
Abstract

Case Presentation
A 21-y-old man was hiking the length of the Appalachian Trail (AT) from its southern terminus at Springer Mountain, Georgia, to its northern terminus at Mount Katahdin, Maine, during the summer after college graduation. By the time he reached the North Carolina section of the AT, he had developed an intensely pruritic, papulovesicular rash with draining pustules confined to a circumferential area around his waist and hips covered by his underwear (Figure 1). He had hiked sections of the AT before as a summer camp counselor and sustained scratches and insect bites while on the trail but had never developed such an extensive and pruritic regional skin eruption. He could no longer continue his trek. He called his sister, who lived in Asheville, North Carolina, on his cell phone, requesting a ride to the nearest urgent care facility.
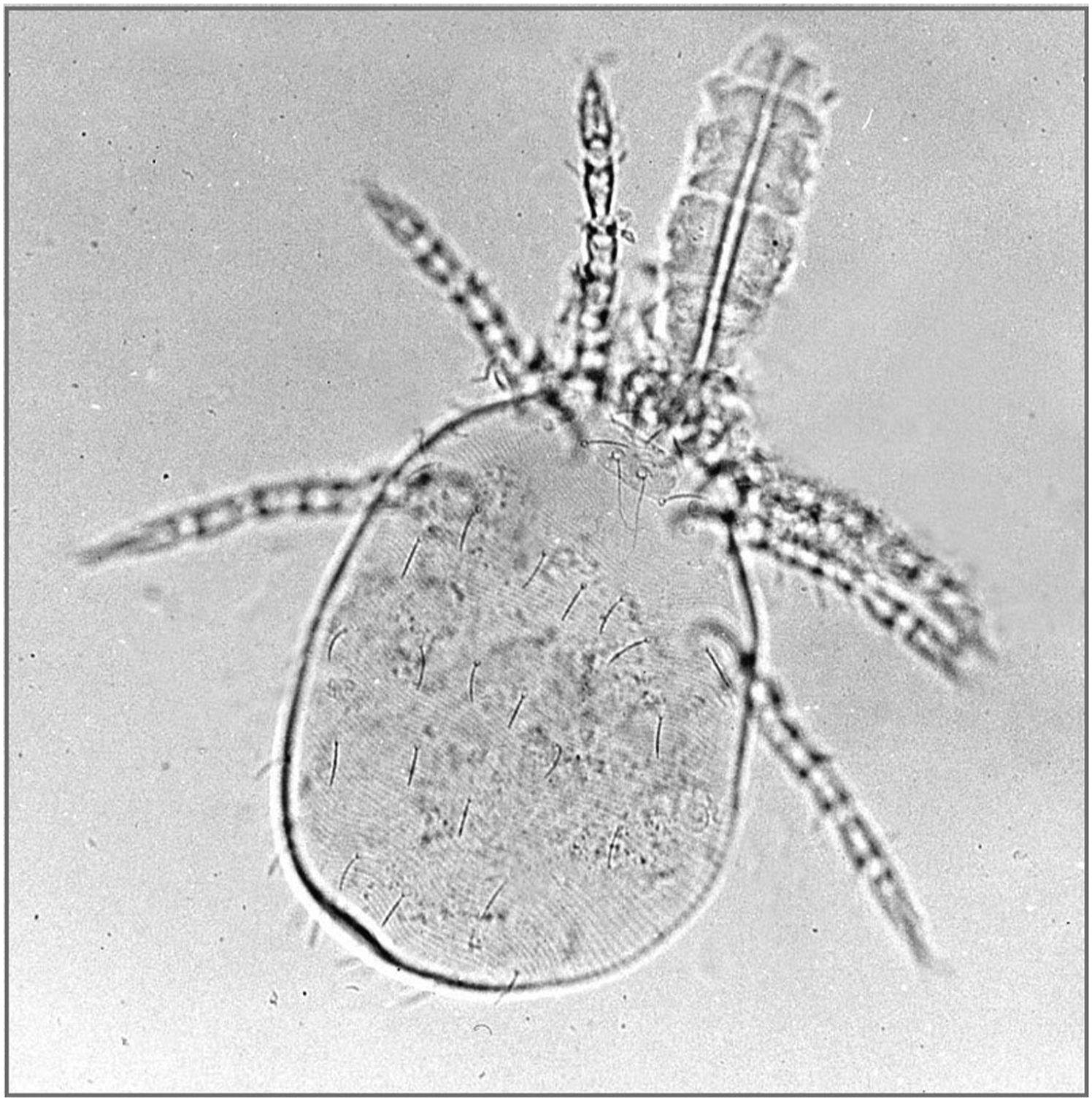
A 6-legged larva of a trombiculid species mite (family Trombiculidae) capable of causing chiggers worldwide. The feathery anterior projection is the mite’s feeding stylostome, which is usually retracted unless feeding. Source: Wikimedia Commons. Photo by Alan R. Walker. Public domain, no copyright permission required. Available at:
Disclaimer: This is a fictitious case based on the author’s experiences hiking the North Carolina section of the AT.
