
Abstract
Introduction
Wildland firefighters (WLFFs) must undergo a 2-wk critical training (CT) period prior to deployment to the field. This stress may result in clinical risks, including severe muscle damage and rhabdomyolysis. We aimed to document the effects of WLFFs’ CT on physiologic markers of muscle damage and soreness.
Methods
Two interagency hotshot crews (n=25) were followed during spring 2022 for 80 h of training. Activity counts as well as records of upper-body (US) and lower-body (LS) muscle soreness were collected daily. Body weight (BW) and skinfold measurements were recorded on Day 1 (D1) and D11 to estimate body fat (BF) and lean body weight (LBW). Blood was collected on D1 and D11 to measure muscle and liver damage markers.
Results
Critical training resulted in significant elevations in creatine kinase (CK) (216.9±57.4 U/L vs 5166.4±1927.8 U/L, P=0.017) and lactate dehydrogenase (LDH) (175.5±4.0 IU/L vs 340.0±42.6 IU/L, P=0.001) despite no significant changes in BW, BF, LBW, cortisol, or testosterone. Main effects of time were seen in US and LS, peaking on D11 (US: 5.2±0.4 cm, P<0.001; LS: 5.5±0.4 cm, P<0.001). Those who spent the most minutes with activity counts of >1500 counts/min showed the greatest increase in CK and LDH.
Conclusions
These data suggest that WLFFs undergo significant physiologic stressors, resulting in muscle soreness and damage during CT, with 6 of the 25 subjects reaching critical levels of serum CK. It appears that much of the muscle damage and soreness occurred because of unaccustomed WLFF job-specific tasks.
Keywords
Introduction
Wildland firefighters (WLFFs) face numerous physical and mental stressors throughout their work that elicit high energy expenditures.1,2 These occupational demands are exacerbated by heat, personal protective equipment, hydration limitations, and sleep deprivation. 3 Preseason fitness is vital to mitigate these physical demands and maintain crew safety during field operations. An 80-h preseason training period, referred to as critical training (CT), is required by interagency hotshot crews (IHCs) to complete qualifications and meet type I certification. 4
Although CT is necessary to ensure adequate seasonal readiness, it frequently represents its own novel stress, resulting in acute muscle soreness and damage. 5 While modest damage may be beneficial for muscular adaptation, debilitating damage can result in delayed-onset muscle soreness (DOMS) and possible development of rhabdomyolysis. 6 Rhabdomyolysis may have potential for permanent muscle, kidney, and cardiovascular damage. There have been 58 confirmed cases of exertional rhabdomyolysis in WLFFs in recent years, which may only represent the most severe cases resulting in hospitalization.7,8 Most of these cases occurred during preseason CT and were associated with intense, occupation-specific exercises.
Despite the importance of early season training, little research has examined the physiologic stress imposed by CT. Previous work from our laboratory identified subclinical elevations in creatine kinase (CK), lactate dehydrogenase (LDH), markers of overreaching, and muscle soreness in 1 IHC during CT. 9 However, since training is not standardized across IHCs, additional sampling is required to determine the representative physiologic stress from CT. Thus, this study examined the impact of 80-h CT on muscle damage, soreness, and overreaching in male and female IHC WLFFs from 2 IHCs.
Methods
A convenience sample of 25 male and female WLFFs was recruited from 2 IHCs in the western region of the United States and monitored for the duration of CT before the 2022 fire season. Institutional review board approval was granted by the University of Montana (#44-20). Participants provided written informed consent and completed a participation readiness questionnaire (PAR-Q+). Upon arrival on the first day of CT, participants completed an informed consent form, PAR-Q+, and a training questionnaire.
Body Weight (BW) and Body Composition
Body weight was recorded each morning in a T-shirt and shorts daily (∼0.25 and 0.5 kg, respectively) to the nearest 10th of a kilogram. Nude BW was estimated by accounting for the weight of the items worn by each individual. Body weight and height were used to calculate body mass index (BMI). Body composition was estimated via a 3-site skinfold method using a calibrated Lange skinfold caliper (Beta Technology, Santa Cruz, CA). The same trained technician took skinfolds in a rotational order by measuring the chest, abdomen, and thigh for men and tricep, suprailium, and thigh for women. Body density was calculated using established sex-specific formulas and converted to body fat (BF) percentages.
