
Abstract
Objective
To evaluate the injury risk associated with indoor rock climbing competition.
Methods
All injuries reported to medical personnel at the 2005 World Championships in Rock Climbing were recorded and analyzed.
Results
Four hundred forty-three climbers (273 men, 170 women) from 55 countries participated in 3 separate disciplines totaling 520 climbing days. Only 4 of 18 acute medical problems that were treated were significant injuries, resulting in an injury rate of 3.1 per 1000 hours.
Conclusions
Indoor rock climbing competition has a low injury risk and a very good safety profile.
Introduction
Since the first World Championships in Rock Climbing in 1991, indoor rock climbing has grown tremendously in popularity. In 1991, only a few countries participated, but at the 2005 World Championships in Munich there were almost 500 climbers from 55 countries. A future goal for the Union Internationale des Associations d’Alpinisme (UIAA), the International Mountaineering and Climbing Federation, and the International Council for Competition Climbing is to see rock climbing included in the Olympics.
Some people still see rock climbing as a high-risk or “adrenalin junky” sport. 1 –5 Outdoor rock climbing is very diverse, and it is difficult to run exact scientific studies on the injury risk of outdoor climbing because the risks and the precautions taken depend on the type of rock climbing chosen by each individual. 6 Bowie et al 7 found an injury risk of 0.2% to 0.4% per climbing day in the Yosemite National Park, equaling 37.5 injuries per 1000 hours of exposure (assuming 1 day of climbing in Yosemite is 8 hours). Nevertheless, a much lower risk potential was observed in 2 studies of indoor climbing. Limb 8 recorded 55 accidents in 1.021 million visits to British indoor climbing walls. Assuming an average of 2 hours per visit, this results in 0.027 injuries per 1000 hours of exposure. Schöffl and Winkelmann 9 surveyed the risk of significant injuries on indoor climbing walls during a 6-month period. A total of 25 163 visitors were registered at the 10 walls studied. Overall, only 4 significant injuries were found, and the injury risk per visit was 0.016%. Estimating 2 hours of performance per visit, this results in 0.079 injuries per 1000 hours of performance. These studies demonstrated a minor injury risk for indoor climbing in comparison with various other sports.9,10
The aim of our study was to evaluate the risk of injury at a high-end indoor rock climbing competition in order to analyze injury patterns and suggest means for injury prevention.
Methods
The first author (V.R.S.) served as the official UIAA competition physician at the 2005 World Championships in Rock Climbing in Munich. All reported injuries were recorded; the injury patterns were analyzed; and, if possible, preventive safety measures were suggested and discussed with the official delegates of the UIAA and International Council of Competition Climbing. Preexisting injuries and overuse problems, which were also treated, were not included.
Time of climbing performance (climbing time) was calculated by including warm-up, cool-down, and performance time. A lead competition climber spends about 11/2 hours in isolation warming up. This typically includes bouldering, gymnastics, and stretching. The performance time is 8 minutes in the first round. In the second round there is another, shorter warm-up. In the workout (second day Lead Climbing), the climber has 30 minutes after the warm-up for practicing the route. There is usually another warm-up session about 12 minutes long before the performance in the evening. The proceedings for the bouldering are comparable. A warm-up is followed by the competition in which the climber has 6 minutes per boulder problem with a 6-minute break in between and a total of 6 boulders to complete. For the Speed Climbing, the performance time is short (9–18 seconds) after warm-up, but up to 16 routes need to be climbed. After the competition, the climbers cool down for approximately 15 minutes with climbing, running, or stretching. An average competition day consists of 2½ hours of performance.
Results
Four hundred forty-three climbers (273 men, 170 women) from 55 countries took part in 3 disciplines: Lead Climbing, Speed Climbing, and Bouldering. A total of 116 men and 68 women participated in Lead Climbing, 45 men and 23 women participated in Speed Climbing, and 112 men and 79 women participated in Bouldering. All climbers participated for at least 1 day. In Lead Climbing, 26 men and 26 women reached the semifinals and finals, and 12 men and 13 women participated in the finals in the Bouldering competition, thus climbing a second day. The overall climbing time was 520 competition days, equaling 1300 hours.
Injuries (See Table)
A total of 18 acute medical problems were treated, most of which were mild bruises (n = 13) attributed to contact with the wall or minor rope burns. Only 4 significant injuries occurred, 1 of which put the athlete out of competition and resulted in a longer recovery time. One male climber complained of nausea, probably stress-related, which improved after medication.
