
Abstract
Hand injuries from surfing tend to be severe and require medical attention. Follow-up of a surfing injury is difficult because many patients are visiting and go home after treatment. We report a case of a surfing hand injury sustained abroad, which was treated upon the patient's return, allowing for follow-up. The mechanism of injury was traction and torsion from the surfboard leash while surfing. The patient was initially treated for nailbed injury but presented later back home after persistent pain, for which an unstable distal phalanx fracture in their right ring finger was found by x-ray. This was surgically reduced with K-wire insertion and nailbed repair. Postoperatively, the injured finger was kept in a splint, and the patient had physiotherapy. Pain was significantly reduced, and the patient regained sufficient function. Considering a fracture as a differential for finger injury caused by the surfboard leash may prevent management delays. Injury may be prevented through education and redesign of the surfboard leash.
Introduction
Surfing is a relatively low-risk sport compared to other sports, such as soccer and basketball.1,2 However, after its debut at the Tokyo 2020 Olympics, we may see more surfing injuries along with its increasing popularity. Surfing injuries commonly occur in the head, neck, and lower limbs.1–3 Hand injuries, which are less frequent, most commonly consist of skin injuries, but surfers who decide to seek emergency care for their hand tend to present with fractures instead.1,4,5 However, we found very little evidence pertaining to follow-up and long-term outcomes after fracture management. Follow-up is difficult because many patients are holidaymakers and go home after the initial treatment. 5 This case study presented a unique opportunity to assess long-term outcomes after an acute surfing hand injury. This case was reported based on CARE guidelines.
Case report
We present a case involving an open distal phalangeal fracture to the right ring finger of a 20-y-old, normally fit and well, right-hand-dominant female surfer. The individual was gripping the surfboard's leash when the board was forcefully and suddenly moved by a breaking wave. This avulsion-type injury was sustained abroad and, on initial presentation, was seen without radiological investigation and managed as a simple soft-tissue nailbed injury. On returning to the United Kingdom 2–3 wk following the injury, the individual re-presented to her local hospital, having experienced persistent fingertip pain in her affected digit. The right ring finger demonstrated deformity and avulsion of the proximal nail plate from the nail fold. There was no tendinous injury, neurovascular deficit, rotation, or