
Abstract
Introduction
Traumatic shoulder dislocations rank among the most common shoulder injuries in climbers, with rising numbers over the last years. The objective of this study was to analyze the outcome following traumatic first-time shoulder dislocation and subsequent surgical treatment in this population.
Methods
In a retrospective study, climbers who experienced a traumatic shoulder dislocation were treated with an arthroscopic repair of the labrum-ligament complex (LLC). The functional outcome was assessed with a standardized questionnaire and clinical examination, including the Constant Murley and Single Assessment Numeric Evaluation scores. The sport-specific outcome was analyzed using the Union Internationale des Associations d’Alpinisme (UIAA) scale of difficulty and a sport-specific outcome score.
Results
The functional and sport-specific outcome for 27 climbers (20 men; 7 women; 3 with bilateral injuries; age, 34±11 [17–61] y; data presented as mean±SD [range]) was assessed 53±29 (12–103) mo after surgery. The postoperative Constant Murley score was 95±8 (67–100) points. At follow-up, 93% (n=25) of patients had started climbing again. Twenty-one climbers (78%) reached a climbing level within the range of ±0.33 UIAA grades of their initial capability or even exceeded their preinjury grade. Only 7% (n=2) of the patients had a recurrent shoulder dislocation, leading to a secondary surgery, and, therefore, required ongoing postoperative treatment at the time of follow-up.
Conclusions
Arthroscopic repair of the LLC following first-time traumatic shoulder dislocation in climbers shows a good outcome and a low recurrence rate. After surgery, most patients are able to regain a high level of rock-climbing ability.
Introduction
Traumatic shoulder dislocations rank among the most common shoulder injuries in climbers, with rising numbers over the last years. 1 A comparison of the incidence of shoulder dislocations in rock climbers in 2 time frames (2009–2012, n=157; and 2017–2018, n=154) revealed an increase from 10% to 18% (percent of total injuries reported), making shoulder dislocations the third most common pathology of the shoulder in climbers after superior labrum anterior posterior (SLAP) lesions (30%) and impingement pathologies (27%). 2 Due to the trauma, the labrum-ligament complex (LLC), rotator cuff, humeral head (eg, Hill-Sachs lesion), and glenoid (Bankart fracture) are especially prone to damage. As insufficient treatment of a first-time traumatic shoulder dislocation often leads to chronic instability with recurrent shoulder dislocations, thus promoting the development of bone loss and osteoarthritis, targeted therapy based on a thorough evaluation of the injury is very important. 3 -7
Athletes—especially contact, collision, and overhead athletes, such as climbers—are an at-risk population for anterior glenohumeral instability, which is most often due to tear and dislocation of the LLC. 8 For this reason, for most first-time labral lesions and/or bony injuries, immediate surgical therapy is considered the therapy of choice, especially for young, active patients and athletes because of their increased risk of redislocation.4,9-11 In fact, age under 30 y and active lifestyle make shoulder redislocation following conservative therapy far more likely; in contrast, the severity of the injury only seems to have a slight effect on the recurrence rate.4,8,12
Depending on the extent of the pathology and associated injuries, various surgical techniques can be used to repair the LLC, such as open or arthroscopic Bankart repair or the Latarjet procedure.
Recent studies that compared the recurrence rate for shoulder dislocation between patients who had been treated conservatively (recurrence rates, 62–70%) and patients who underwent surgical therapy (open or arthroscopic Bankart repair; recurrence rates, 9–14%) following first-time traumatic shoulder dislocation highlighted the role of surgical therapy.8,12 A study including 65 patients showed a significant long-term benefit in overall shoulder stability and functional outcome for first-time anterior dislocation, comparing patients who had received an arthroscopic washout to those who received an arthroscopic Bankart repair. The rate of recurrent dislocation was significantly higher in the arthroscopic washout group than in the arthroscopic Bankart repair group (47% and 12%, respectively). 9
For contact and collision athletes, studies highlighted a trend toward decreased recurrence rates using open Bankart repair compared to those using arthroscopic procedures. 13 -17 These types of surgeries (open osseous augmentation procedures) are also reliable therapy options and should be used for athletes with glenoid bone loss of >20% to 25%, which can be measured best using computed tomography scans. 8 Recent literature, furthermore, suggests promising results with all-arthroscopic bony procedures such as the Latarjet procedure. 18
Considering the functional and sport-specific outcome following a traumatic shoulder dislocation, all of the above-mentioned studies have been performed especially for collision and contact sports such as rugby or football, while there is still little knowledge about the outcome for noncontact overhead athletes such as rock climbers.
