
Abstract
Scrub typhus (ST) is an acute focal infectious disease that is caused by Orientia tsutsugamushi. The Asia-Pacific region is an area of relatively high incidence. There is a high incidence in China, principally owing to the disease being endemic in the south of the country. The main source of ST infection is rats, which act as reservoirs of infection after being bitten by the chigger mite, and the human population is generally susceptible to the disease. ST can be controlled and treated successfully if antibiotics are administered in a timely manner. However, because it does not have a specific clinical manifestation, it is difficult to distinguish ST from other febrile diseases in clinical practice. Therefore, rapid diagnostic methods are still needed to help clinicians make a timely diagnosis. Here, we share three cases of patients with ST who experienced hemorrhage, but did not have typical skin lesions, such as eschar and ulcer, early in the course of their disease, and review the relevant literature regarding ST. We conclude that clinicians should pay attention to the risk of hemorrhage associated with this disease, and emphasize the importance of making an early diagnosis.
Introduction
ST is an acute focal infectious disease that is caused by the intracellular parasite Orientia tsutsugamushi. The Asia-Pacific region is an area with a relatively high incidence of endemic ST. In China, the highest incidence of this disease is in the south, and in particular in Guangdong.1,2 The main source of ST infection is rats, which act as reservoirs of the ST pathogen after being bitten by chigger mites. The population of China is generally susceptible, owing to the quantity of agricultural land and the high ratio of rural to urban land. A previous study showed that China has a higher incidence of ST than Japan, South Korea, and Thailand. 3 A systematic evaluation of the mortality rate associated with untreated ST 4 comprising 76 studies of a total of 19,644 patients revealed a range of 0% to 70%, with a median mortality for all the series of <6.0%. ST can be controlled and treated by the timely administration of antibiotics. However, it is difficult to distinguish ST from other febrile diseases in clinical practice because it does not have a specific clinical manifestation. Therefore, additional diagnostic methods are needed to help clinicians make a timely and specific diagnosis. Here, we share the details of three patients who did not have the characteristic eschar and ulcer skin lesions early in the course of ST, but were characterized by hemorrhage. These patients had their disease diagnosed at an early stage, and were treated with doxycycline and other antibiotics in a timely manner. Clinical cure was achieved, and they were discharged. In addition, we review the latest findings regarding ST.
Case presentation
The reporting of this study conforms to the CARE guidelines. 5
Case 1
A nearly 80-year-old man who claimed not to have any chronic diseases developed fever associated with symptoms of a cold. He did not measure his temperature at the time, but his symptoms were chills, paroxysmal dizziness, intermittent chest tightness, and general fatigue, and after approximately 3 days, he attended his community hospital, without having taken any medication beforehand. The physician at the community hospital performed a physical examination and recorded a quick sequential organ failure assessment (qSOFA) score of 2. He did not find any eschar or ulcer lesions of the skin, or any swelling of palpable lymph nodes, but the patient’s breath sounds were loud in both lungs and he had a few moist rales in his right lower lung.
Laboratory testing revealed the following: white blood cell (WBC) count 9.6 × 109/L, neutrophils 86.2%, red blood cell (RBC) count 3.9 × 1012/L, hemoglobin (Hb) concentration 121 g/L, C-reactive protein (CRP) concentration 313.0 nmol/L, serum sodium concentration 122.80 mmol/L, serum calcium concentration 1.08 mmol/L, lactate dehydrogenase (LDH) activity 365.7 U/L, serum a-hydroxybutyrate deaminase activity 260.5 U/L, aspartate aminotransferase (AST) activity 13.0 U/L, alanine aminotransferase (ALT) activity 22.3 U/L, serum albumin (ALB) concentration 502.6 μmol/L, and serum brain natriuretic peptide (BNP) concentration 1,292.1 pg/mL. The patient’s highest temperature after admission was 39.5°C. He was initially administered levofloxacin (0.5 g qd for 2 days) to treat his infection, as well as symptomatic treatment, but this had little effect. A post-hospitalization examination (Table 1) showed that the patient had anemia (Hb 114 g/L), mild liver dysfunction (ALT 52.2 U/L, AST 49.87 U/L, and ALB 341.6 μmol/L), a coagulopathy (activated partial thromboplastin time (APTT) 32.9 s), an electrolyte imbalance (Na+ 117.4 mmol/L, Cl− 86.93 mmol/L, K+ 2.94 mmol/L, and Ca2+ 1.72 mmol/L), and high circulating concentrations of inflammatory indices (procalcitonin (PCT) 1.07 ng/mL and interleukin-6 (IL-6) 46.7 pg/mL); but urine, blood, and sputum cultures were negative for bacteria and fungi. Therefore, the patient was diagnosed with a fever of infectious origin at this time.
