22 reported 67% of snakebite incidence during monsoons in Southern India, which is similar to our findings. In contrast, a study from Iran reported an increased incidence of snakebites during summer. 23 The majority of the bites occurred in a rural area (90%) and outside the home (67%).
Most victims (78%) received some kind of first aid after the snakebite. Applying a tourniquet, squeezing the bite site, and using herbal medicines were the adopted first aid measures, irrespective of the species identified. These findings are similar to the study reports from southern India. 16 Unfortunately, none of these first aid measures were recommended for treating snakebites since they may cause more harm than good and may also delay seeking appropriate treatment measures. 24 Moreover, none of the subjects practiced the first aid measures recommended by WHO. The general first aid measures recommended by WHO for all species of snakebite are (i) reassurance of the anxious victim, which will reduce the patient's heart rate and slow down systemic spread of the venom; (ii) immobilizing the entire patient's body by making him lay down in a safe and comfortable position, ideally in a recovery position to reduce the chance of aspiration followed by vomiting, and immobilizing the bitten part with a splint or sling; and (iii) to avoid interfering the bite wound via incisions, rubbing, vigorous cleaning, massage, or herbal application as it may lead to infection. The first aid measures to be followed after an elapid bite, according to WHO, are pressure-immobilization methods to prevent the quick progression of life-threatening respiratory paralysis. With prompt use of pressure immobilization methods like pressure-pad immobilization or pressure-bandage plus immobilization, respiratory paralysis may be delayed by reducing the speed of absorption of venom from the bite site. 25 The fact that none of the recommended first aid measures were followed here indicates the importance of training the members of the public regarding common first aid measures to follow in a snakebite.
The mean duration from snake envenomation to the onset of systemic signs and symptoms after elapid bite was 59 ± 16.32 min (52 ± 14.28 min in the cobra bite and 66 ± 18.35 min in the krait bite). The duration of symptom onset and its severity largely depends on the type of bite and the amount of venom injected. The elapid venom causes significant neurotoxicity. Paralysis is initially identified as ptosis and ophthalmoplegia, starting within 15 min after envenomation. Descending paralysis is usually observed, which progresses as paralysis of the face, palate, jaws, tongue, vocal cords, and neck muscles. Obstruction of the airway, intercostal muscle, and diaphragmatic paralysis may lead to respiratory failure. The neurotoxins do not cross the blood-brain barrier. With timely administration of ASV, the neurotoxic effects can completely be reverted. 26 The mean duration from bite to onset of systemic signs and symptoms following a Viperidae bite was 45 ± 42.5 min in our study (42 ± 13.47 min and 48 ± 16.38 min in Russell's viper and saw-scaled viper, respectively). Hemostatic abnormalities are a hallmark of Viperidae envenomation. Continuous bleeding from the bite site may be the initial local manifestation noted. Hematemesis, hemoptysis, epistaxis, ecchymosis, and intracranial hemorrhage point toward a systemic envenomation. 26 A similar study reported the time of onset of clinical envenomation within 1 h of a snakebite. 27
In the present study, 18% of patients reported to the hospital 3 h after a snakebite. A similar study from South India reported that nearly 39% of their patients sought treatment 6 h after a snakebite, which differed from our study finding. 16 The arrival delay was attributed to the lack of appropriate transportation facilities, lack of knowledge about the hazards of snakebite, and the victims’ ignorance.