Diagnosis
Chigger bites (trombidiosis).
Management
A physician on duty had observed similar skin conditions in individuals hiking on the AT that summer and diagnosed them with chigger bites with possible impetigo. The physician took diagnostic swab samples of the drainage from the weeping vesicles and pustules for Gram staining and for culture and antibiotic sensitivity testing.
The patient was given hydroxyzine, 50 mg, intramuscularly to control severe itching and provide sedation. The affected areas were washed with antibacterial soap and warm water and dried prior to the application of a topical solution of calamine lotion.
The Gram stain results were positive for staphylococci. Oral empiric therapy for community-acquired methicillin-resistant Staphylococcus aureus (MRSA) was initiated with trimethoprim/sulfamethoxazole (Bactrim), 2 double-strength tablets (160 mg + 800 mg) twice daily for 10 d. Culture and antibiotic sensitivity analysis results from the swab samples were subsequently reported as positive for MRSA and sensitive to trimethoprim/sulfamethoxazole.
The physician counseled the patient on his risk factors for severe immune reactions to chigger bites, including prior exposures while working in hyperendemic regions, perfect environmental conditions supporting chigger mite activity, failure to impregnate clothing and bedding with permethrin, and failure to apply topical N, N-diethyl-meta-toluamide (DEET) or picaridin on exposed skin.
All lesions crusted over by the fourth day, and the hiker resumed his challenging trek, better prepared to prevent another attack by chigger mites.
Discussion
Bites by trombiculid mite larvae (chiggers) can cause trombidiosis and transmit scrub typhus in endemic regions of Asia and northern Australia. However, only larval chigger mites from the genus Leptotrombidium harbor and transmit the rickettsia-like bacterial agent of scrub typhus Orientia tsutsugamuchi. The remaining genera of trombiculid mites can cause chigger bites but do not transmit scrub typhus or other infectious diseases. “Chiggers” is also a colloquial term for trombidiosis, which describes the intensely pruritic clusters of erythematous welts resulting from bites by larval chigger mites.
Definitions and Taxonomy
There are >700 species of chigger mites (family Trombiculidae) in the world, but only about 20 species cause trombidiosis or transmit scrub typhus. 1 In the United States, the term “chiggers” includes immune reactions to bites by the 6-legged larval stage of the American trombiculid mite Eutrombicula alfreddugesi . 1 The other local names for larval trombiculid mites in the United States include jiggers, harvest mites, red bugs, red mites, harvest lice, and mower’s mites. Other indigenous species of trombiculid larval mites cause trombidiosis worldwide (Table 1).
Representative larval trombiculid mites (family Trombiculidae) causing chiggers
Life Cycle
The 8-legged adult female chigger mite lays up to 40 eggs/mo on leaf litter, ground cover, and grasses. 1 The eggs hatch in 1 to 2 wk and, following short prelarval dormant phases, release reddish-colored, mobile, 6-legged larvae, which climb up to 30 cm on plants and vegetation to search for a rodent host (Figure 2). 1 Once the larvae find a host, they feed for 2 to 4 d before dropping off the host and developing into free-ranging nymphs and adults that feed on insects. 1 Adult red chigger mites are <1 mm in length, barely visible without magnification, and usually unnoticed even when they bite humans or feed on zoonotic hosts (Figure 3).

