
Abstract
Introduction
Daboia palestinae is the most common venomous snake in Israel. In most cases, snakebite does not develop into a systemic disease. Since the introduction of specific antivenom therapy, the mortality rate has declined sharply. Nevertheless, there is still no uniform therapeutic protocol in Israel for patients who have been envenomated, and there is no current data regarding latency of symptom development. We aimed to evaluate the latency of symptom development after D palaestinae snakebite in patients presenting to the emergency department (ED) with local reaction.
Methods
This was a retrospective single-center study of all patients who presented following a snakebite from 2015 to 2020. Patients with confirmed or suspected D palaestinae bite were included. Demographical and clinical data were extracted from each electronical medical record and subjected to descriptive and comparative analysis.
Results
Sixty-two patients met the inclusion criteria. Their median (IQR) age was 30 (17–48) y, and 75% were male. Forty-one percent presented with local reactions to the snakebite, 29% presented with advanced local reaction, and 29% presented with systemic symptoms. Antivenom was given to 22% of patients with advanced local reaction and 89% of patients with systemic reaction. The median (IQR) time from bite to antivenom and from ED arrival to antivenom were 2 (1.5–2.5) h and 1 (0.75–1.5) h, respectively. Antivenom was administered at the latest 3.5 h after presentation to the ED for progression of local symptoms.
Conclusions
Our study may support a 4- to 6-h observation period in the ED for patients with mild clinical presentation after D palaestinae bite. Further larger prospective studies are needed.
Introduction
In Israel there are 3 venomous snake families with 8 different species: Viperidae (Montivipera bornmulleri, Cerastes vipera, Daboia palaestinae, Echis coloratus, Cerastes gasperettii, Pseudocerastes fieldi), Atractaspididae (Atractaspis engaddensis), and Elapidae (Walterinnesia aegyptia). 1 D palestinae is the most common among them, accounting for 100 to 300 reported cases of envenomation in adults and children every year. 2
D palestinae venom is composed of neurotoxins, hemorrhagins, angioneurin growth factors, and different types of integrin inhibitors. 3 These enzymes can cause local and systemic manifestations. In most cases, the snakebite does not cause systemic manifestations and is limited to local symptoms. The most common local tissue reaction includes pain and edema, while the most common systemic reactions include abdominal pain, nausea and vomiting, tachycardia, and hypotension. 4 -8 However, gastrointestinal symptoms may reflect nonspecific symptoms present in medically insignificant snakebite as well. Snakebite presentations are usually classified based on local and systemic findings. Local symptoms can be further classified based on the distance from the snakebite (simple vs advanced), and systemic symptoms can be classified as mild moderate or severe based on the treating physician’s judgment. 4 There are other classifications, also based on the clinical severity at the time of presentation 5 : mild, only local involvement confined to the site of the bite; moderate, systemic manifestations of gastrointestinal involvement; and severe, patients admitted with hemodynamic shock (systolic blood pressure <fifth percentile for age). Since the introduction of specific antivenom therapy, the mortality rate has declined sharply from 6 to 10% to 0.5 to 2%. 3 Nevertheless, there is still no uniform therapeutic protocol in Israel for patients who have been envenomated, and particularly for envenomated children. 6 It has been suggested that patients with systemic manifestations and progressive local signs be treated with the specific antivenom,7,9-11 although a recent local study suggests antivenom treatment for only moderate or severe systemic reactions. 4
There is no current data regarding latency of symptom development after D palestinae bite. Some authors suggest admission to the hospital for 72 h regardless of the severity of initial symptoms, with observation in the intensive care unit for the first 48 h. 8 Others suggest 6 h of surveillance for children with mild clinical presentation. 6
In our study, we aimed to evaluate the latency of symptom development after D palestinae snakebite in patients presenting to the emergency department (ED) with local reaction or no symptoms.
Methods
This was a retrospective single-center study of all patients who presented to Ha’emek Medical Center ED following a snakebite between 2015 and 2020. Ha’emek Medical Center is a regional hospital serving northeastern Israel, with 110,000 annual presentations distributed among separate EDs (87,000 to the general ED and 23,000 to the pediatric ED).