Preparedness Questionnaire
Upon arrival on Day 1 (D1), participants completed a questionnaire regarding their past WLFF experience and physical preparedness for the upcoming season, detailing their off-season activity and training history, including the previous 48 h of activity.
Muscle Soreness Scale
Visual analog scales have been established to quantify perceived muscle soreness. 10 Upon arrival each day, participants were asked to assess both upper-body (US) and lower-body (LS) muscular soreness on a continuous 10-cm visual analog pain scale to reflect pain levels (Figure 1). Marks were quantified using a ruler and recorded in centimeters. US and LS were separated due to potential localized differences in soreness dependent on activity (ie, push-ups vs downhill hiking).
A visual analog scale was distributed to participants to assess upper-limb and lower-limb soreness. NRS, numerical rating scale.
Actigraphy
ActiCal activity monitors (MiniMitter, Bend, OR) were placed on the nondominant wrist using a nonremovable wristband as previously described. 11 Activity counts were averaged into 1-min intervals (expressed as counts per minute). Activity counts were divided into 3 intensity ranges: sedentary (0–99 counts/min), light (100–1499 counts/min), and moderate/vigorous (≥1500 counts/min), as has been done previously in this population. 2 Using crew logs, shift time was isolated; activity not related to shift work was eliminated from activity analysis.
Blood Collection and Analysis
Blood was collected following a >12-h fast using a gel-barrier vacutainer to isolate serum. Blood was centrifuged at LabCorp (Laboratory Corporation of America, Burlington, NC) manufacturer settings for 10 min. Following centrifugation, the tubes were placed on ice for <90 min before being taken to the LabCorp facility for analysis. The serum was analyzed for markers related to muscle damage, including CK, LDH, blood urea nitrogen (BUN), creatinine, bilirubin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), cortisol, and alkaline phosphatase (ALP). Additionally, serum was analyzed for testosterone from a subset of individuals (n=12).
Statistical Analysis
Blood markers related to muscle damage and body composition were analyzed using a 2-tailed paired samples t test. One-way repeated-measures analysis of variance was used to analyze muscle soreness. If a main effect of time was seen, a Bonferroni post hoc analysis was completed. Two-tailed Pearson correlations were used to examine relationships. All data are presented as mean±SEM. Analyses were conducted using SPSS data analysis software, version 27 (SPSS Inc, Chicago, IL), with significance set at P <0.05.
Results
Twenty-two men (27.1±1.4 y, 83.3±2.7 kg, and 179.5±1.3 cm) and 3 women (30.0±1.0 y, 65.7±3.4 kg, and 165.1±5.3 cm) completed the CT period. Male and female participants’ data were pooled for the remainder of the analysis.
Preparedness Questionnaire
Twenty-four participants completed the preparedness questionnaire. Participants reported an average of 2.6±0.6 previous seasons of experience as a WLFF. During the off season, they reported spending 2.8±0.3 mo training for the upcoming wildfire season, with 4.4±0.3 d/wk spent training and 72.5±4.4 min per training session. On average, participants reported spending 3.5±0.3 d/wk and 2.3±0.3 d/wk on aerobic and anaerobic training, respectively.
BW and Body Composition
No significant differences were seen in BW, BMI, BF, or lean body weight from before CT to after CT (Table 1).
Body weight and composition alterations before and after wildland firefighter critical training
Values are presented as mean±SEM (n=25).
Muscle Soreness
Twenty participants completed soreness scales for all shift days during CT (days 1-4 and 8-11, days 5-7 were off duty). A main effect of time was seen in US (P<0.001) and LS (P<0.001) (Figure 2).
