
Abstract
John Hayward, PhD (1937–2012), was an early and significant contributor to the understanding of cold water immersion physiology and survival. This article summarizes his work on the 50th anniversary of his first publication in this area. He described areas of high heat loss and emphasized the importance of protecting these areas during cold exposure using the Heat Escape Lessening Posture (HELP) and the potential for heat donation to these areas during rewarming. He described several factors that affect the rate of core cooling, including body composition, behavior (swimming increases cooling whereas the HELP position decreases cooling), wet and wind, and thermal protective garments (dry suits offered much more protection than wet suits). Hayward determined breath-hold duration in children as young as 4 y and had his own heart catheterized for 3 d to complete 3 hypothermia rewarming trials. His work provided early understanding of the cold shock response and ways to mitigate its threat to survival. Hayward provided valuable contributions to prediction models for heat production, heat loss, and core cooling rates in cold water. He also developed a human model for severe hypothermia and patented the UVic Thermofloat Jacket. Finally, as evidence of his stature in the cold physiology community, Hayward was a coauthor of the initial State of Alaska guidelines for the treatment of hypothermia. John Hayward was truly a cold water pioneer.
Introduction
In 1975, the University of Victoria (Canada) published a brochure, Man in Cold-Water (Figure 1), highlighting the recent work of one of its new professors of biology, John Hayward, PhD. The brochure addressed several cold water–related topics, such as: 1) human studies on physiology and physics of heat loss; the effects of behavior, thermal protection, and alcohol on heat loss; and early references to the cold shock response; and 2) mathematical prediction of shivering heat production and core cooling in cold water. Importantly, the brochure introduced the UVic Thermofloat Jacket, a patented design that was at the forefront of thermoprotective garments for cold water survival. This brochure was significant for 3 reasons: 1) Hayward had only started studying human cold exposure since arriving at the University of Victoria in 1969; 2) most of the topics came from 3 articles published in 1973 1 and 1975,2,3 and the remainder came from soon-to-be-published data or future work; and 3) all but a few conclusions have stood the test of time and still make up the foundation for what is currently taught about cold water immersion half a century later. We are unaware of any attempt to summarize the scientific contributions of this trailblazer in cold water safety and survival.
Cover pages of brochure “Man in Cold Water,” published by the University of Victoria in 1975.
John Stanley Hayward, PhD (1937–2012), initially published 20 articles on temperature regulation in animals in the 1960s. He then started his innovative work on human responses to extreme environmental conditions in the 1970s. Hayward’s research program followed a logical progression from describing long-term and acute responses to cold water immersion, to determining factors affecting core cooling rates in cold water, to treating cold individuals, and finally to contributing to guidelines for handling cold patients in prehospital scenarios. Following his retirement in 1992, he continued to inspire research and to publish articles (see Table 1 for brief summaries of all related articles). 1 -23
Summaries of cold–related human studies by Hayward and colleagues grouped in topic areas.
CWI, cold water immersion; BHD, breath-hold duration; HELP, Heat Escape Lessening Posture; Tco, core temperature; Twater, water temperature; Tsk, skin temperature.
Long-term Responses to Cold Water Immersion
The year 2023 is the 50th anniversary of Hayward’s first publication involving human subjects 1 (on 4 males and 1 female, including the authors), which provided valuable infrared thermography to illustrate the regional differences in skin temperature, and therefore heat loss, after being still or swimming in cold water (Figure 2). These thermographs revealed areas of highest heat loss in the axillae, groin, and neck where large blood and lymph vessels pass close to the skin. This article provided early indications that heat loss increases considerably during muscular exercise, such as swimming, compared with being still (Figure 2, panel c vs panel b). 1 The results were also valuable in recognizing that areas of high heat loss could also be targeted for heat donation to the core during rewarming. This information also influenced future work on the design of the UVic Thermofloat Jacket (see Figure 1).