The present study reported that 55% of the victims had envenomation by elapids and 45% by Viperidae. The findings corroborate with that of Singh et al, who reported more neurotoxic symptoms with elapid bite than hemotoxic symptoms by Viperidae bite in their victims from eastern India. 28 The increased incidence of elapid envenomation is due to the increased existence of these snakes in the geographic regions studied. 29 The most common systemic effects of envenomation following elapid bite was ptosis (76%), which was followed by nausea and vomiting (54%), drowsiness (33%), muscle weakness (30%), and dyspnea (23%). Two Sri Lankan studies reported that the incidence of ptosis ranged from 70–85%, muscle weakness in 27–54% of cases, and dyspnea in 18–45% after neurotoxic snake envenomation.30,31 The venom of the elapids is abundant in phospholipase A2 and other similar proteins, which affect neuromuscular transmission adversely in either presynaptic or postsynaptic levels. The presynaptic neurotoxins, called beta neurotoxins, block acetylcholine release, whereas post-synaptic neurotoxins, known as alpha neurotoxins, block acetylcholine receptors reversibly. This explains the predominant incidence of ptosis following an elapid snakebite. 32 Bleeding from the bite site was the most common manifestation (54%) after a Viperidae bite. This was followed by ecchymosis, hematuria, hemoptysis, and epistaxis. This finding is similar to the study results of B. D. Sharma. 33 Bleeding from the bite site after a Viperidae bite is due to the action of snake venom serine protease (SVSP). SVSP is a thrombin-like enzyme that has a fibrinogenolytic function. The snake venom metalloproteinases (SVMP) toxins also cause the degradation of capillary basement membranes by enhancing the vascular permeability of blood vessels. This may result in extravasation and contribute to hemorrhagic activities. 34
A WBCT was carried out in all the patients who had a history of snakebite. It is a simple coagulation test performed in assessing, diagnosing, and therapeutic monitoring of snakebite patients. If the blood fails to coagulate after 20 min of collection in a dry glass tube, it indicates a coagulopathy. 35 In this study, 48% of the samples didn’t coagulate, suggesting a viper bite. In contrast, other studies from India reported a higher incidence of hemotoxic snakebites.36,37
The definitive and reliable treatment available for snakebite envenomation is ASV. In India, the currently available ASV is polyvalent. The venoms of Big Four venomous snakes—that is, Indian cobra (Naja naja), Indian krait (Bungarus caeruleus), Russell's viper (Daboia russelii), and saw-scaled viper (Echis carinatus)—are used in the development of polyvalent ASV. 38 Our hospital uses polyvalent anti-snake venom (ASV) supplied under the name of BENOMTM. Each ml of this polyvalent ASV neutralizes 0.6. mg cobra venom, 0.45 mg krait venom, 0.60 mg Russell's viper venom, and 0.45 mg saw-scaled viper venom. 39 It is a lyophilized, polyvalent, enzyme-refined equine (Fab) immunoglobulin that is to be reconstituted with 10 mL sterile water supplied along with the combi pack. Monovalent ASV is not presently available in India because of the lack of objective means of identifying snake species in the absence of a dead snake. It would not be possible to determine the exact monovalent ASV to be used in the treatment of patients. 40 The mean dose of polyvalent ASV administered in Viperidae and the elapid bite was 18.49 and 16.77 vials, respectively. The mean dose of ASV used in various studies ranges from 7 to 21 vials depending on the snakebite's severity and treatment response.16,41,42 The present study reported a 4% incidence of allergic reactions after ASV administration. A few studies reported more than 10% of allergic reactions after an ASV administration.16,20 Meticulous monitoring is necessary to identify any early manifestations of allergic reactions. Prophylactic administration of hydrocortisone and pheniramine maleate may reduce the incidence of allergic reactions.
Our incidence of complications, including cellulitis, respiratory failure, DIC, ARF, and compartment syndrome, was similar to that reported by Halesha et al. 16
The present study reported a mortality rate of 2.5% after an elapid bite and 1.5% after Viperidae bite. The reported mortality rates after a snakebite differ across various studies ranging from 3% to 10%.10,43 Higher mortality in the Indian population is due to the increased prevalence of the rural population engaged in agricultural and other field activities where early transportation and treatment facilities are suboptimal. Compared to similar studies, the reduced mortality rate reported in the present study is attributed to the fact that most victims approached health care facilities for treatment in comparably less time.
Limitations
The present study was done in a single tertiary care hospital. Since snakebite warrants emergency management, many victims may initially be treated at local hospitals or primary health centers. If treated uneventfully, they may not be referred to higher centers. This may lead to unclear morbidity status estimation after a snakebite. The long-term follow-up data regarding the snakebite victims were not elucidated in the present study, which could reflect the exact morbidity and mortality status after the snakebites.
Conclusions
Snakebite is considered an occupational hazard in India, commonly affecting young male farmers from rural areas. The incidence of snakebites was higher during monsoon season. Lower extremities are a common site of snakebites, and more than half of victims sustained bites from elapids. Most victims were unaware of the first aid measures to follow after a snakebite. Early immobilization, timely transport to the hospital, and ASV administration can substantially reduce the mortality and morbidity associated with a snakebite. Timely administration of ASV is crucial for snakebite treatment. Our study reported a low incidence of death in patients who received ASV. Interestingly, no death was reported for patients who received ASV within 6 hours of the bite. Hence, the public must be educated and trained regarding adequate first aid measures and accessing treatment quickly after a snakebite to improve the patient outcome.
Footnotes
Acknowledgments
The authors thank Mr Azhar SM and Mr Siby YS, All India Institute of Medical Sciences (AIIMS), Bhubaneswar, for their assistance in this study.
Author Contribution(s)
Declaration of Conflicting Interests
The authors have no potential conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.