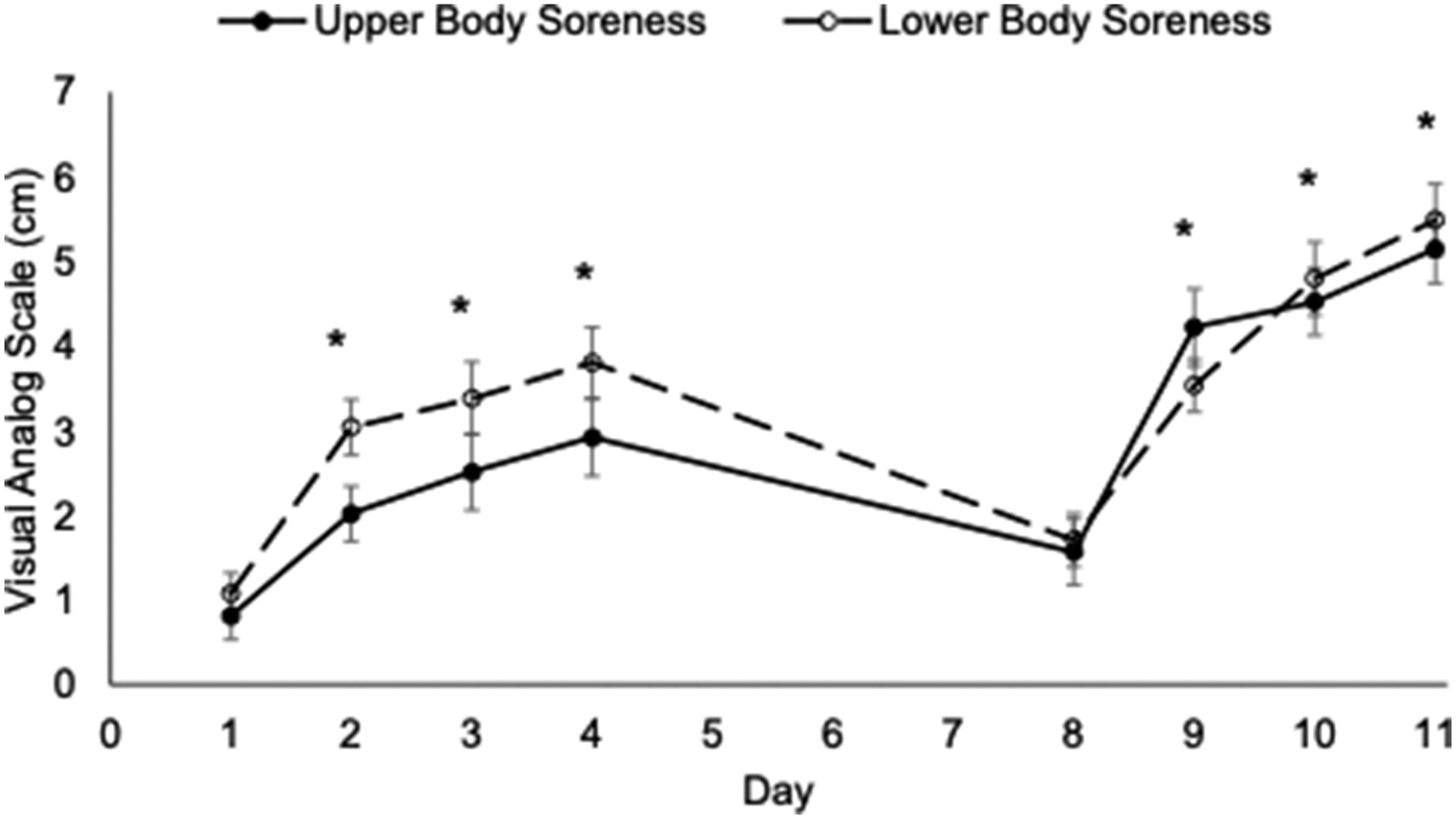
Upper-body and lower-body muscle soreness across 11 d of critical training (n=20). ∗Significant difference from Day 1 (P<0.05). Values are reported as mean±SEM.
Markers of Muscle Damage
Serum markers of muscle damage (Table 2) showed significant increases in CK (P=0.017), LDH (P=0.001), BUN (P=0.002), BUN:creatinine (P=0.001), bilirubin (P=0.029), AST (P=0.004), and ALT (P=0.001) from before CT to after CT. No difference was seen in ALP or creatinine. Importantly, CK and LDH varied considerably; 6 of the 25 participants (24%) demonstrated clinically relevant levels of CK after CT (>5× upper normal limit or >5555 U/L).
Serum markers of muscle damage before and after 80 h of critical training
BUN, blood urea nitrogen.
Range is presented as minimum–maximum.
Significant difference from before critical training (P<0.05).
Markers of Overreaching
No significant differences were seen in cortisol, testosterone, or the T:C ratio from before to after CT (Table 3).
Serum markers of overreaching before and after 80 h of critical training
T:C, testosterone-to-cortisol.
Values are presented as mean±SEM.
Actigraphy
Twenty-four participants had complete activity counts for the entire CT period. Activity data across shift days (D1–D5 and D8–D11) are summarized in Table 4.