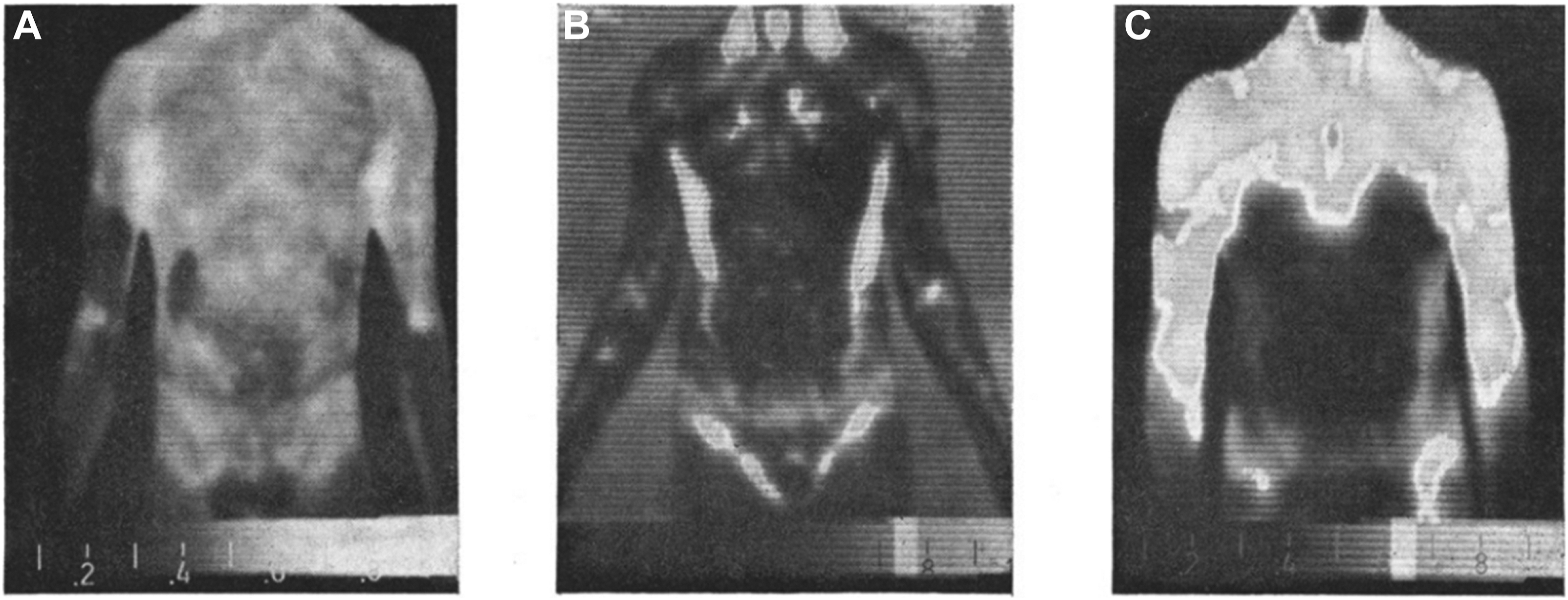
Infrared thermographs illustrating temperature distribution of the front of a male subject before immersion in 7.5°C water (a), after holding still in the water for 15 min (b), and after swimming for 15 min (c). 1
Hayward’s group demonstrated that core temperature (Tco) increased for the first 10 to 20 min of cold water immersion before starting to decrease. 4 They also demonstrated an initial spike in metabolism upon immersion followed by a gradual increase until a plateau was reached. This study also developed a prediction equation for shivering heat production, which had an inverse linear relationship with Tco. This relationship described a linear “gain” to the response. This and other studies provided early parameters for thermoregulatory responses, which include threshold for response onset, response gain, and the maximum response (these terms also apply to sweating and vasomotion).
Hayward also studied the effect of hypothermia on brain electrical activity. 5 The study determined that brain electrical activity begins to significantly decline only at or below a Tco of 33.5°C. This is useful in understanding the cognitive impairments of patients experiencing mild hypothermia (Tco, 32–35°C).
One of Hayward’s more creative works was his research on wet-wind-cold exposure. 6 He built a 25-m “Wet Walk” track on his own property. The track was sheltered by a weather-protective cover that simulated adverse conditions with a rain-generating sprinkler system and large fans. The participants attempted to walk in this track at 5°C for 5 h. After 1 h, either wind (control) or wind and rain were turned on. All 16 subjects completed the “no rain” trials, but only 5 could complete the “rain” trials. Results showed that wetness caused an increased metabolic rate (due to shivering) and a drop in core temperature (Figure 3a). 6 The breadth of human variability was also demonstrated, as some subjects reached the cutoff core temperature of 35°C in as little as 2.5 h (Figure 3b). 6
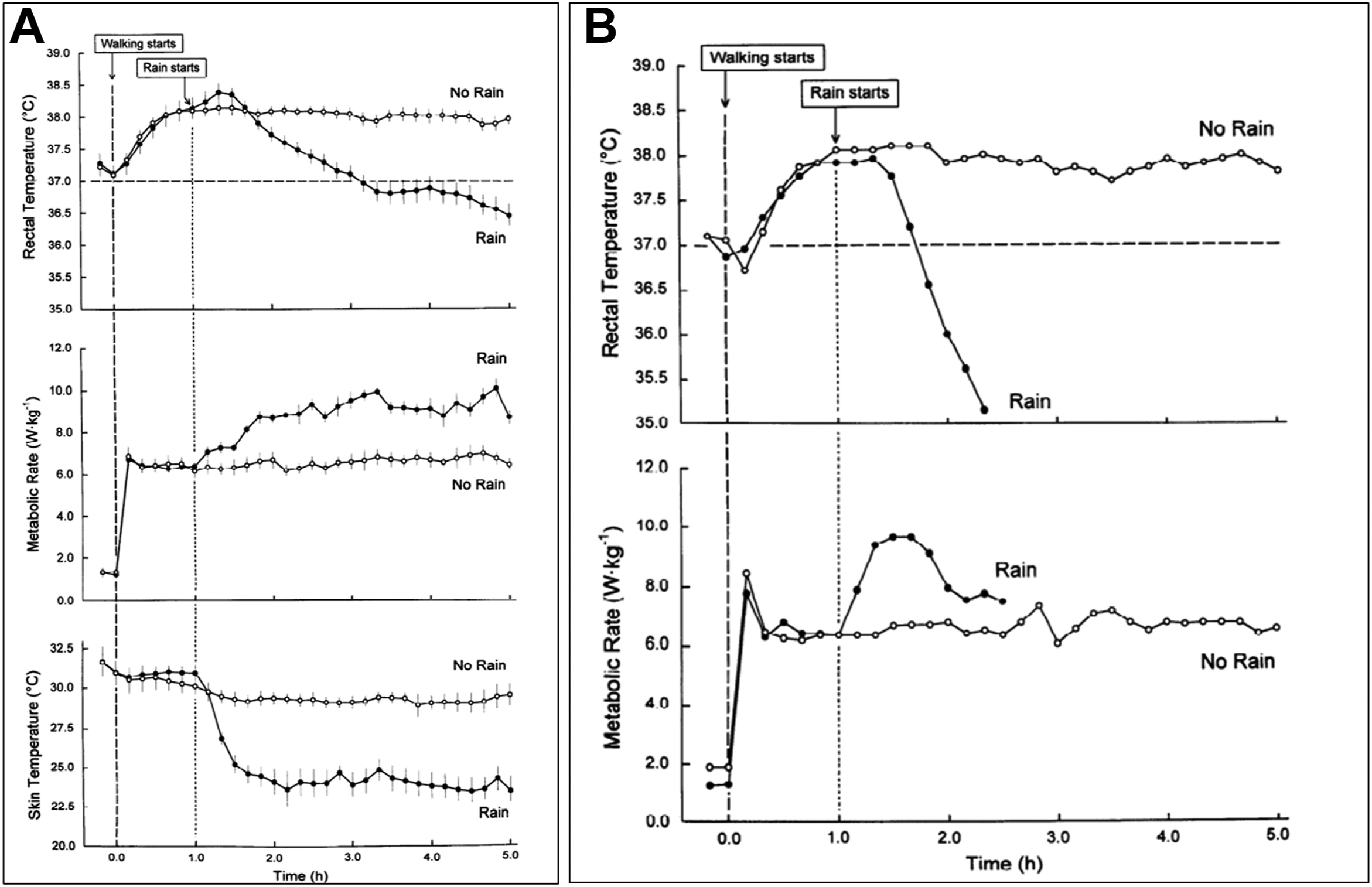
Wet walk. (a) Thermal and metabolic responses of 5 male subjects to wetting by rain while walking at 5.1 km/h in 5°C air (bars, SE). (b) Individual responses for ectomorphic subject experiencing rapid cooling in rain condition. 6