scissoring. Anterior-posterior and lateral radiographs demonstrated an unstable, transverse fracture of the distal phalangeal base (Figure 1). Surgical reduction was performed by inserting a single Kirschner wire percutaneously through the vertical axis of the phalanx (Figure 1), and the nailbed was repaired. Following 4 wk of hand therapy involving a proximal interphalangeal joint movement regimen, the individual reported residual stiffness at the distal interphalangeal joint and significantly reduced pain. She regained sufficient range of motion, and function was not impaired.
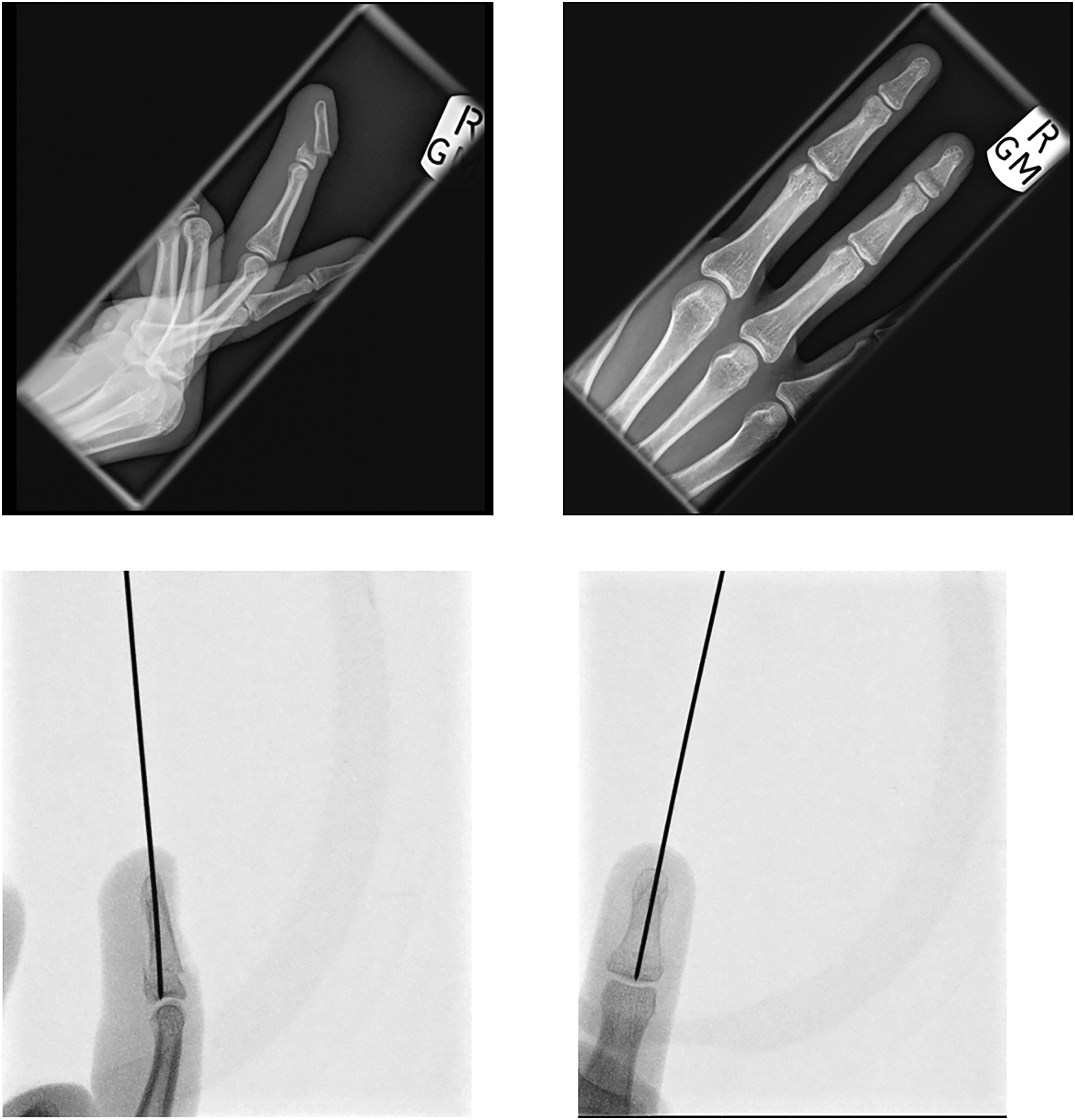
Lateral and antero-posterior x-rays of injured finger. Top row shows before surgery, and bottom row shows after K-wire insertion.
Under Health Research Authority (UK) guidelines, our case study does not require review by a research ethics committee. The patient has provided written informed consent for the publication of this case report and radiographs before and after the surgery. University Hospitals Plymouth NHS Trust does not require ethical approval for reporting individual cases or case series.
Discussion
The majority of studies showed that acute surfing injuries commonly occur in the head and neck and in the lower limbs.1–3 However, there is some debate between studies as to whether the shoulder or the hand is the most common acute upper-limb injury.3,4,6 The method of data collection could explain this discrepancy. Taylor (2004) showed that emergency department medical records will more likely pick up acute hand injuries as they tend to be severe (such as fractures) compared with surveys completed by active surfers. 4 Meanwhile, there is a general consensus that minor injuries such as lacerations and contusions are the most common type of acute surfing injury.1,2 Ruijs's case series reported that 26 out of 37 hand injuries (70%) were fractures, of which 21 were open (81%) and 24 (92%) were due to the surfboard leash. 5 Other hand injuries besides bone injury include sprains, open wounds, digital nerve lesions, and flexor tendon injury.4,5 The above implies that hand injuries are more likely to be severe and require medical attention compared to shoulder injuries, and therefore, clinicians are more likely to encounter them. In addition, different experience levels of surfers may lead to different results between studies, as more experienced surfers will be more likely to perform aerial maneuvers as they score more points in competitions and, therefore, more likely to sustain hand fractures. 1 However, a limitation of this study is that we do not know the patient's surfing experience and skill. Further research is needed to examine this association between experience and upper-limb injury.