Daily activity counts across shift days during wildland firefighter critical training
Values are presented as mean±SEM.
Pearson Correlations
The change (Δ) in CK correlated with the change in other markers of muscle damage, including ΔLDH (R=0.98, P<0.001), ΔAST (R=0.98, P<0.001), ΔALT (R=0.89, P<0.001), and Δbilirubin (R=0.44, P=0.033). Minutes spent doing vigorous activities on D10 were correlated with increases in ΔCK (R=0.53, P=0.008), ΔLDH (R=0.55, P=0.006), and ΔALT (R=0.64, P<0.001). Those who had completed more seasons had lower peak US (R=−0.46, P=0.028). Higher BMI correlated with greater sedentary time across the CT period (R=0.58, P=0.003).
Discussion
This study examined the impact of an 80-h WLFF CT period on markers of muscle soreness and damage in 2 separate IHCs in the western United States. Most telling was the significant elevation in US and LS soreness that corresponded with significant increases in activity counts. The post-CK levels increased by >20 fold. Despite this, none of the WLFF IHC participants sought clinical care or missed a workday. Collectively, these data indicate that CT is a sufficient stimulus to cause impactful physiologic alterations in muscle damage and soreness despite no changes in BW and body composition or increases in markers of overreaching. Many of these detriments were observed following activities that simulated fire suppression in the latter half of CT.
Serum CK and LDH significantly increased from before to after CT, 23.8 and 1.9 times higher than baseline values, respectively. After CT, a serum CK of 5166.4 U/L meets the threshold of 5 times the upper normal limit required for a potential exertional rhabdomyolysis diagnosis. 10 The mean is misleading, as there was significant variability in CK. Of the 25 participants, 52% (n=13) remained within normal limits, 24% (n=6) had elevated CK but did not meet the clinical threshold, and 24% (n=6) exceeded 5 times the upper normal limit. Because of the clinical risk of rhabdomyolysis in participants with CK values of >5555 U/L, 6 they were contacted directly to be on the alert for symptoms of severe muscle pain and cola-colored urine. Amazingly, no secondary symptoms were reported in these participants, and all were able to continue normal training activities. The elevated CK and LDH corresponded with increases in BUN, BUN/creatinine, bilirubin, AST, and ALT. Collectively, this suggests that CT was sufficient to elicit significant muscle damage, including a quarter of the sample at risk for exertional rhabdomyolysis. Despite this, and for the first time in WLFFs, we showed that CK values often associated with clinically manifested rhabdomyolysis did not result in additional symptoms necessary for a diagnosis. Indeed, none of the participants missed a day of CT or the following week’s work.
Muscle soreness is a significant subjective marker of muscle damage; in the current study, muscle soreness was separated into US and LS soreness to isolate specific regions of damage. The data indicate a significant increase in both US and LS, with values peaking on day 11 of training. While similar increases were seen in earlier work by our group, there were marked differences in the timing of these peaks. 9 Typically, DOMS peaks 48 to 72 h after exercise completion and can remain elevated for up to 10 d after exercise, which parallels previous findings from our laboratory. 12 Crew logs reported that day 1 to day 4 of CT focused on general fitness and classroom training, while day 8 to day 11 focused more on occupation-specific activities. This suggests that significant elevations in muscle soreness resulted from a combination of accumulative work and specific occupational responsibilities that simulate fire suppression.
Previous research has established that testosterone and cortisol may indicate the anabolic/catabolic state within athletes, especially men. 13 Serum cortisol and testosterone showed no significant changes from before to after CT; however, a trend was seen in the T:C ratio (P=0.08). While, in general, these data imply that participants could maintain an appropriate anabolic-to-catabolic balance within the body, only 1 of the 2 crews was analyzed for testosterone (n=12). The experimental design did not intend to capture transient alterations in these hormones. Our previous work, which included 4 blood draws over CT, demonstrated a significant increase in the T:C ratio. 9
During CT, daily activity counts average from 781 to 1025 counts/min, with 77 to 226 min spent completing moderate/vigorous activity (>1500 counts/min). This activity is representative of WLFF activity levels previously shown during CT 9 and mimics WLFF activity during seasonal operations. 3 Time spent in the moderate/vigorous activity zone increased by >70% during the second half of CT while crews completed occupation-specific duties such as line construction, building hazard reduction, and active fire suppression. These patterns corresponded with increases in US and LS muscle soreness and elevated blood markers of muscle damage. In fact, moderate-to-vigorous activity on day 10 was positively associated with changes in CK, LDH, and ALT.