Hayward realized that human cooling studies had a confounding factor of intense shivering. This background heat production prevented the quantification of isolated effects of any source of heat donation on rewarming. As a result, a human model for severe hypothermia was created by pharmacologically inhibiting shivering with meperidine in hypothermic patients. 7 Shivering inhibition resulted in a 3.2-fold increase in core temperature afterdrop and a 4.2-fold increase in duration. These results illustrate the importance of shivering heat production in attenuating postcooling afterdrop, and they laid a groundwork for future research to test methods of rewarming in the absence of shivering.
Acute Responses to Cold Water Immersion—Dive and Cold Shock Responses
In the 1980s, Hayward extended his research to the effect of cold water on the dive and cold shock responses. In 1984, Hayward studied the effect of cold water on the human dive response, which includes breath holding, bradycardia, and redistributing blood flow to the brain. 8 It was previously believed that the dive response improved the survivability of cold water drowning victims because it redistributed a limited oxygen supply to the brain, an effect that increased as water temperature decreased. Children seemed to have increased survivability in cold water drownings, and it was believed this was because of their superior dive response.
On the contrary, Hayward’s research showed that breath-hold duration decreased as water temperature decreased from 35 to 0°C (Figure 4a)8,19; this is now attributed to the cold shock response, which includes gasping followed by hyperventilation. He reasoned that reduced breath-hold duration experienced in cold water likely contributed to drowning through the forced inhalation of water. His research also contradicted previous interpretations that the cardiovascular alterations of the dive response are temperature dependent. He found no difference in heart rate during diving bradycardia in water from 35 to 0°C and concluded that decreased breath-hold duration was a major contribution to cold water drowning. Hayward subsequently concluded that the survivability of cold water drowning victims was dependent on the degree of hypothermia rather than the effectiveness of the dive response. Thus, the advantage of children in cold water drowning was their small body mass, larger surface area-to-mass ratio, and resultant increased core cooling rate.