All patients with an ICD-9 discharge diagnosis of “Venomous snakes and lizards causing poisoning and toxic reaction” and “Bite of nonvenomous snakes and lizards” (E905.0, E906.2) were extracted from the electronical medical records.
After chart review, only patients with confirmed or suspected D palestinae bite were included. Diagnosis of D palestinae bite was made based on the snake itself, brought in alive or dead, a photo, or confirmed by individuals familiar with local snakes. Suspicion of D palestinae bite was based on geographical distribution of the snake and clinical findings.
Each chart was reviewed for the date and time of bite, age, sex, time of presentation to the hospital, time of antivenom administration, length of stay (LOS) in the ED, disposition, hospitalization time, clinical signs and symptoms on presentation and during hospitalization, complication evaluation and management, follow-up in the wards, and return visits to the ED after discharge from the hospital.
Snakebite presentations were classified based on the clinical presentation on admission: local, involvement confined to the site of the bite (eg, swelling, pain, discoloration, ecchymosis); local advanced (rapid extension of swelling, enlarged tender lymph node draining the bitten limb, swelling involving more than half the bitten limb or more than 1 joint); and systemic (eg, gastrointestinal, cardiovascular, central nervous system, hematological). 11
Indications for treatment with D palestinae–specific antivenom (Kamada, Israel) were rapid progression of local signs proximal to the site of the bite and systemic manifestations such as circulatory shock or gastrointestinal symptoms.2,5 The antivenom currently used is a monovalent whole immunoglobulin. Since 2012, it has been produced by Kamada, Beit-Kama, using good manufacturing practice, according to the methods developed by the Felsenstein (previously Rogof) institute. It is equine based, 100 PD50/mL-1.
Patient data were transferred to an electronic spreadsheet (Excel 365) and subjected to descriptive and comparative analysis. Data are presented as median (IQR).
The study was approved by Ha’emek Medical Center institutional ethics review board (EMC-20-235).
Results
