
Abstract
Introduction
Nonfreezing cold injury (NFCI) occurs when tissues are subjected to prolonged cooling that causes tissue damage, but not freezing. Long-term effects include cold intolerance, with allodynia, pain, or numbness of the affected limb. Those who participate in outdoor paddlesports are at particular risk.
Methods
This is an epidemiological study that aimed to determine the risk factors for paddlesport athletes developing NFCI and chronic cold intolerance in their hands. Secondary outcomes were to correlate cumulative cold exposure with the development of cold intolerance and to identify risk factors for developing NFCI or cold intolerance. Six hundred nine athletes responded to a survey distributed by their national governing body obtaining demographic and activity details, symptoms of NFCI, and a cold intolerance severity score (CISS).
Results
Twenty-three percent reported symptoms consistent with acute NFCI. The median CISS was 31 y (interquartile range 25–43), and 15% had a pathological CISS defined as >50. Females and individuals with Raynaud’s phenomenon or migraines had a significantly higher CISS (P<0.05). Regression analysis found that females, smokers, and those with Raynaud’s phenomenon or a previous nerve injury had a significantly higher risk of developing pathological cold intolerance (CISS >50). There was no correlation between cumulative cold exposure and CISS.
Conclusions
A large proportion of paddlesport athletes undertaking activity in cold conditions have a pathological CISS or episodes consistent with NFCI. Cumulative cold exposure was not associated with a pathologically high CISS. The risk factors were female sex, smokers, and those suffering from either Raynaud’s phenomenon or nerve injury.
Introduction
Nonfreezing cold injury (NFCI) occurs when tissues are subjected to prolonged cooling that causes damage, but does not cause freezing.1,2 This typically occurs during exposure to cold and wet environments, affecting the hands and feet. 2 First recognized in World War II, numbness of peripheral limbs upon prolonged cold exposure followed by painful hyperemia upon rewarming was described, lasting from 30 min up to several days. 2 A final chronic phase has subsequently been recognized, which can last from several years to a lifetime.3,4 Long-term effects commonly include cold intolerance, with allodynia, pain, or numbness of the affected limb upon exposure to cold.2,5,6 The exact pathogenesis of NFCI is poorly understood but is hypothesized to be a combination of vascular and neural dysfunction. 6 -8 Prolonged exposure to cold with subsequent vasoconstriction results in tissue ischemia. 9 This ischemia is thought to result in damage to the vascular endothelium, compromising its ability to initiate vasodilation. 10 However, neurological examination of those with chronic NFCI has suggested a neurological component to the syndrome. 7
NFCI continues to be a problem for military personnel in cold environments.11,12 Civilians undertaking outdoor sports during cold conditions in temperate climates, such as the UK, exposes them to similar conditions and hence places them at risk. Those who participate in outdoor paddlesports, such as outdoor canoeing and kayaking, are a prime example. The hands are exposed to a cold, wet environment and are frequently immersed in cold water. This can be up to several hours of duration at a time. Anecdotally, many have experienced symptoms consistent with an NFCI and have over time developed cold intolerance as a result of their activities.
The relationship between NFCI, repeated cold exposure, and the subsequent development of chronic cold intolerance is poorly understood and complex and has not yet been fully defined. Military studies have found that individuals with certain traits, such as Afro-Caribbean ethnicity, low body mass index, and smoking, are more susceptible to NFCI and developing cold intolerance.11,12 Pathological cold intolerance has also been associated with other neurovascular conditions such as previous limb injury, Dupuytren’s disease, diabetes mellitus, peripheral vascular disease, and migraines. 13 However, it is thought that increased and repeated cold exposure and NFCI increase the risks of developing chronic symptoms such as neuropathic pain and pathological cold intolerance.4,7
This study aimed to: Determine if paddlesport athletes who are regularly exposed to cold conditions suffer from NFCI and develop chronic pathological cold intolerance in their hands. Correlate repeated cold exposure with development of chronic cold intolerance. Identify risk factors for developing chronic cold intolerance and NFCI.
Methods
This was an epidemiological study of paddlesport athletes in the United Kingdom conducted during March 2021. An online survey was created using SurveyMonkey software (Momentive Inc, San Mateo, CA). This was distributed by the national governing body in the United Kingdom (British Canoeing) via their Twitter page in a series of 2 tweets spaced 2 wk apart. All respondents were included in the final analysis.