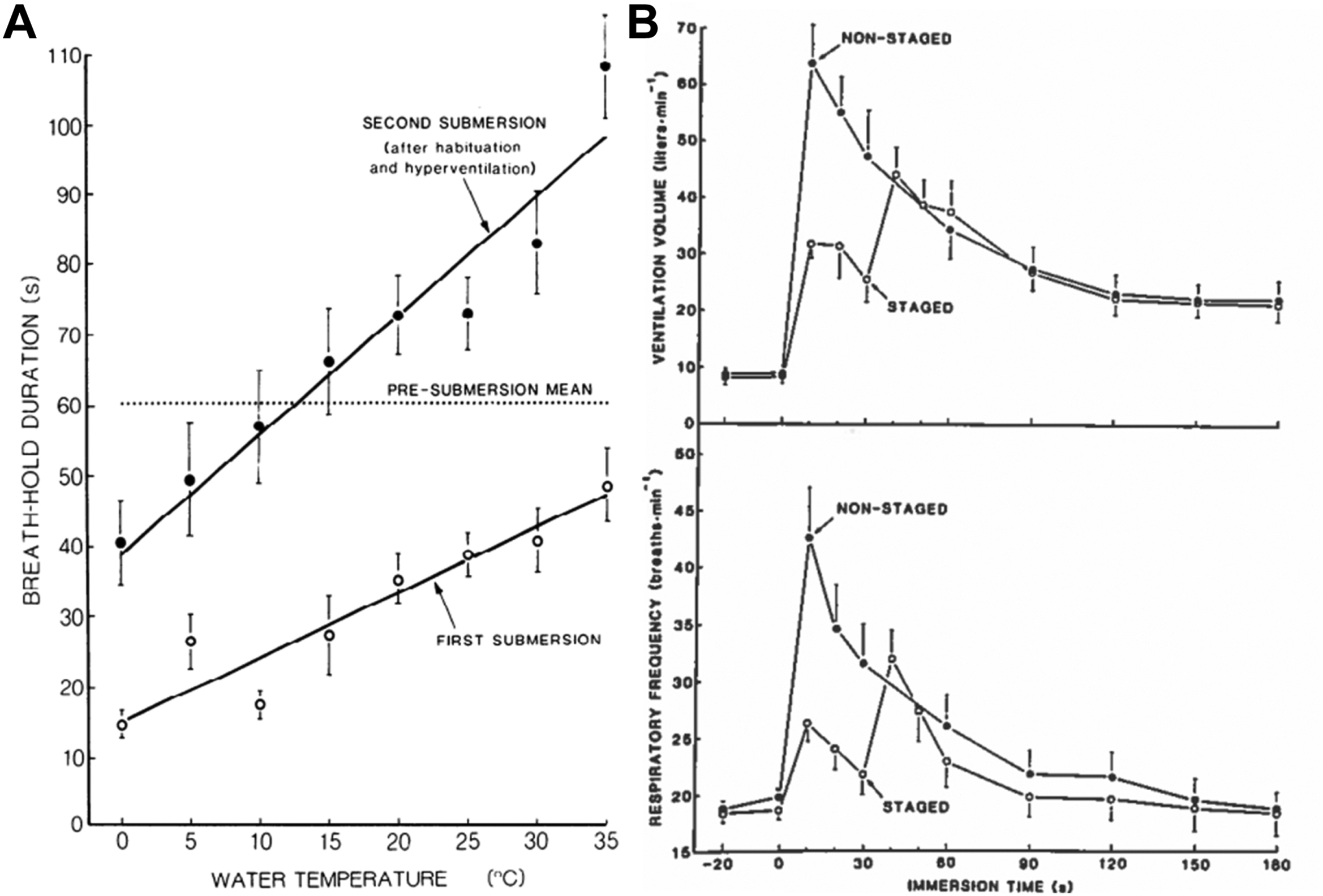
(a) Effect of water temperature on maximum breath-hold duration of humans after a first submersion and then after a second submersion after habituation with 2 min of immersion and 10 s of hyperventilation. 8 (b) Comparison of initial respiratory response to cold water immersion (15°C) to when entry is staged (lower body first immersed for 30 s). 19
In 1987, Hayward went on to compare responses to breath holding in 29°C water between children (4–13 y) and adults (20–70 y). 9 Breath-hold duration decreased with age in the children but not the adults (Figure 5), 9 and the magnitude of diving bradycardia was similar (∼37%) in children and adults. To our knowledge, this study was the first to show objectively that the dive response was not the major factor in improved resuscitation outcomes for children after cold water drowning. Once again, Hayward suggested that increased cooling rates of children (due to their smaller size) explained their improved outcomes because greater brain cooling provided protection under anoxic conditions of drowning.
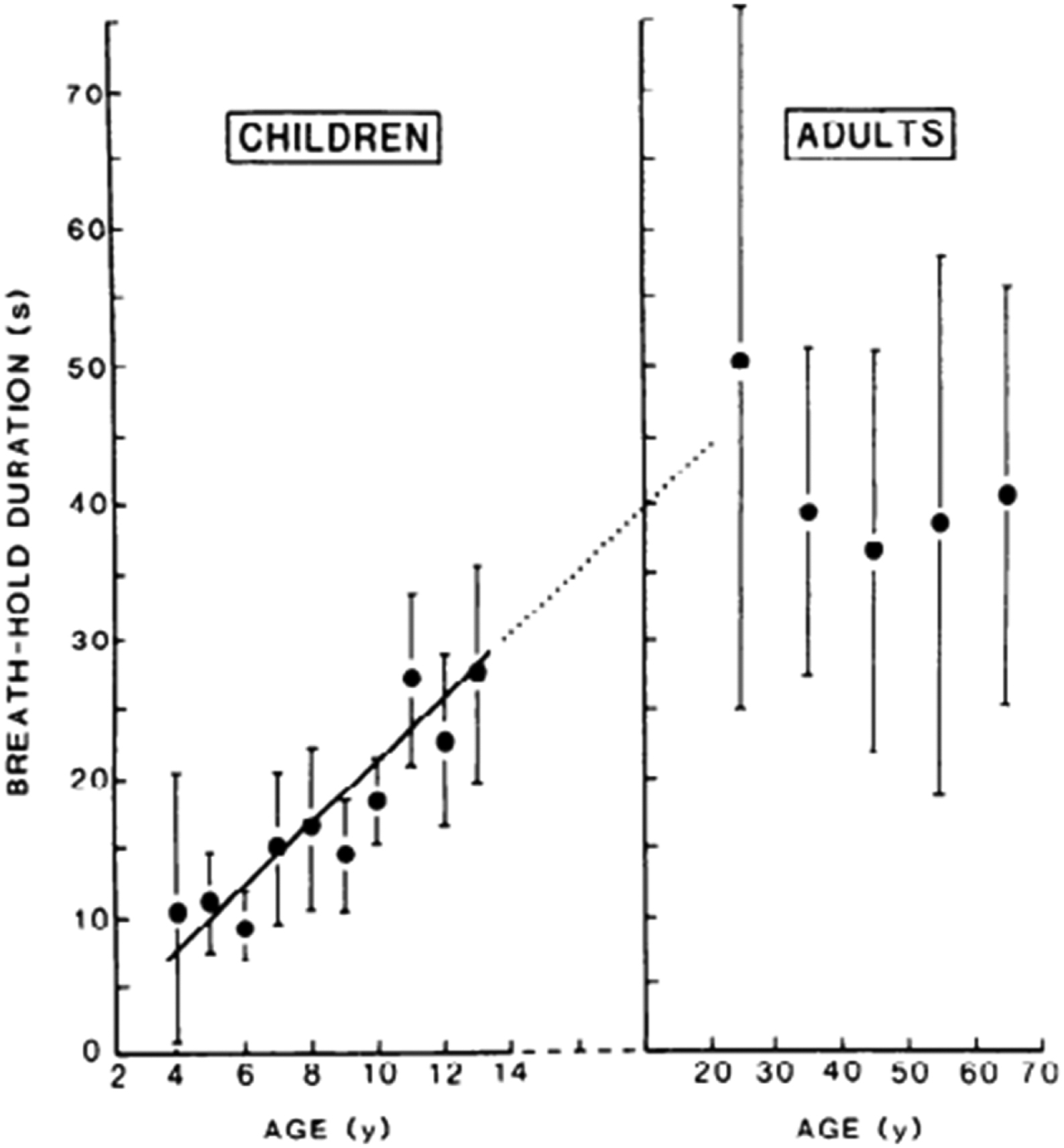
Effect of age on maximum breath-hold duration of children and adults during submersion in 29°C water. 9
Factors Affecting Core Cooling
Hayward’s earliest cooling trials were conducted on males and females in the ocean waters off the coast of Vancouver Island. The first study compared holding still and swimming in 4.6 to 18.2°C water. 2 Although swimming increased metabolic heat production to 250% of resting levels, the core cooling rate increased by 35% compared with holding still. As part of the planned efforts to create prediction equations, Hayward’s group determined that when holding still, metabolic heat production was inversely related to water temperature, and the response was similar to the response to the same air temperature in a low wind condition (2.24 m/s).