Rock climbers in particular rely on a stable glenohumeral joint in order to achieve their sport-specific goals. During climbing, complex overhead movements with a wide range of motion are performed while significant forces act on the shoulder. Thus, a high level of function is mandatory. Still, to the best of our knowledge, there are no data on the postoperative functional (ie, general recovery of the shoulder required for daily activities) and sport-specific (ie, recovery of rock-climbing ability) outcome after surgical treatment of a traumatic first-time shoulder dislocation in rock climbers.
The purpose of this study was to analyze the general and sport-specific outcome following traumatic first-time shoulder dislocation and subsequent arthroscopic refixation of the LLC in rock climbers.
Methods
The study was approved by the institutional ethics board of the Friedrich Alexander University Erlangen-Nürnberg. All patients gave their informed consent in written form for evaluation and use of anonymized data. Inclusion criteria were active rock climber (climbing at least once a week before the respective trauma), traumatic first-time anterior-inferior dislocation of the shoulder (not necessarily caused by rock climbing), or surgical repair (refixation of the LLC with FASTak suture anchors) performed at our department between 2009 and 2018.
All surgeries were performed by the same experienced shoulder surgeon (VS) in the beach-chair position. The LLC was reconstructed arthroscopically by 1-3 FASTak suture anchors (Arthrex, Naples, FL) depending on the degree of injury. If necessary, associated injuries that were detected in the course of diagnostics (physical examination, magnetic resonance imaging, diagnostic arthroscopy as part of LLC refixation) were simultaneously addressed.
For follow-up, we performed a clinical examination, including inspection and palpation, as well as tests for range of motion, muscle strength, and neurologic outcome. All follow-up examinations were performed by the same physician (LG). For outcome measurement, the Constant Murley score, 19 one of the most commonly used shoulder scores, was used to determine the general function of the shoulder. On a scale of 1 to 100, it combines the results of a questionnaire and physical examination assessing pain, activities of daily living, movement, and strength.
In addition to this examination, all patients completed a standardized questionnaire. The questionnaire included items relating to patient history, injury mechanism, activities of daily life, pain, profession, and expectations with regard to the surgery. We augmented the questionnaire with measurements of subjective postoperative satisfaction and subjective sport-specific outcome. For satisfaction, the Single Assessment Numeric Evaluation (SANE) score was used, wherein patients rated the general function of their shoulder between 0% (no function for everyday activities) and 100% (nonimpaired function). 20 For sport-specific outcome, we queried patients’ subjective evaluation of their climbing capacity on an ordinal scale from I (poor) to V (excellent) (Table 1). 21
Sport-specific outcome score after climbing injuries 25
UIAA, Union Internationale des Associations d’Alpinisme.
To objectively analyze the climbing capacity after return to sport, we also calculated the mean climbing level according to the Union Internationale des Associations d’Alpinisme (UIAA) scale of difficulty,22,23 of the 3 hardest routes climbed in redpoint style within the last year before re-evaluation (ascertained by recall). Redpoint style in this context means to climb a route from the ground to the top in 1 go without falling or even resting on the rope. This level was then compared to the mean level of the 3 hardest redpoint climbs within the last year before the injury. The ability to climb at the same UIAA level 22 ±0.33 in redpoint style, in comparison to the hardest preinjury redpoint climbs, was defined as “preoperative climbing level regained.”
Data are presented as mean±SD (range) throughout the manuscript.
Results
We identified 27 climbers (20 men; 7 women; 3 climbers with bilateral injuries; age, 34±11 [17–61] y) who experienced a traumatic shoulder dislocation and were treated with arthroscopic repair of the LLC. The overall characteristics of our study collective are summarized in Table 2. In addition to the pathology of the LLC, 63% of our patients (n=17; 2 patients with involvement of both shoulders) presented with associated shoulder pathologies at the time of surgical therapy. If appropriate, these were addressed during surgery. For example, in 11 out of 17 patients with additional SLAP lesions, mini-open biceps tendon tenodesis was performed.24,25 Furthermore, in 1 patient, a dislocated fracture of the tuberculum majus was addressed with open reduction and internal fixation using a specialized plate and screws (Figure 1). 26 Table 3 depicts all associated shoulder injuries besides the pathologies of the LLC and information on the additional operative treatment.