Participants completed the survey on a voluntary basis, which included permission to use any personal data provided for the purposes of research and education in accordance with General Data Protection Regulation. The study was registered with the audit and research department at the Pulvertaft Hand Centre and deemed not to require ethical approval.
Demographic information such as age, sex, ethnicity, smoking status, and medical comorbidities was obtained. Comorbidities associated with cold intolerance were screened for in order to assess for bias and any correlation. A further option was given in free text to allow participants to volunteer any other comorbidities that may be relevant.
Exposure to conditions below 10°C has previously been associated with a significantly higher risk of cold injury and is commonly used as the definition of cold exposure.14,15 Historical meteorological office data were consulted to identify for which months the mean air temperature was <10°C. These data were used to define a time period during which outdoor sports would have resulted in cold exposure; this was found to be between November and March. A cumulative exposure to cold was estimated by multiplying the number of years spent participating in paddle sports during this time period, with the number of times the activity was completed in a week and the average length of the activity in hours.
Data on the use of protective clothing and what conditions prompted users to wear it were collected. Protective clothing was considered to be anything covering the hands, preventing exposure to cold air; this included gloves, mitts, or specific hand coverings that attach to the paddle shaft, termed “pogies” or paddle mitts.
Previous studies have defined NFCI as a history of significant cold exposure causing sensory symptoms in an extremity lasting over 30 min and as often painful upon rewarming. 1 Should participants report episodes with symptoms fitting these criteria, they were considered to have sustained an acute NFCI. Chronic NFCI is not as well defined, but the most common symptom reported is that of cold intolerance.1,6 The cold intolerance severity score (CISS) has not been validated as a tool for the diagnosis of chronic NFCI. However, it is an established and validated method for the assessment of cold intolerance. 16 CISS was calculated using the method outlined in Table 1 to quantify symptoms reported by respondents rather than for the diagnosis of chronic NFCI. Two previous studies investigated the CISS of a normal population. They defined the upper 95th percentile as having pathological rather than physiological symptoms of cold intolerance. One study found this to be 30 and the other 50.17,18 The higher of the 2 published values was used to avoid a type 1 error. Therefore, for the purposes of this study, a CISS of >50 was defined as pathological.
Cold intolerance severity score
Data were analyzed using SPSS statistics program version 24. Nominal variables are presented as proportions. Numerical variables were tested for normality and presented as either mean or median with interquartile range, as appropriate. Univariate analysis was performed to determine which demographic and cold exposure-related factors were associated with a higher CISS. For nominal variables this was performed using a Mann-Whitney U test or Kruskall-Wallis analysis of variance, as appropriate. Chi-squared analysis was performed for each variable to correlate it with a pathological CISS, defined as >50. Numerical variables were correlated through the calculation of a Pearson rank coefficient. Multivariate analysis was performed by constructing a binary logistic regression model to identify any correlations between demographic and cold exposure factors and a pathological CISS. Based on existing literature, this was defined as a CISS ≥50 to generate odds ratios for developing a pathological cold intolerance adjusting for the above variables. A P value of <0.05 was considered statistically significant.
Results
The survey was completed by 609 paddlers. The results are summarized in Table 2. Almost 95% of participants undertook activity during cold conditions (n=576), with the majority (78%) having over 2 h of cold exposure per week for an average of 12 y. Between 60 and 75% report either pain or numbness to their hands upon cold exposure, occurring at least weekly in 60% of participants. Twenty-three percent report ongoing pain and edema lasting over 30 min after their hands had been rewarmed, consistent with an acute NFCI (Table 2). Overall, the median CISS was 31 (interquartile range 25–43), and 15% (86) of participants had a CISS of over 50.
Survey results summarizing participant demographic characteristics, cold exposure activity, and symptoms upon cold exposure
Data are presented as n (%) or median (IQR).