An 8-legged, free-ranging adult trombiculid chigger mite, also known as a red bug or harvest mite, that feeds on insects and insect eggs and does not cause chiggers or transmit scrub typhus in endemic regions. Source: Wikimedia Commons. Photo by André Karwath. Public domain, no copyright permission required. Available at:
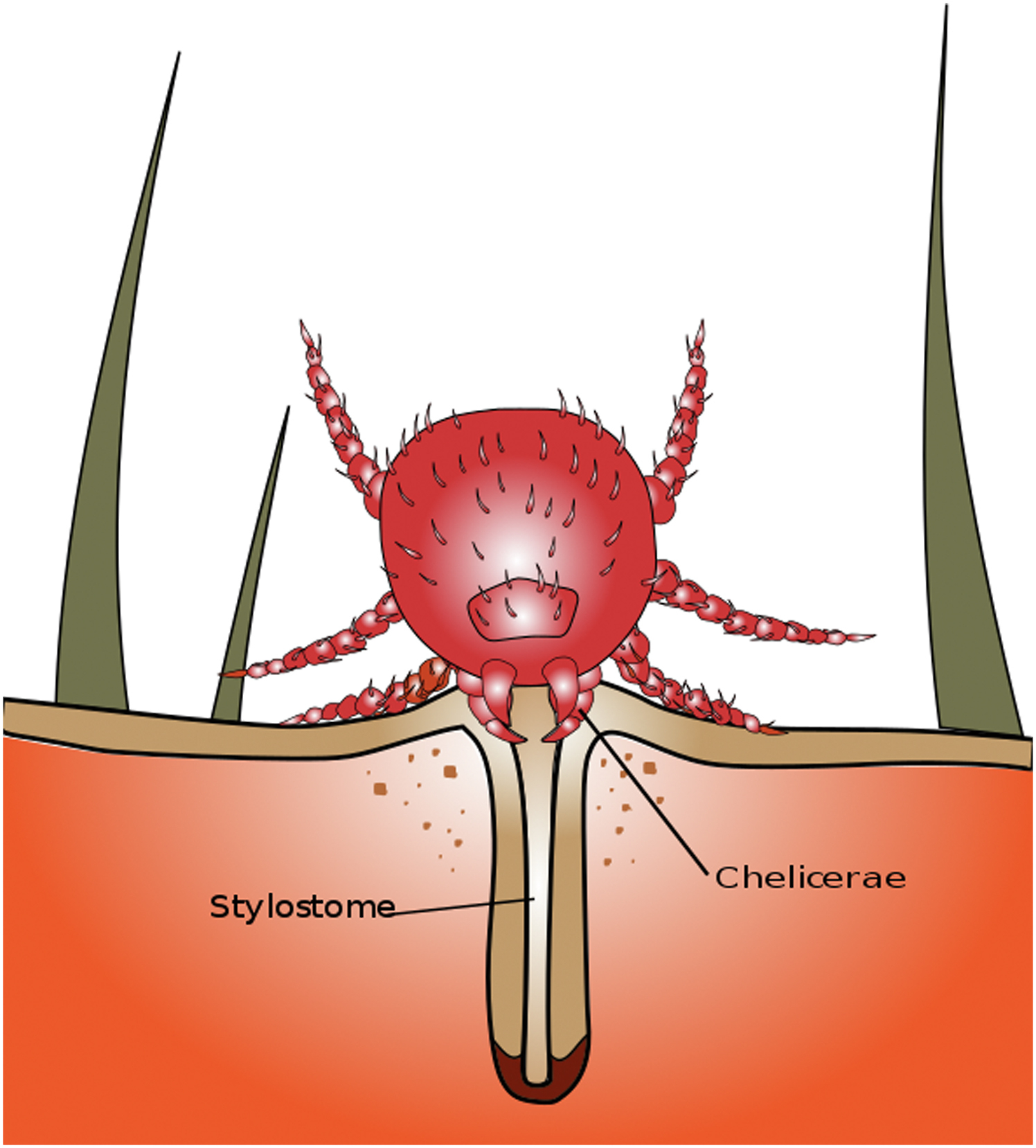
Diagram depicting the feeding position of a trombiculid mite larva with a hollow, straw-like stylostome penetrating deeper under the host’s skin and permitting the siphoning of fresh tissue juices dissolved by salivary enzymes. Source: Wikimedia Commons. Author: Bugboy52.40. Public domain, no copyright permission required. Available at:
Regional Distribution and Ecology
Chigger mites are found in greatest abundance in the southeastern and south-central United States, where environmental conditions support egg laying and maturation and provide a range of rodent and insect hosts. 1 The best seasonal and environmental conditions to support larval feeding and maturation are achieved during summer and early fall, with temperatures between 10°C (50°F) and 32°C (90°F) and a relative humidity of around 80%. 1
Feeding Behavior
Chigger mites do not burrow beneath the skin to feed like scabies mites do. They crawl on the skin to find a suitable area for feeding where the skin is soft, warm, and moist, particularly where clothing is tight and compresses the skin, restricting mite movement. Preferred areas include under waistbands, underwear bands, collars, cuffs, and socks. When ready to bite and feed, chiggers attach their mouthparts at a skin pore or at the base of a hair shaft to initiate a unique manner of feeding on tissue juices using their specialized stylostomes. 2 Unlike ticks, chiggers are tissue juice feeders, not blood feeders. Tissue juices are composed of edema fluid, lymph, and dissolved epithelial cells. 2
Larvae pierce the skin with sharp chelicerae and inject tissue

An intensely pruritic papulovesicular rash with draining pustules confined to a circumferential area around the waist, hips, and genitals, usually covered by underwear. Source: United States Centers for Disease Control and Prevention, Atlanta, GA. Public Health Image Library (PHIL). Image Number 20202. Public domain, no copyright permission required. Available at:
Clinical Manifestations
Initially painless, chigger bites become symptomatic within 3 to 6 h. They often cluster in patterns and progress through a sequence of stages from macules to papules, to papulo-vesicles, to urticarial wheals, and, later, to draining pustules (Figure 1). 1 The lesions become intensely pruritic as they progress and accumulate in areas where clothing impedes mite movement in a downward direction, such as under belts, waistbands, sleeves, socks, and underwear elastic waist and thigh bands. As a result, these groupings may exhibit a circumferential pattern around the wrists, knees, waists, thighs, ankles, toes, male genitalia, and under the elastic bands of undergarments (Figure 5). 1

Clustering of trombiculid mite bites at the ankle, where socks and high-top shoes tightly compress the skin and impede the movement of feeding mites. Source: United States Centers for Disease Control and Prevention, Atlanta, GA. Public Health Image Library (PHIL). Image Number 12069. Public domain, no copyright permission required. Available at:
Patients who have previously experienced chigger bites or have developed significant immune responses to past chigger bites often suffer from severe local bite-site reactions to subsequent chigger bites. These reactions include bullae and weeping pustules and may be misdiagnosed as scabies or bullous pemphigus (Figure 1). 1 A hypersensitivity reaction known as the “summer penile syndrome” has been described in prepubertal boys, usually summertime campers, with multiple circumferential penile and scrotal chigger bites causing significant penile and scrotal edema with intense pain and pruritus. 3
Treatment
The treatment of chigger bites is nonspecific, supportive, and symptomatic, including topical applications of local anesthetics, antiseptics, antipruritics, antihistamines, cooling counterirritants, and corticosteroids. Effective topical anesthetics applied in ointments, creams, foams, or incorporated into or placed under patches include lidocaine, prilocaine, benzocaine, and pramocaine. 1 Effective topical antibiotic ointments for low-grade skin infections, such as impetigo, include 2% mupirocin and bacitracin. Effective antipruritics include oral and parenteral antihistamines, such as diphenhydramine and hydroxyzine, and cooling topical counterirritants, such as calamine, camphor, and menthol. 1 Topical diphenhydramine should not be used because it can cause sensitization, with subsequent allergic reactions to topical or oral diphenhydramine. Temporary occlusion of bite sites by occlusive plastics, collodion, liquid skin, or clear finger nail polish has been reported to increase itching, erythema, and edema. 1 If it is necessary to use an occlusive dressing for prolonged corticosteroid application, these symptoms can be alleviated by covering the dressing with plastic bags filled with ice and inserting a cloth barrier between the ice and dressing to prevent frostbite. 1
In rare cases, intralesional corticosteroids and excision of bite lesions have provided permanent relief when topical and oral treatments have failed to control itching. 4 Low concentrations of corticosteroids between 2.5 and 5.0 mg/mL are recommended for intralesional injections to avoid fat atrophy with permanent skin dimpling.1,4
Complications
Chigger bites may be secondarily infected with common skin contaminants.
Prevention and Control
All mite species have developed very close associations with their supporting ecosystems and preferred zoonotic reservoirs referred to as mite islands. Mite islands typically border cleared land and scrub brush. Environmental requirements include warm soil temperatures with high humidity to support grassy vegetation frequently visited by rodents. Humans stumbling onto or camping within mite islands are at a significantly greater risk of multiple larval chigger bites.
Preventive strategies for chigger bites include avoidance of high-risk mite island areas of grasslands during late summer and early autumn in endemic areas and application of synthetic pyrethroid insecticides, such as permethrin, on clothing, shoes, tents, tarps, hammocks, and sleeping bags. In addition to permethrin-impregnated or -sprayed clothing and bedding, other personal protective measures should include topical applications of 10 to 30% DEET or 10 to 20% picaridin (also known as icaridin) to skin surfaces, especially in high-risk bite areas around the wrists, elbows, waists, knees, and ankles. Combination preparations of insect repellents and sunscreens are not recommended because sunscreens require more frequent applications than insect repellents and may potentiate insect repellant toxicity, especially in children.