Characteristics of the study collective, N=27 (3 patients with bilateral shoulder dislocation)

Postoperative x-ray imaging following open reduction and internal fixation of a dislocated tuberculum majus fracture using a specialized “Bamberg” plate and screws.
Associated shoulder injuries besides pathologies of the labrum-ligament complex and their additional treatment
PASTA, partial articular supraspinatus tendon avulsion; SLAP, superior labrum anterior posterior.
Subacromial impingement syndrome was diagnosed on the basis of a thorough clinical examination and preoperative magnetic resonance imaging.
After surgery, each patient received a personalized follow-up treatment, typically starting with passive mobilization (associated injuries permitting, as early as third postoperative day) and later permitting general sport-related activities (12 wk after surgery), gradual resumption of rock climbing (16 wk after surgery), and, finally, full sport-specific exertion (6 mo after surgery). The detailed rehabilitation protocol following isolated injuries of the LLC that we have used is presented in Table 4. It is based on the recommendations of the current literature 27 and augmented by the authors’ experience regarding the specific characteristics of and requirements for rock climbing.
Postoperative rehabilitation protocol.
Bolded text indicates the most important steps of the rehabilitation protocol.
The follow-up examination was then performed at least 12 (53±29 [12–103]) mo after surgery. In case of revision surgery, follow-up was performed at least 12 mo after the second surgery.
Regarding the general outcome, the mean Constant Murley score was 95±8 (67–100) points (n=30 shoulders and n=27 patients). Ninety-two percent (n=25) of the patients were satisfied with the postoperative outcome (100% SANE score for everyday activities) and stated that they would choose to undergo the procedure again. Two patients reported persisting complaints in everyday life, stating a SANE score of 80% and 65%, respectively. In all patients with bilateral injuries, we found no difference considering the outcome scores between the 2 shoulders.
Two patients (7%) had a renewed shoulder dislocation. While 1 experienced a new significant trauma, the other patient’s shoulder dislocation happened as part of an overhead workout during outpatient rehabilitation 2 months following surgery. These 2 patients had to undergo revision surgery after magnetic resonance reimaging showed renewed damage to the LLC and, in 1 case, also to the glenoid, with bone loss. The patient who had a bony injury of the glenoid was treated with an arthroscopic assisted mini-open Latarjet procedure, 28 and the other patient was again treated arthroscopically with LLC repair using FASTak suture anchors.
Furthermore, 1 patient developed a secondary adhesive capsulitis, leading to temporarily restricted mobility and pain, which was successfully treated conservatively with physiotherapy.
Regarding the sport-specific outcome, at the time of follow-up, 93% (n=25) of our patients had resumed climbing on a regular basis, at least once a week. The 2 patients with a recurrent dislocation were both already climbing again. Furthermore, 2 patients had not started climbing again. One of those patients stated that family responsibilities were the cause, while he was 100% (SANE score) satisfied with the postoperative outcome and displayed a Constant Murley score of 100. Thus, he was excluded from the following evaluation of the sport-specific outcome. The second patient reported that he was not able to climb because of persistent complaints in his shoulder. While this was reflected in his Constant Murley score of 71, he was still subjectively satisfied with the outcome and reported a SANE score of 95%.
For those patients who had resumed climbing, the mean postsurgery UIAA climbing level had not changed in comparison to the preinjury climbing level (9±3 UIAA grades), while the range had changed from 6.33 to 11 to 4.33 to 11. Specifically, at the time of re-evaluation, 68% (n=17) of the patients had regained their initial climbing level, as objectively measured using the UIAA scale, 16% (n=4) had not, and 16% (n=4) exceeded their initial level (Figure 2).