Injuries at the 2005 World Championships in Rock Climbing
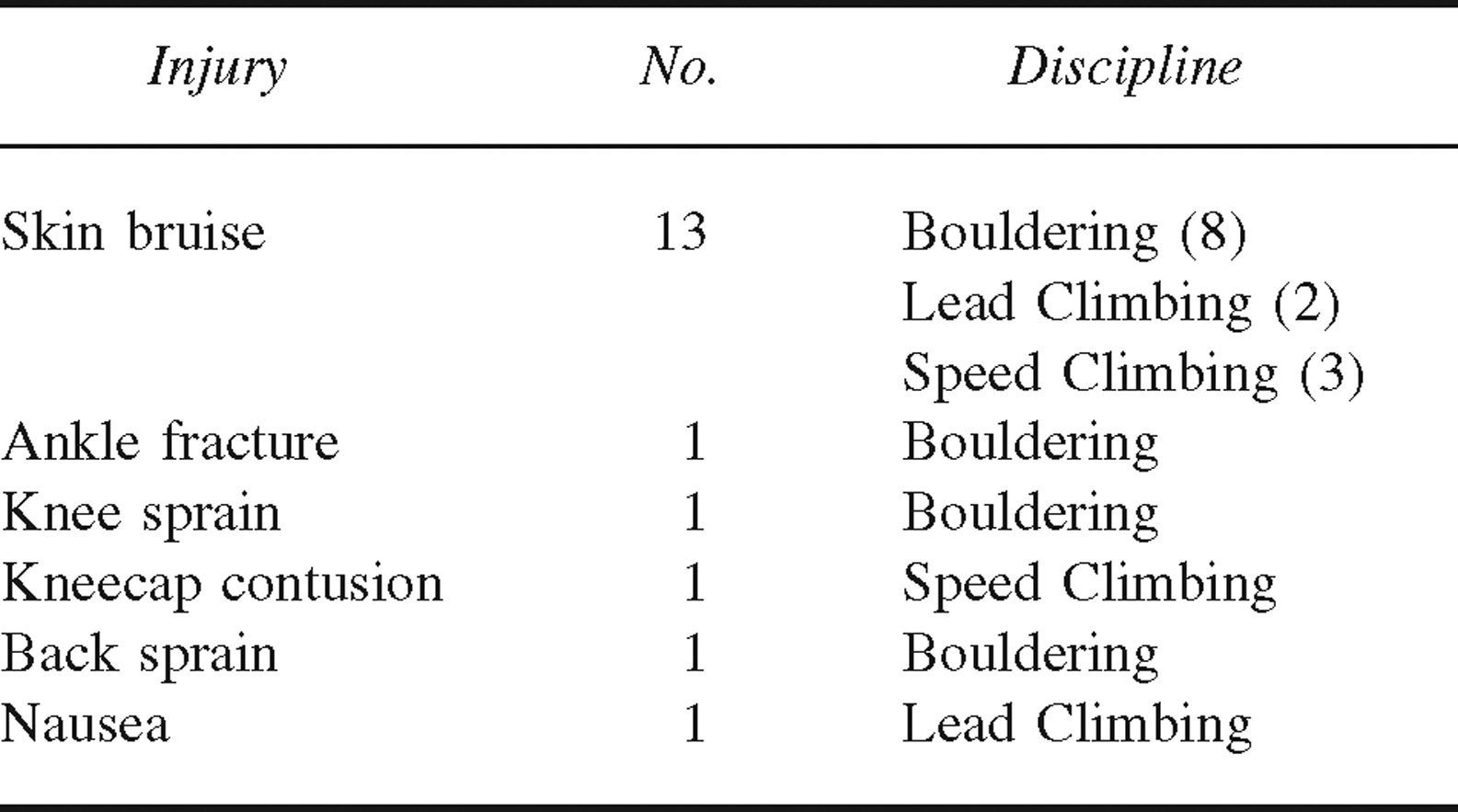
The 4 significant injuries (all to women) were an ankle fracture, a knee strain, a kneecap contusion, and a back sprain. The ankle fracture occurred during a fall with the climber's body initially erect but then with an additional rotational moment that caused a twisting of the ankle, resulting in a break. The climber had to end the competition and later had a surgical repair. The knee strain (strain of the musculus popliteus and injury to the posterior insertion of the lateral meniscus) happened when heel hooking during a particular boulder problem. After treatment, the climber continued the competition. Another female climber fell backwards onto the boulder mattress, causing a minor back sprain. After osteopathic mobilization of the lower spine, she was able to proceed with the competition without further complaint. The kneecap contusion occurred in the Speed Climbing. The climber wore shorts and hit her knee multiple times against the wall or the holds, causing skin bruises and a kneecap contusion. After medical treatment she was able to continue the competition, achieving second place.