The second ocean study compared thermal responses with various behaviors in 9 to 10°C water 3 ; the drawings of these behaviors have been commonly reproduced in related literature throughout the years (Figure 6). Drownproofing and treading water without a personal flotation device (PFD) increased the core cooling rate by 82% and 34%, respectively. Conversely, the Heat Escape Lessening Posture (HELP), which reduces heat loss through high heat loss areas in the axillae and groin), 1 and huddling with 2 other subjects decreased the core cooling rate by 31% and 34%, respectively. These results supported the advice that any swimming in cold water should only be attempted if a PFD is worn.
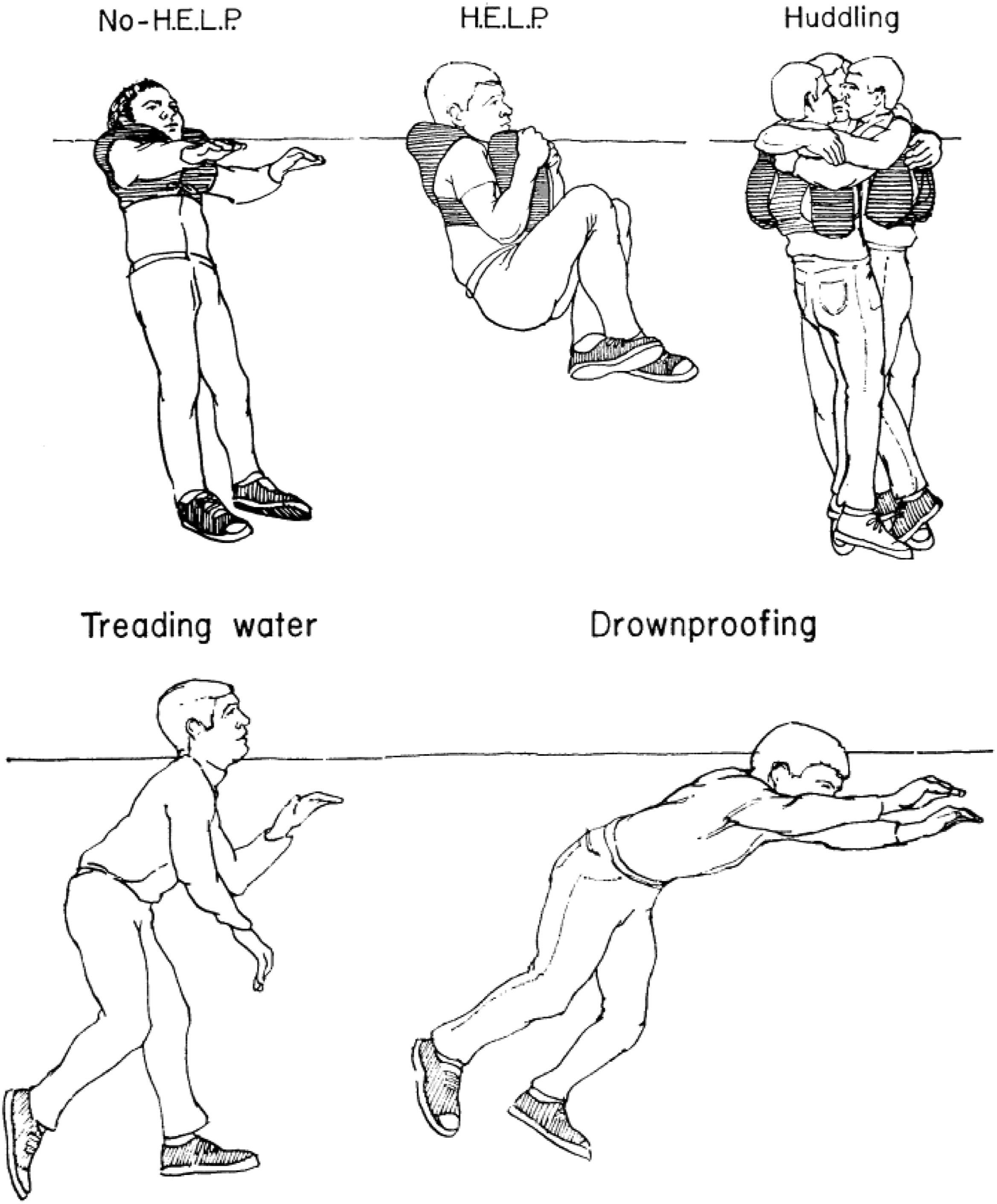
Behavior variables while holding still (a) and while moving (b). 3 HELP, Heat Escape Lessening Posture.
Hayward’s group demonstrated that a blood-alcohol concentration of 82 mb/100 mL decreased heat production in 10°C water by 13%, but this did not affect the core cooling rate, afterdrop, or the core temperature increase during rewarming. 10 They attributed the deleterious effects of alcohol to dangerous behavior rather than to thermoregulatory effects.
Finally, when men and women were immersed in 0°C water, the core cooling rate was negatively correlated to skinfold thickness and endomorphy. 11 However, there was no effect of sex on core cooling rate or metabolic heat production. Part of the explanation for similar cooling rates for the smaller, lighter females was their greater percentage of body fat (20.3% vs 11.5%).
In 1984, Hayward returned to the ocean to study the thermal protection of 5 dry and insulating survival suits during 6 h of immersion in 1°C water. 12 He demonstrated the significant impact that dry and insulating survival suits can have in cold water. Although it is predicted that those without survival suits may only survive approximately 1 to 1.5 h in 1°C water, this study used the overall cooling rate of 0.13°C/h and assumed a lethal Tco of 27°C to predict that those wearing dry and insulative survival suits might survive up to 78 h.