Laboratory findings for case 1.

TBIL: total bilirubin; DBIL: direct bilirubin; IBIL: indirect bilirubin; PCT: procalcitonin; RBC: red blood cell; WBC: white blood cell; Hb: hemoglobin concentration; ALT: alanine aminotransferase activity; AST: aspartate aminotransferase activity; ALB: albumin; PT: prothrombin time; APTT: activated partial thromboplastin time; IL-6: interleukin-6; PCT: procalcitonin; CRP: C-reactive protein; BNP: brain natriuretic peptide; G test: 1,3-β-D glucan test; “O”: typhoid bacillus sycosis antigen; “H”: typhoid flagellar antigen; “A”: paratyphoid A flagellar antigen; “B”: paratyphoid B flagellar antigen; “C”: paratyphoid C flagellar antigen.
Cefoperazone sulbactam sodium (3 g q8h for 2 days) and imipenem-cilastatin sodium (1000 mg q8h for 6 days) were empirically administered to treat such an infection. Chest computed tomography (CT) showed inflammation in both lungs and bilateral pleural effusion; therefore, thoracic puncture and drainage was performed. Samples of the pleural effusion were taken for the identification of pathogenic microorganisms through DNA analysis. This revealed a relative abundance of Orientia of 88.7%, 122 sequences relating to the genus, 115 sequences relating to Orientia tsutsugamushi specifically, and an identification confidence of 99%. Therefore, a diagnosis of ST was made. A thorough medical history was then collected, which revealed a recent visit to an orchard. An eschar was then identified (Figure 1a), which had been obscured because it was at the site of insertion of the indwelling needle on the patient’s forearm. Therefore, we were confident of our diagnosis of ST, and a combination of doxycycline (0.1 g q12h for 9 days) and ceftriaxone sodium (2 g qd for 7 days) was administered to treat the infection. Two days later, the patient reported abdominal pain, and physical examination revealed abdominal muscle tension, slight tenderness, and rebound pain in his left lower abdomen. Abdominal enhanced CT showed a mass shadow in the left retroperitoneum, which was consistent with a hematoma (Figure 1b). Based on the CT imaging results and routine laboratory test results indicative of anemia (Hb 53 g/L), we considered that a hematoma had formed in the patient's abdomen; and Agkistrodon acutus hemocoagulase, aminotolic acid, vitamin K1, and etamsylate were used to stop the bleeding. However, the patient’s carbohydrate antigen 125 concentration was high; therefore, we did not rule out the possibility of gastrointestinal cancer. A blood transfusion was performed, and octreotide acetate was administered to alleviate his gastrointestinal symptoms. During the first week of treatment, the patient’s body temperature fluctuated, but ultimately fell below 37.3°C. There were also decreases in his PCT concentration (to 0.04 ng/mL), IL-6 concentration (to 8.16 pg/mL), and WBC count (to 5.11 × 109/L) after a week, and the hematoma had decreased in size. Therefore, the patient was discharged. A telephone consultation was conducted 1 year following his discharge, when he reported no fever, abdominal distension, or abdominal pain; normal bowel movements; and significant improvements in his mental state, appetite, and sleep. In addition, the patient's eschar had subsided, and there were no sequelae to the infection.

Findings in case 1. (a) An eschar on the patient’s forearm and (b) Abdominal enhanced computed tomography image, showing a mass shadow deep to the peritoneum on the left side (red arrow), characterized by uneven density, slightly high-to-low mixed density, and unclear boundary with the left psoas major muscle. It was approximately 110 mm × 87 mm × 109 mm in size, and was consistent with a hematoma.