Discussion
In the past, ankle sprains and fractures were quite common in bouldering competitions,9,11–13 mostly caused by the climber misplacing a foot between the protection mattresses and twisting it. This injury pattern is now rarely seen because of a new rule by the ICC, based on the medical statement of the Medical Commission of the UIAA 11 mandating closed intersections between the mattresses and the adjacent area of the boulder (Figure 1). Some ankle fractures result from twisting an ankle while landing on a soft surface (mattress) after a fall. In this type of mechanism, the climber tends to fall backwards or sideways onto the mattress. Increased safety in lead climbing is achieved with 1 belayer plus 1 backup belayer plus a third person spotting the climber on the lower part of the route and with the use of a mattress (see Figure 2). The risk of a ground-fall injury is thus minimized. 12

Velcro straps are used to cover intersections between mattresses.
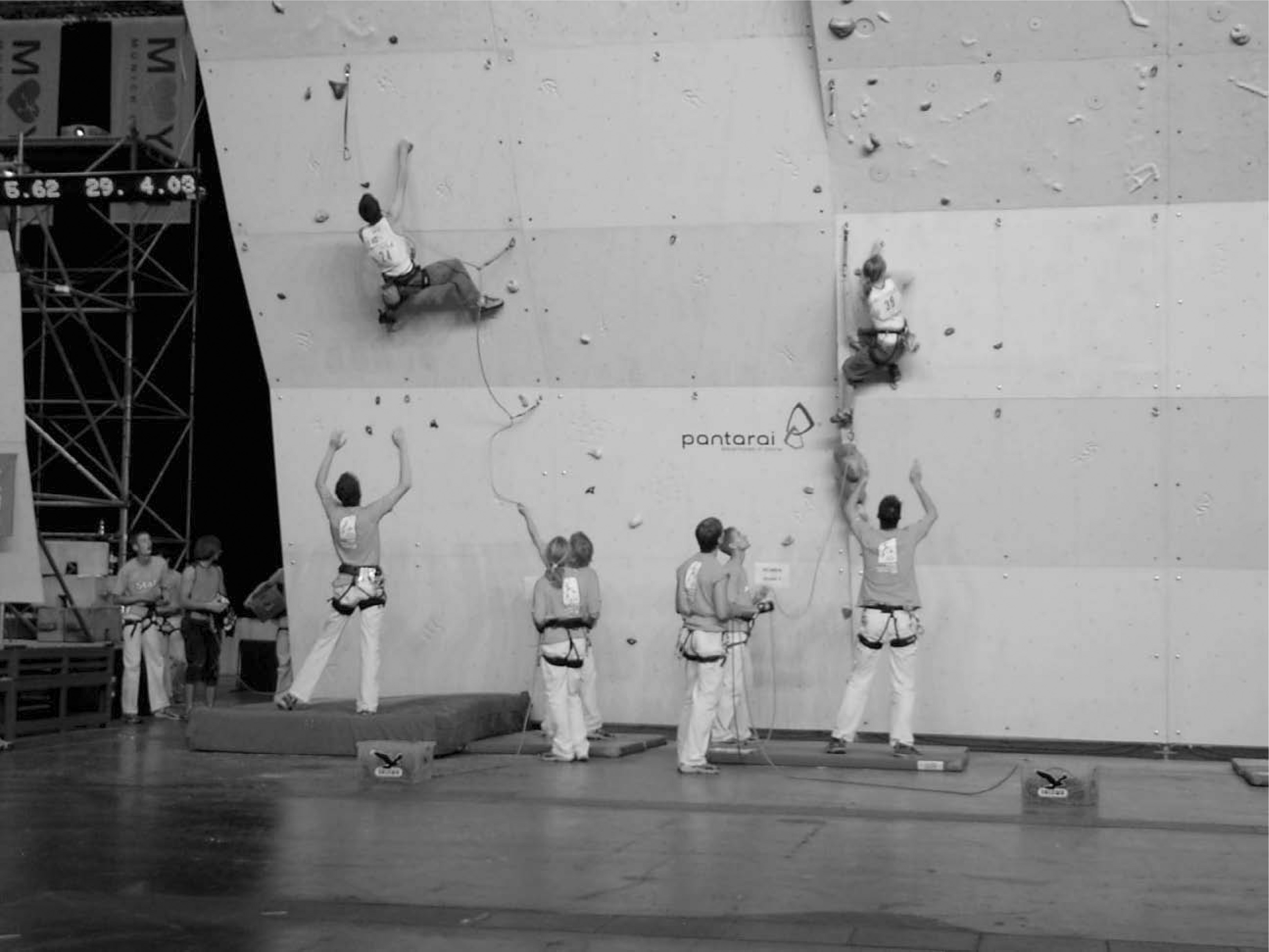
Climbers were “spotted” in the lower section of the routes to improve safety.