In 1987, in one of his works that had the greatest impact, Hayward collaborated with the US Coast Guard in the first study to determine the impact of rough seas (1–2 m waves with occasional 1.5-m breaks) on the effectiveness of antiexposure suits during immersion in 11°C water for 90 min. 13 Each subject wore each of the garment ensembles, which included 1 uninsulated flight suit (control), 3 loose-fitting wet suit garments, 2 tight-fitting wet suits, and 2 insulated dry suits (Figure 7). 13 Rough seas only increased cooling rates with the 3 loose-fitting wet suits because of increased flushing of water through them. The study confirmed that dry suits were superior in both calm and rough sea conditions and would be preferred for those at risk of accidental cold water immersion.
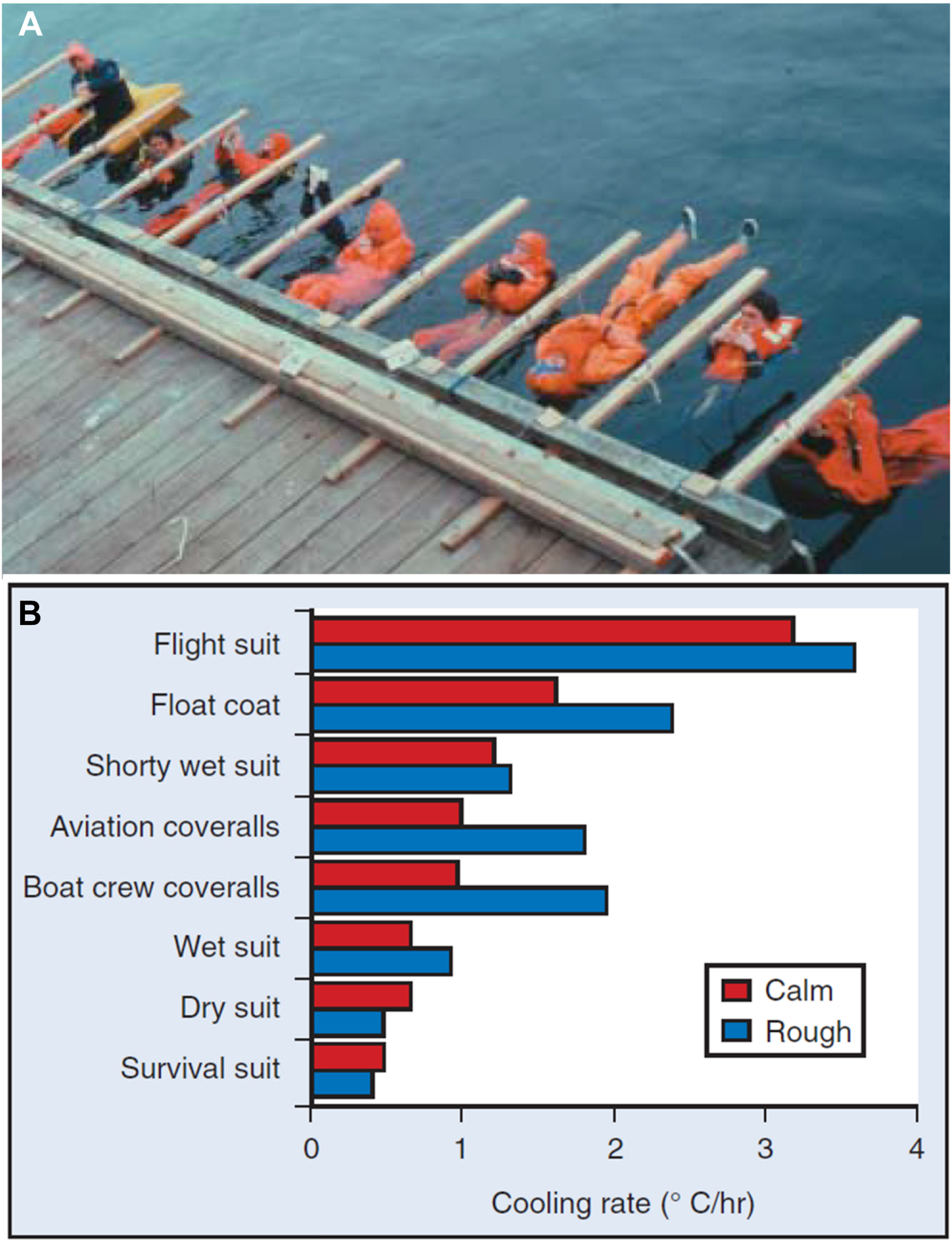
(a) Survival suit testing in the ocean (Photo courtesy of University of Victoria). (b) Comparative core cooling rates for 8 cold protective ensembles in calm and rough water (11°C). 13
Hayward regularly used data from his studies to create predictive equations for cooling and rewarming. Early on, he and his colleagues developed equations to predict core cooling rate, heat loss, and survival time using the single variable of water temperature.2,3 They later used core and skin temperatures to predict metabolic heat production. 4 This group even predicted rewarming rates based on end-cooling core and skin temperature as well as body anthropometry, such as (height/weight)0.5. 14 A final contribution to modeling came from Hayward’s most severe test involving up to 40 min immersion in stirred 0°C water. 11 Final calculations predicted that in 0°C water, it would take 1 to 1.5 h for the average person to reach a Tco of 30°C.