Univariate analysis was performed for each variable to determine its correlation with CISS. Among the demographic characteristics, female sex was associated with a significantly higher CISS in comparison to male sex (male 25.5: female 40, P<0.05). Those with Raynaud’s phenomenon or migraines also had a significantly higher CISS (Raynaud’s 46 vs no Raynaud’s 28, P<0.005; migraines 37.5 vs no migraines 29, P=0.002). A significantly higher proportion of females, smokers, and those with Raynaud’s phenomenon or migraines had a pathological CISS (27% females, 30% smokers [P=0.04], 40% Raynaud’s phenomenon [P<0.005], 27% migraines [P=0.03, Table 3]).
Univariate analysis of cold intolerance severity scores for demographic and activity variables
Factors with statistical significance have been highlighted in bold.
ANOVA, analysis of variance; CISS, cold intolerance severity score; KWA, Kruskall Wallis ANOVA; MWU, Mann Whitney U test.
There was no significant difference in CISS between those who undertook activity during cold conditions and those who did not (P=0.15) (Table 3). Cumulative cold exposure did not correlate with CISS (Pearson r=–0.03 P=0.47) (Figure 1). However, the choice of clothing did correlate with CISS. Those who wore protective clothing in warmer temperatures had a significantly higher CISS than those who did not (P<0.005) (Table 3).
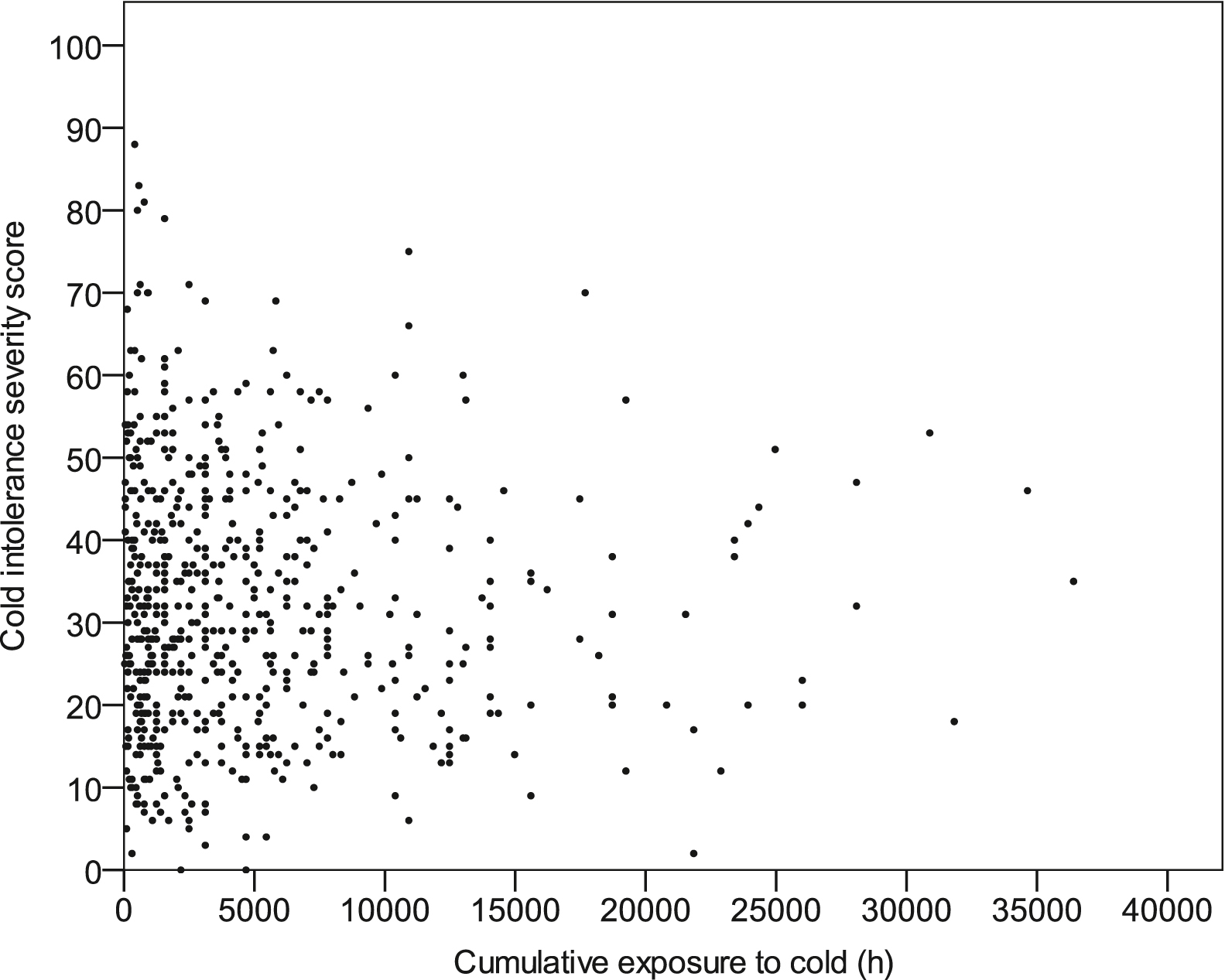
Scatterplot correlating cold intolerance severity score with cumulative cold exposure.