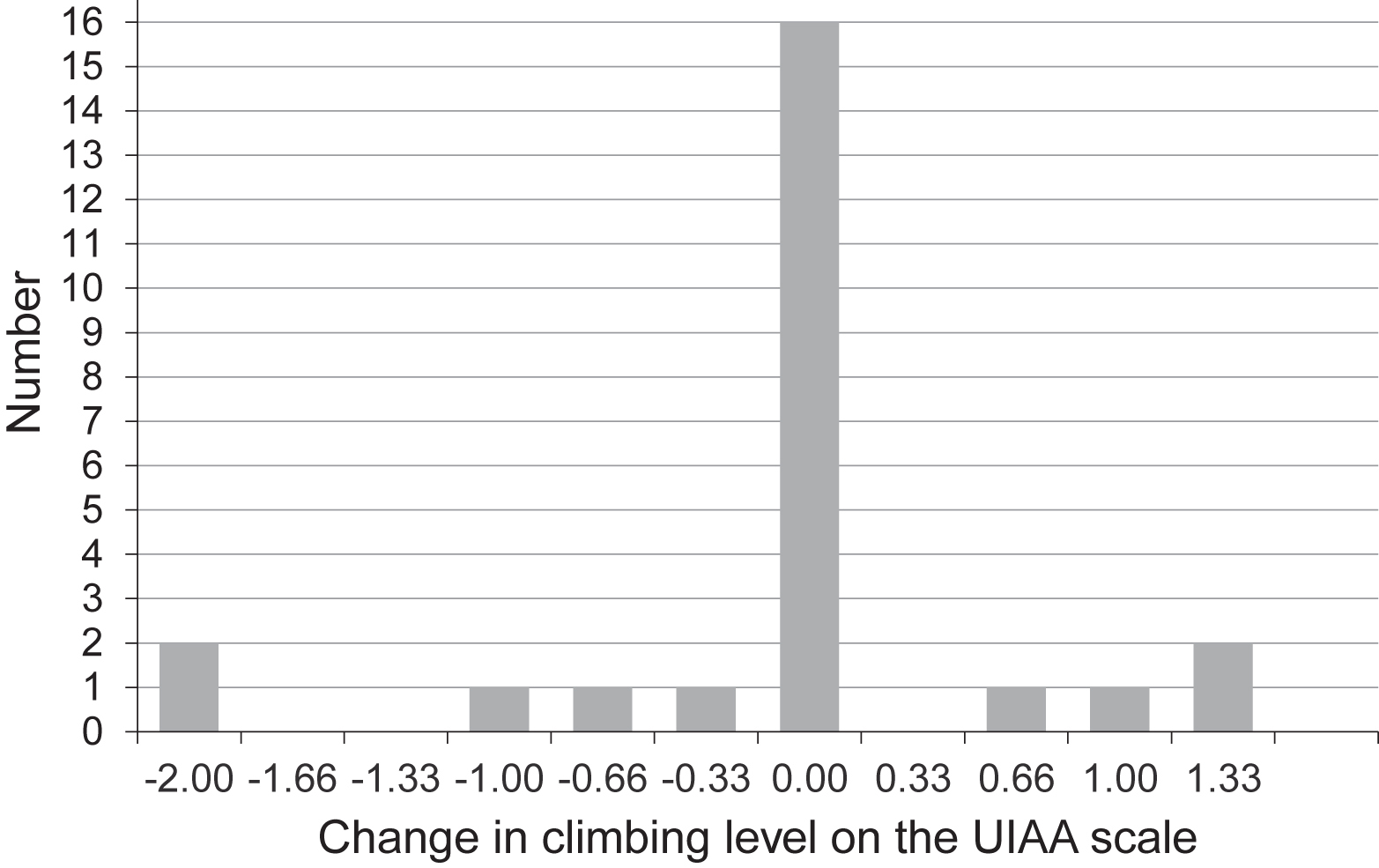
The change in climbing level after surgery is depicted for all participating climbers who had returned to sports (n=25) using the Union Internationale des Associations d’Alpinisme scale. UIAA, Union Internationale des Associations d’Alpinisme.
With regard to the overall sample, 78% (21 of 27 climbers) of patients had returned to the sport at the preinjury level of climbing or even exceeded their preinjury level.
These results were reflected in our patients’ subjective evaluation of their sport-specific outcome (n=26). Here, excellent (V) results were reported in 73% (n=19) of cases, good (IV) results in 12% (n=3), satisfactory (III) results in 4% (n=1), fair (II) results in 8% (n=2), and poor (I) results in 4% (n=1).
Discussion
The overall outcome following surgical repair of pathologies associated with first-time traumatic shoulder dislocations in climbers shows promising results for activities of daily life and sport.