Rewarming Effectiveness
Hayward conducted several studies on the effectiveness of inhalation warming (saturated 45°C air) and warm bath immersion (rapidly warmed from about 30 to 41°C). He felt that inhalation warming could reduce the risk of physiological dangers associated with peripheral vasodilation from external rewarming. In 1975, his first study found no differences in core rewarming rates between inhalation and warm water warming. 15 However, he reasoned that inhalation rewarming was superior for its ability to oxygenate the blood and directly warm the lower brain stem to reverse the cold-induced depression of respiratory and thermoregulatory control centers. Hayward then tried to enhance inhalation warming by having subjects partially rebreathe expired air, increasing minute ventilation to 50 L/min. This technique increased core rewarming by 77% from 1.21 to 2.15°C/h. 16
In his final landmark work on rewarming hypothermic victims, Hayward studied the cardiovascular changes experienced during 3 methods of rewarming. 17 In 1984, Hayward was the lone subject and had a Swan-Ganz catheter inserted into his right pulmonary artery for 3 d. After 3 successive immersions for 100 min in 10°C water, cardiovascular changes were determined during spontaneous warming (no external heat source), inhalation warming, and warm bath immersion. Results confirmed esophageal temperature as an accurate measure of core (heart) temperature (Figure 8a). 17 The study also identified important cardiovascular changes during each of the rewarming techniques, such as a large drop in mean arterial pressure and an increase in heart rate and cardiac output due to peripheral vasodilation in the warm bath (Figure 8b). 17 This resulted in an afterdrop with the warm bath but not with spontaneous and inhalation rewarming. These results confirmed recommendations for rescuers to avoid warm bath immersion.