Fitness can ameliorate these concerns as muscle tissue adapts to chronic stressors. 9 Despite participants reporting training 4.4 times a week for 2.8 mo, this did not appear to provide adequate protection against muscle damage and soreness. Thus, it may be essential to consider the type and modality of training WLFFs are undertaking. The most consistent modality reported by participants was hiking (45%). While hiking is beneficial for general cardiorespiratory fitness, it might be insufficient for specific fire suppression activities. In fact, a study demonstrated that 40% of shift time was spent hiking, while more significant percentages of time were spent staging, fire suppression, and mop-up activities. 14 Thus, more task-specific training might provide enhanced protection. To support this point, WLFFs with more experience endured less soreness. Together, these data suggest that more task-specific training before CT might attenuate muscle damage and soreness severity.
Limitations
The IHC participants in this study were a convenience sample without a control group. Activities performed by these crews likely do not represent all crews during preseason CT, as CT is not standardized. In fact, 1 of the crews examined was sent on a local fire assignment during CT, which is uncommon. A limitation is the inability to control participant behavior outside of work. Forty-eight hours before CT started, 50% of participants reported abstaining from physical activity, 32% reported light physical activity, and 18% reported moderate-to-heavy physical activity. These variations could contribute to the variability across the CT period. Our sample only contained 3 women (12% of the sample pool). While this is similar to other WLFF-related studies and within the greater WLFF community, it prevents us from identifying any sex-specific differences.2,3,15
Regardless, these data are impactful in a number of ways. Preparatory periods for physically demanding group settings (firefighters, military, team sports, etc) may predispose participants to severe clinical outcomes. This may be due to the inability to mimic the occupational activities during outside training, unique working environment, rapid introduction of novel activities over long days, inability to individualize the training stimulus in a group setting, or simply inadequate preparation prior to arrival. It should be highlighted that not only in our population of WLFFs but also in military, collegiate athletes, and others, the risk of exertional rhabdomyolysis is mainly in the initial days of reporting to duty. 6 Knowledge of this should allow supervisors to monitor clinical manifestations. These data also add to a growing body of evidence that extremely elevated serum CK is not an absolute marker of clinical risk. 16 This suggests that many potential cases in these at-risk populations go unreported and may be on the verge of development of exertional rhabdomyolysis. The key symptom that results in clinical manifestations remains to be determined, but continued kidney function (adequate hydration with frequent urination) may be protective.
Conclusions
This study confirms that CT provides a significant physiologic stressor to elicit changes in muscle damage and soreness. In this elite IHC population, markers of muscle damage suggested clinical significance in 24% of the individuals despite no clinical manifestation of rhabdomyolysis. However, it highlights the need for careful monitoring of WLFFs throughout CT to ensure crew safety. Those with greater preseason training appeared protected from these detriments, emphasizing adequate preparation prior to CT. It is well known that muscle damage occurs from novel bouts of exercise; therefore, preparation and gradual progression are important in the avoidance of clinical risk. It may be prudent to think of WLFF CT not as a chance to get into shape but more as an opportunity to hone the skills necessary for this high-risk occupation.
Footnotes
Acknowledgements
Acknowledgments: The authors thank the participating fire crew members for their time and effort. Special gratitude is extended to Molly West and Skylar Brown for their data collection efforts. The results of this study are presented clearly and honestly and without fabrication, falsification, or inappropriate data manipulation.
Author Contributions: study concept and design (KSC, JAS, SCG, CLD); obtaining funding (JAS, CLD); acquisition of the data (JAS, SCG); analysis of the data (KSC, CLD); drafting of the manuscript (KSC, CLD); critical revision of the manuscript (KSC, JAS, SCG, CLD); approval of the final manuscript (KSC, JAS, SCG, CLD).
Financial/Material Support: This study was funded by the US Forest Service (16-CR-11138200-005). The authors report no potential conflicts of interest.
Disclosures: The authors declare that they have no competing interests in access to these data or associations with companies involved with the products used in this research. The views and conclusions contained herein are those of the authors and should not be interpreted as necessarily representing the official policies or endorsements, either expressed or implied, of the US Department of Agriculture, Forest Service, the National Wildfire Coordination Group, or the Department of Interior.