All the skin bruises were minor and were probably presented for treatment only because a physician was present. The other 3 injuries, except for the ankle fracture, were relatively minor. Nevertheless, they were included in calculation of injury risk and resulted in a risk of 0.77% per climbing day (4/520) or 3.1 injuries per 1000 hours. This is a higher risk than demonstrated in previous studies8,9 on indoor climbing. This may be due to greater risk-taking behavior by climbers competing in a world championship. It is interesting that all the 4 significant injuries occurred in female climbers. Because of our small sample size, we consider this to be a coincidence. Although highly active male climbers have demonstrated no increased risk of fractures, 14 it is still unclear if there is evidence for increased osteoporosis in relation to a low body mass index in female climbers. This is currently the topic of an ongoing study we are performing with the Institute of Medical Physics, Department of Osteoporosis Research, University Erlangen-Nuremberg, Germany.
Seventy-five percent of the significant injuries occurred during the Bouldering competition, which can be explained by analyzing the competition patterns. Although the lead climber mainly takes a free fall once per performance without wall contact, the boulderers have as many tries per boulder problem as possible (in a 6-minute time frame). Therefore, they have many more falls—always with ground contact. Spectators as well as the media demand spectacular boulder problems with lots of dynamic moves and jumps, which lead to numerous uncontrollable falls. Schöffl and Winkelmann 13 and Schöffl and Hochholzer 15 distinguished between rock-impact traumas during which the climbers get pulled against the wall through rope pull and ground-fall traumas with respect to the lower extremity. Ground-fall traumas are typically distortions, sprains, and fractures of the ankle, that is, injuries that are therefore to be expected in boulder competitions. Considering these injury patterns, a balance between thick and soft or thin and hard mattresses is important. Boulders where a climber falling straight downward onto his or her feet is expected should have thinner and harder mattresses for ankle control, whereas soft mattresses are needed in boulder problems where uncontrolled and full-body landings are expected.11,13,15 Standards were defined through the Medical Commission of the UIAA 11 to regulate the thickness and the compression factor of mattresses as well as the extent of the area to be covered around a boulder problem. In Munich, “spotters” were present at the more dangerous boulder problems. Nevertheless, teams need to focus on fall training and ankle stabilization training needs, which are already part of the normal training routine in some countries. Rock climbing has already been used for functional ankle control in rehabilitation of ankle instability. 16
It is interesting to compare these results with outdoor and indoor climbing. Limb 8 found an injury risk of 0.027 per 1000 hours of exposure, and Schöffl and Winkelmann 9 found an injury risk of 0.079 per 1000 hours of performance. Considering 1 climbing day (competition, warm-up, and cool-down) to consist of 2½ hours of sport activity, there were 1300 hours of exposure at the World Championships. With 4 significant injuries, we obtained an injury rate of 3.1 per 1000 hours, which is higher than in general indoor climbing8,9 but lower than in outdoor climbing. 7 Assuming 3.1 injuries per 1000 hours and 4 hours per day of climbing, this would translate to 12.4 injuries per 1000 days of exposure in competition climbing. This is similar to the risk of many outdoor activities (eg, hiking, mountain biking, kayaking) but smaller than some competitive outdoor sports (eg, adventure racing has much higher injury rates).17,18 In comparison with the German “standard sport activity,” soccer, Ekstrand et al 19 found a higher injury risk in male senior national soccer players in competition (30.3 per 1000 hours) and training (6.5 per 1000 hours).
Conclusions
Overall, indoor rock climbing has a low injury risk and very good safety profile in high-level competition.