Overall, between 2015 and 2020, 62 patients presented to the ED after D palestinae bite. Figure 1 describes patient inclusion. Their age was 30 y (17–48), and 75% were male (47). Most patients presented to the ED with local reactions to the snakebite (41%) while 29% presented with advanced local reaction and 29% with systemic symptoms. Antivenom was given to 22% of patients with advanced local reaction and 89% of patients with systemic reaction (Table 1). Overall, 52% of patients were admitted to the hospital with a 2-d length of hospitalization.1,3 Sixteen patients were admitted to ICU (25%).
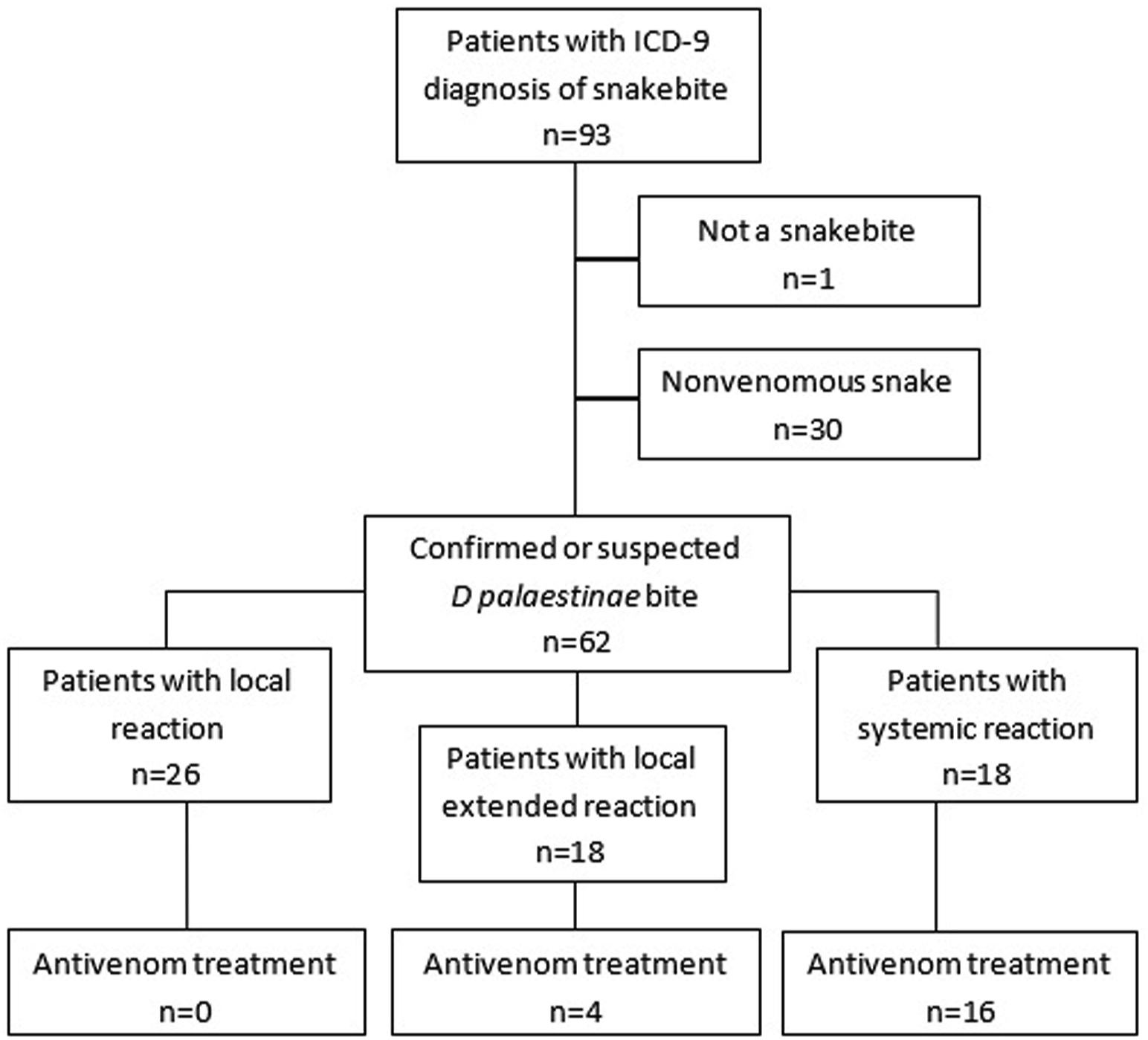
Patient inclusion.
Demographics, general characteristics, and outcome of patients presenting to the ED with D palestinae snakebite
IQR, interquartile range; ED, emergency department; ICU, intensive care unit; LOS, length of stay.
Overall, ED LOS was 4.5 (2.4–7.8) h. Similarly, among discharged patients ED LOS was 4.5 (2.4–7.4) h. The time from bite to antivenom and from ED arrival to antivenom were 2 (1.5–2.5) h and 1 (0.75–1.5) h, respectively. Antivenom was administered at the latest 3.5 h after presentation to the ED for progression of local symptoms. The characteristics of patients treated with antivenom are described in Table 2.
Characteristics of patients treated with antivenom
ED, emergency department; LOC, loss of consciousness; M, male; F, female.
No adverse reactions were reported other than 1 patient who lost consciousness after treatment with the antivenom. She recovered with no need for intervention. One 35-y-old pregnant patient (16 wk of gestation) developed systemic reaction and was treated with antivenom with no reported adverse reactions. Four patients developed swelling progression beyond 2 joints within 24 h. Only one 57-y-old patient was treated with an additional antivenom. The others were observed, with resolution of symptoms.
Two patients with mild systemic reactions were not treated with antivenom; a 21-y-old male with local reaction and mild prolongation of prothrombin time was observed in the ED for 20 h with no progression of symptoms or of worsening coagulopathy. A 47-y-old female with limb pain, nausea, weakness, and palpitations was observed for 7 h in the ED until resolution of systemic symptoms.