A binary logistic regression model was constructed defining a CISS of >50 as pathological to identify any correlations between either demographic or activity variables and a pathological CISS (Table 4). Female individuals were 3.5 times more likely to have a pathological CISS. Other factors significantly associated with a pathological CISS were smoking (OR 4.8), previous nerve injury (OR 4.7), and Raynaud’s phenomenon (OR 5.3).
Binary logistic regression identifying factors associated with a pathological cold intolerance severity score (>50)
P<.0005. Nagelkerke R2=0.293. Variables with few events per variable, such as Asian/Afro-Caribbean ethnicity, diabetes, Dupuytren’s, hand arm vibration syndrome (HAVS), peripheral neuropathy, and peripheral vascular disease, are excluded due to sparsity of data.
Factors with statistical significance have been highlighted in bold.
Discussion
This was an epidemiological study performed on paddlesport athletes with a wide age range and varied time spent undertaking paddlesport, at varied intensity, from recreational paddlers having occasional exposure to those spending over 20 h·wk-1 exposed to cold conditions. This is likely to be representative of the population within the United Kingdom that undertakes paddlesport.
We have found that a large proportion (23%) report episodes consistent with NFCI. Our findings also suggest that paddlers have a significantly higher CISS than a normal population; 14% reported a pathological CISS score of >50 in comparison to 5% reported by other studies performed on the general population.17,18 There was no correlation between cumulative cold exposure and the development of cold intolerance. Females and those with either Raynaud’s phenomenon or migraines had a significantly higher CISS. Regression analysis found that the only significant risk factors for developing pathological cold intolerance were female sex, smoking, or having medical comorbidities, specifically Raynaud’s phenomenon or a nerve injury.
Females were at significant higher risk (odds ratio 3.5) of developing pathological cold intolerance. The relationship between female sex and cold sensitivity is well described, with many possible contributing factors from vascular to homornal and neural mechanisms.13,14,19 Males have larger hands and a higher body mass index, which are thought to be protective against cold injuries. 13 The female vasculature is also thought to be of smaller diameter with a higher resting sympathetic tone, resulting in reduced resting digital blood flow. 20 Hormonal factors may also have a role; high levels of estrogen are associated with other vasospastic disorders such as Raynaud’s phenomenon, and estrogen has been directly linked to increased adrenoceptor-mediated vasoconstriction. 21 Finally, some studies suggest that females report pain differently; females not only have a higher density of cutaneous nerve fibers but also greater temporal summation of painful stimuli.19,22
Smokers and those with Raynaud’s phenomenon or a prior nerve injury also had a significantly higher risk of developing pathological cold intolerance. NFCI and cold intolerance are thought to be due to neurovascular dysfunction, which shares a pathophysiological mechanism with the aforementioned conditions. 9 The correlation between Raynaud’s phenomenon and pathological cold intolerance is well described and unsurprising, given that both have overlapping symptoms that are induced by cold exposure and so would result in a high CISS regardless of the etiology. Smoking is known to cause peripheral vascular disease with subsequent constriction of the peripheral vascular through atherosclerosis. 23 Nicotine has been shown to alter the metabolic and hormonal responses to cold exposure.23,24
Those with migraines had a significantly higher CISS and pathological cold intolerance upon univariate analysis; regression analysis did not find this correlation to be statistically significant. Migraines are also thought to be a neurovascular disorder. Changes in cerebral blood flow have been observed in those suffering from migraines, and vasoactive medications such as triptans can also be effective for relief of symptoms. 25 Migraines have been associated with cold intolerance and other vascular disorders such as Raynaud’s phenomenon, peripheral vascular disease, and coronary artery spasm. 13 They are also more common in women and can be precipitated by menstruation, stress, or sleep deprivation, thus suggesting not only neurovascular but also hormonal factors in its etiology, similar to those described for Raynaud’s phenomenon.13,25,26
There was no correlation between cumulative cold exposure and cold intolerance found in this study. This is in contrast to previous studies finding a positive relationship between cold exposure and intolerance.5,11,13 This may be due to the effect of self-selection among paddlers, with those who suffer from significant cold intolerance choosing not to participate in paddlesports. Exercise is thought to be protective against cold injury, and the correlation between cold exposure and intolerance has been observed in populations undertaking more static duties. Exertion raises the core body temperature and enhances the cold-induced vasodilation response, both of which are thought to prevent peripheral cold injury. 27 Other sources of cold exposure and data to evaluate exertion were not collected in this study, preventing the effect of exercise from being analyzed. Many participants had significant cold exposure over many years, yet had a low CISS, suggesting that genetic and physical attributes may be the significant determinants of developing chronic cold intolerance rather than the duration of cold exposure itself.