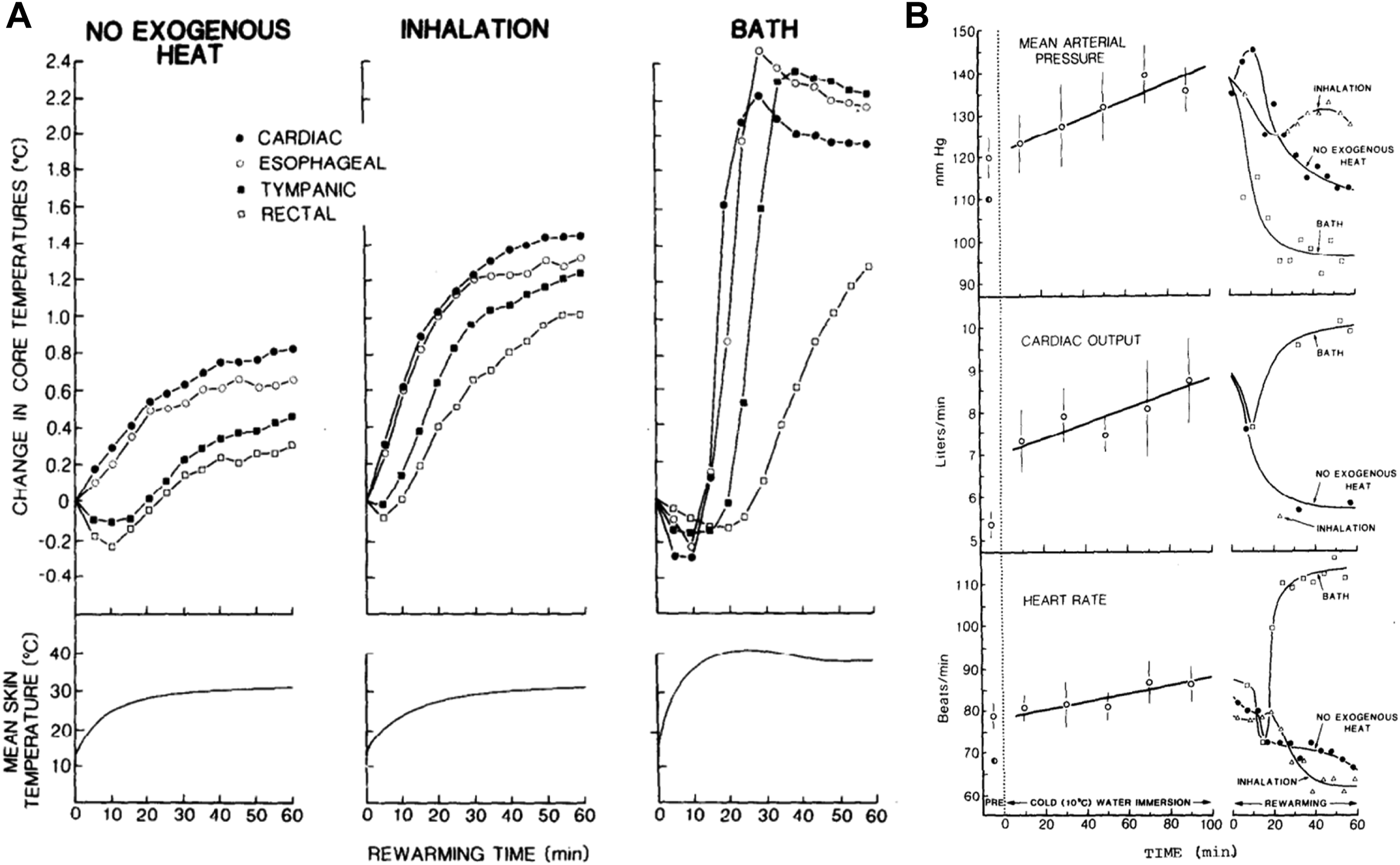
Thermal (a) and cardiovascular (b) responses during cold water immersion and rewarming by 3 procedures. 17
Hayward patented several inventions, but only 1 has stood the test of time. After his early work in the 1970s on heat loss during cold water immersion, Hayward designed the UVic Thermofloat (Figure 1) with Mustang Survival in Vancouver. The novel design included a flap (also termed a “beaver tail”), which could be pulled under the groin and snapped into place on the front. The flap covered the high heat loss areas in the groin, decreased flushing of water within the suit by 50%, and doubled the insulation value of the jacket. In this configuration, the Thermofloat Jacket increased predicted survival time of the average person in 10°C water from 2.7 to 9.5 h.
Conclusion
John Hayward was an early and key contributor to the understanding of cold water immersion physiology and survival. He described the groin and axillae as areas of high heat loss and emphasized the importance of protecting these areas during cold exposure (eg, the HELP position) and the potential for heat donation during rewarming. He determined that the rate of core cooling is inversely proportional to skinfold thickness, is increased by swimming, decreased by assuming the HELP position and wearing thermal protection (dry suits offered much more protection than wet suits), and is not affected by alcohol or sex.
Hayward conducted some studies that might not be repeatable today. For example, he determined breath-hold duration in children as young as 4 y and had his own heart catheterized for 3 d to complete 3 hypothermia rewarming trials. It is important to note that these studies received ethical approval and, at the time, were not considered controversial and were within normal parameters.
He determined that breath-hold duration decreases with age in children but is not age-dependent in adults and that breath-hold duration can be increased by staged immersion or habituation. This work provided an early understanding of the cold shock response and ways to mitigate its threat to survival. He used Swan-Ganz catheterization of the right pulmonary artery and demonstrated the dangers of warm bath immersion because it decreased mean arterial pressure and increased cardiac output and afterdrop of Tco.
Hayward provided valuable contributions to prediction models for heat production, heat loss, and core cooling rates in cold water. He also developed a human model for severe hypothermia and patented the UVic Thermofloat Jacket. Finally, as evidence of his stature in the cold physiology community, Hayward was a coauthor of the initial State of Alaska guidelines for the treatment of hypothermia. 24 John Hayward was truly a cold water pioneer.