One 15-y-old male with local reaction returned to the ED 17 h after discharge with worsening of pain and rash. He was admitted for observation and supportive care with no need for antivenom or surgical intervention.
Discussion
We found that most patients with D palestinae envenomation were treated with antivenom within an hour of presentation to the ED. The latest antivenom administration in the ED was for a patient with mild systemic reaction who was treated with antivenom 4 h after envenomation. Only 4 patients with local extended reaction and no systemic symptoms were treated with antivenom. The progressive local reaction developed within 2 h of their presentation to the ED. One patient received a second dose of antivenom 24 h after admission due to progressive local symptoms. One patient returned to the ED 17 h after bite due to worsening of pain and rash and was treated with antihistamine.
A recent study 4 supports our findings. In their cohort of 41 adult patients bitten by D palestinae, most patients were treated with antivenom within 90 min of presentation to the emergency department, and only 1 patient with systemic symptoms was treated 6 h after presentation. Similar findings were described among envenomated children, 7 possibly because children are more vulnerable to the toxic effect of snakebite in view of the larger dose received relative to body size. 6 In that recent evaluation of antivenom therapy for D palestinae bites in children, among 25 children who were treated, median time from envenomation to antivenom administration was 1 h (up to 2.5 h). One patient was treated with antivenom 24 h post bite for severe tachycardia. 7 Symptom progression in patients with late antivenom administration was not described in these studies.
Data from North America revealed similar findings. An 8-h period of observation for children with mild symptoms after pit viper bite is suggested. 12 This time frame was based on symptoms on presentation to the ED (average of 8 h from snake bite). In Israel, on the other hand, given the short distances from residential areas to hospitals in the geographical distribution of D palestinae, average time from snakebite to ED presentation is much shorter (47 min). 8 Moreover, asymptomatic patients with normal clotting lab results within 6 h of snake bite suggest no envenomation at all. 13
Based on our findings and previous studies,4,7 4 to 6 h of observation in the ED for patients with mild nonprogressive symptoms post D palestinae envenomation may be a safe and sufficient approach. Delayed administration of D palestinae antivenom was already found to be effective.9,14 All cases described had late (>24 h), progressive local manifestations, some accompanied by systemic manifestations and hematological abnormalities, and were treated effectively with antivenom. Thus, discharging patients home with clear return to ED instructions (progressive local manifestation) and after appropriate observation in the ED may decrease unnecessary hospital admissions.
In our study, 1 patient suffered from adverse reactions to the antivenom treatment (Table 2). The antivenom currently used is more purified and less immunogenic than the original antivenom, which was associated with anaphylaxis (4%) and serum sickness (4%).2,8 Our findings differ from recent reports of no adverse reactions to the newer antivenom in envenomated adult and pediatric population,4,7 although our patient did not need any intervention.
Limitations
Our study has several limitations. First, it was a single-center study with the inherent limitations of a low-powered retrospective study. Furthermore, there was a limited follow-up data to confirm the lack of symptoms after discharge. Some variables, such as sequestration of venom, medical comorbidities, and unknown factors, could have led to delayed symptom development. However, it can be assumed that a patient who did not re-present to the ED did not have significant symptoms requiring treatment with antivenom, which is not given outside the hospital. Second, we assumed the case to be D palestinae envenomation by appearance of the injury and based on the habitat of the snake. However, D palestinae is the most common venomous snake in northern and central Israel accounting for most envenomations. 14 In addition, adverse reactions to antivenom may have occurred, but were not documented in the medical records. Delayed reactions or long-term complications may exist.
Conclusions
Our study may support a 4- to 6-h observation period in the ED for patients with local reaction after D palestinae bite. These patients should be discharged only after clear return precautions if medical care is available close to the patient’s home. Further larger prospective studies are needed to confirm our findings.
Footnotes
Acknowledgements
Author contributions Study design (MAM, RJ); data collection (MAM); data analysis and interpretation (MAM, RP, GC, RJ); manuscript draft (MAM, RJ); manuscript revision (GC, RP, RJ); all authors approved the final version of the manuscript.
Financial/Material Support: None.
Disclosures: None.