Both the Wilderness Medical Society and the American College of Sports Medicine have made recommendations for the management and prevention of cold injuries.28,29 Primary prevention is the recommended approach, given the limited treatment options. Principally, these are maintaining peripheral perfusion through adequate clothing, nutrition, and hydration. Appropriately assessing and compensating for current weather conditions when choosing appropriate protective clothing is important. Common practice among paddlesport athletes is to use protective clothing during the winter months, notably when the air temperature drops below 5°C. It is accepted that individuals personally decide what clothing is appropriate for them and the nature of the activity. A greater understanding of the long-term risk linked with NFCI within paddlesport would be pivotal to assist in national governing bodies’ advice and guidance around participating in activities during winter months.
Limitations
The self-reporting, self-selecting, and retrospective design of the study does limit the conclusions that can be drawn due to potential selection and recall bias. The size of the study population is unknown. The number of people undertaking paddlesports in cold conditions cannot be calculated and hence neither can incidence. Participants were required to estimate their weekly exposure over many years, the variable nature of activity and the time frame in which it was undertaken will prevent accurate reporting of data. Participants were therefore provided with time categories to aid their estimation. This combined with recall bias will prevent accurate reporting of exposure and as such can only be used as an estimate. Releasing the survey online allowed it to be disseminated widely and generated a large number of responses but prevents a response rate from being calculated.
Despite a large sample size in comparison to existing studies on the topic, analysis of certain variables was limited due to their rarity and the resultant low numbers within the study population. Such low numbers resulted in certain variables being excluded from regression analysis to avoid rare-event bias, thus limiting both the statistical power of the study and the strength of conclusions that can be drawn from it. For example, the predominantly Caucasian population of the study prevented any analysis on the effect of ethnicity, a factor well known to impact the risk of NFCI and cold intolerance. 11
Future research by undertaking a larger study recruiting participants across multiple sports that have similar exposure, such as sailing, rowing, or surfing, would allow more detailed analysis and confidence in the conclusions drawn. Furthermore, the inclusion of a control group of similar age, sex, ethnicity, and comorbid status would help quantify the relative risk of developing cold intolerance due to participation in paddlesports.
Conclusions
A large proportion of paddlesport athletes undertaking activity in cold conditions have symptoms of cold intolerance or episodes consistent with an NFCI. Cumulative cold exposure was not associated with developing a pathologically high CISS. The only significant risk factors were female sex, smoking, and Raynaud’s phenomenon or nerve injury. Further research looking into the effect of preventative measures, such as protective clothing, would be beneficial to the paddlesport community.
Footnotes
Acknowledgements
Acknowledgments: The authors thank Sandra Owdziej for her contribution in designing the questionnaire and British Canoeing for their support in disseminating the questionnaire.
Author contributions: Study concept and design (BO, LCB, NJ); questionnaire design (all authors); acquisition of data (HB); analysis of data (all authors); drafting of manuscript (BO, HB); revision of manuscript (all authors); approval of final manuscript (all authors).
Financial/Material Support: None.
Disclosures: None.