Other demographic factors to consider for acute injury are age and gender. Within the literature, increasing age was associated with significant injury, with risk almost doubling for surfers more than 40 years old. 2 Our patient's future risk of injury may, therefore, rise if they continue to surf. In addition, they will have further experience with age and may prefer performing higher-risk surfing maneuvers when they are older. In contrast, gender has been reported to not affect the risk of significant injury. 7 Many studies report that most (if not all) of their surfers are male, and others do not even report surfer gender. 1 It can be argued instead that there were not enough female surfers to make a fair comparison, but this issue may become less relevant with the sport's increasing popularity. On the other hand, gender may influence patient outcomes, with sources reporting that women are more likely to seek medical help than men.8,9 This may potentially affect the timing of presentation and compliance with follow-up. However, this may not apply to athletes, and therefore, gender's impact on patient outcomes is a recommended area for future research for both surfing and watersports in general.
The mechanism of injury to the hand often involves the surfboard leash. 5 Originally designed to prevent an uncontrolled surfboard from hitting others nearby, it conversely also increases the risk of hitting the surfer themselves.3,4 Hand injury occurs when the leash wraps itself around the surfer's digit while surfing. The board may end up being jettisoned and rapidly moves off in direction, usually after bailing from the board. This then causes rapid traction and torsion forces on the digit around which the leash is wrapped, leading to fracture or soft-tissue degloving. This is similar to the mechanism of injury from dog leads when a dog bolts away from the walker. A redesign of the leash may help prevent injury, although the risks of injury to self need to be balanced with the risk of injury to others. 4 Injury may also be prevented through education at surf schools, teaching surfers to refrain from holding onto their boards or pulling the boards back with the leash. 5
In contrast to acute injury, the leash is not a common cause of chronic hand injury. Chronic injuries were predominantly caused by repetitive strain or overuse when pushing down to stand up on the surfboard, followed by duck diving.4,10 Age, rather than surfer experience or hours spent surfing, was a significant risk factor. 10 The most common sites of major chronic injury are at the joints, which reflects the repetitive nature of the injury mechanism. While the leash risks acute injury, it has minimal impact on hand injuries in the long term.
Long-term outcomes for surfing injury management were previously difficult to assess, as many patients did not live locally and returned home after initial treatment. 5 In contrast, this patient received follow-up as the initial fracture management occurred after they had returned home. The patient presented here fully recovered and regained satisfactory function. Regardless of delay in management, the phalangeal fracture remained treatable with minimal immediate complications. Continuity of care with the hand therapists after the operation may also have contributed to the patient's recovery. Nevertheless, it is difficult to determine after a 4 wk follow-up whether delayed intervention will lead to any subsequent chronic injury. Chronic injury following a previous acute hand injury is uncommon but not impossible. 4 In this sense, the lack of continued follow-up for long-term outcomes for this patient was a limitation to this study, as it is difficult to know at present if this patient's fracture limited any future function (such as their surfing activity) or caused any chronic injury. There is opportunity to assess long-term outcomes with further follow-up.
For patients presenting with a surfboard leash–related injury, excluding a phalangeal fracture with imaging may prevent delays to management, especially if there is persisting pain. Delayed management has no immediate negative impact on function and pain, but outcomes in the long term are unknown. Prevention by either teaching surfers to safely avoid surfboard leash injury or a careful redesign of the surfboard leash may help reduce risk of injury to the surfer while continuing to stop the surfboard from hitting others nearby.
Footnotes
Author Contribution(s)
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by all authors. The first draft of the manuscript was written by Ryo Yoshimura, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. The authors consider that the first two authors should be regarded as joint first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Justin Wormald, NIHR Doctoral Research Fellow, NIHR301793, is funded by the National Institute for Health Research (NIHR) for this research project. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, NHS, or the UK Department of Health and Social Care.
Informed Consent Declaration
Written informed consent was obtained from the patient regarding submission of case report and radiographs for publication.