Our results are consistent with recent literature emphasizing the role of immediate surgical therapy as the treatment of choice for most cases of first-time anterior shoulder dislocations, especially in young patients and athletes.9,10 While recurrence rates between 62% and 70% have been described in conservatively treated patients, recent meta studies reported a recurrence rate between 12% and 20% after arthroscopic soft-tissue LLC repair, with recurrence being defined as any report of dislocation or subluxation.9,29,30 With a recurrence rate of only 7% (n=2), our findings are more favorable than the rates described in the current literature. However, the results are only comparable to a limited extent since many of the athletes included in the studies mentioned above were participating in contact and collision sports, such as rugby or American football, which might present a greater risk for a recurrent dislocation than rock climbing. Compared to collision and contact sports, a direct trauma to the arm and the shoulder girdle occurs much less frequently in rock climbing (specifically, roped climbing, ie, climbing with a rope using fixed bolts for security), thus possibly reducing the risk of repeated shoulder dislocation. However, in the climbing subdiscipline of bouldering (climbing without a rope at relatively short jump-off heights with crash pads for protection), falls onto the shoulder and the arm are inevitably more frequent than in roped climbing. 31 As the participants in the presented study are mainly sport climbers, further research is necessary to find out if there is an increased risk for recurrent shoulder dislocation in bouldering athletes.
With a return-to-sport rate of 78% at the preinjury level of climbing or above, our results are comparable to those of existing studies including both contact and noncontact athletes, such as volleyball players, water polo, rugby, soccer and tennis players, that found a return-to-sport rate of 81% to 83% at the preinjury level.17,32 Still, due to the differences between the disciplines, a direct comparison is not feasible.
Our findings are also in line with recent research on the surgical treatment of other climbing injuries, specifically SLAP lesions and rotator cuff tears, which also found favorable functional and sport-specific outcomes following surgery (for a detailed comparison, see Table 5).24,33
Comparison of functional and sport-specific outcomes after surgical therapy of shoulder dislocation, superior labrum anterior posterior lesions, and rotator cuff tears in rock climbers
In total, 4 patients in our study had not returned to their previous climbing level at the time of follow-up, and 1 patient was unable to return to the sport after surgery because of persistent complaints due to secondary adhesive capsulitis in addition to his pre-existing high-grade osteoarthritis. This is a rare but well-known complication after surgical repair following shoulder dislocation. 34 Since the follow-up examination of this patient was performed 15 months after surgery, further improvement in this individual is possible but was not confirmed. It is likely that the presence of associated injuries or pre-existing degenerative pathologies (Table 3) might have led to prolonged or incomplete recovery after traumatic shoulder dislocation.
Limitations
Our study might have incorrectly estimated the presurgery climbing level due to recollection bias. Climbers might have misremembered when reporting their maximum climbing level. The postsurgery climbing level might have been influenced by temporary suspension of the patients’ training routine, as required by the rehabilitation protocol, wherein full exertion was allowed only 6 mo after surgery. Thus, the climbing level might have been different if we had measured it later than 12 mo after surgery.
We only report descriptive data and did not compare the results following surgery with those of a conservatively treated control group as extant literature highlights the superior efficacy of surgical therapy over conservative treatment.
The generalizability of our findings is limited because of the small sample size. Furthermore, as the performing surgeons’ department is a recognized center for the treatment of climbing injuries, a selection bias might have occurred as only active, high-level climbers might have sought out this surgeon’s opinion and treatment. Associated with this is the limitation that all operations were performed by only 1 experienced surgeon, which might have further biased our results.
Finally, our sample included not only isolated traumatic pathologies of the LLC of the shoulder, which complicates the assessment of our findings.
Conclusion
In this study, we presented descriptive data based on a relatively small sample. Our findings are promising and show that a favorable outcome following first-time traumatic shoulder dislocation and arthroscopic repair of the LLC in climbers is likely. This includes both general function and sport-specific performance. Most athletes in our sample were able to return to or near their preinjury level of climbing after surgery, and shoulder dislocation recurrence rates were low.
Our results thus concur with the extant literature centered on other sport disciplines. In summary, we view arthroscopic surgery as an advisable treatment for climbers who wish to return to this sport after a first-time traumatic shoulder dislocation and associated acute traumatic pathologies, specifically of the LLC. Of course, patients still need to be informed about the general risks of the procedure and should be made aware of potential adverse effects on their climbing performance.
Footnotes
Acknowledgements
Author Contributions: study concept and design (MS, LG, CL, VS); acquisition of data (MS, LG, CL, VS); drafting of the manuscript (MS); critical revision of the manuscript (LG, CL, VS); approval of final manuscript (MS, LG, CL, VS).
Financial/Material Support: None.
Disclosures: None.