Case 2
A nearly 80-year-old woman, without any chronic disease, was hospitalized because of diarrhea for 1 week. A previous head CT had revealed lacunar cerebral infarction, and the patient’s symptoms improved after the appropriate treatment was administered. However, she had a fever for approximately 3 days, with a highest temperature of 39°C. She had a CRP concentration of 58 mg/L, a WBC count of 6.69 × 109/L, a neutrophil percentage of 83%, an Hb concentration of 119 g/L, and a platelet (PLT) count of 111 × 109/L. A chest CT showed minor inflammation in her right lung. At another hospital, which the patient had visited before, sulbactam, cefoperazone, and metronidazole was administered to treat an infection. She passed a black stool on one occasion, but an occult blood test (OB test) was negative.
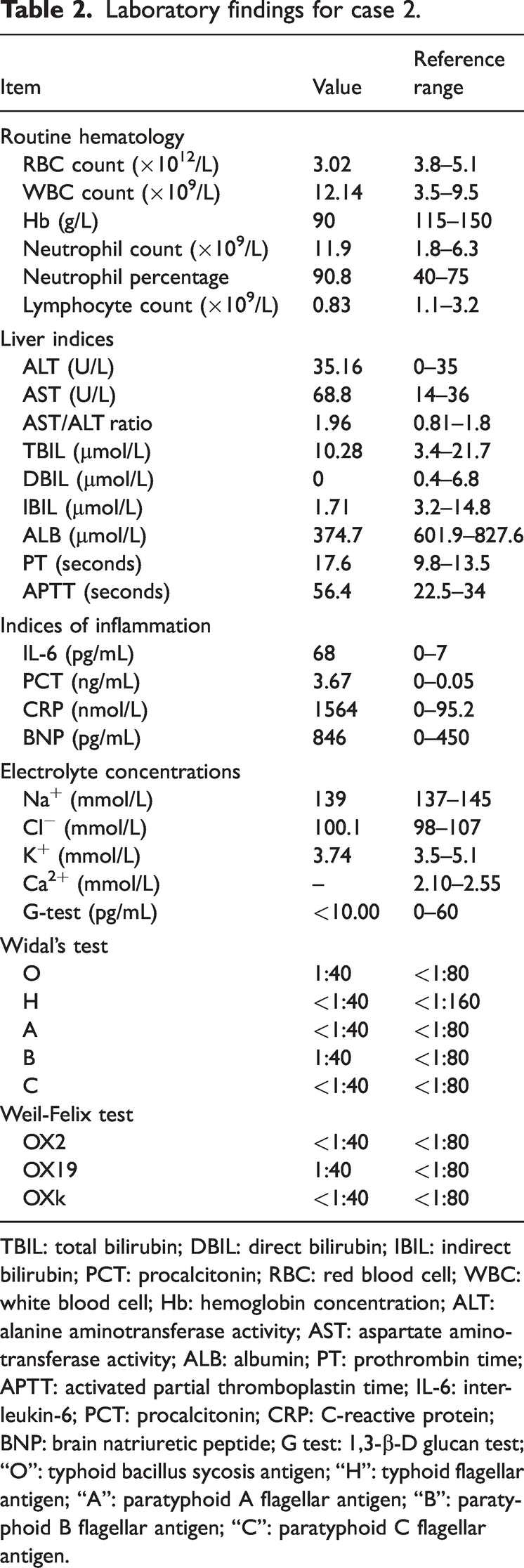
On admission to our hospital, her WBC count was 16.24 × 109/L, her neutrophils percentage was 90.2%, and her Hb concentration was 99 g/L. Her qSOFA score was 1, and physical examination revealed facial edema, slight shortness of breath, coarse breath sounds in both lungs, large blood stasis spots on her right waist and abdomen, and small pustules on her proximal right thigh, with ulceration and minor discharge. Therefore, she was initially diagnosed as having sepsis. After admission, her body temperature was high; she had high values of inflammatory indices (WBC count 12.14 × 109/L, CRP concentration 1.563 μmol/L, PCT concentration 3.67 ng/mL, and IL-6 concentration 68 pg/mL); she had a low RBC count (3.02 × 1012/L) and Hb concentration (90 g/L); and she had hepatic dysfunction (ALT 35.16 U/L, AST 68.8 U/L, and ALB 374.7 μmol/L) (Table 2). Her stool OB test was positive, and therefore the presence of gastrointestinal hemorrhage was considered. Orientia tsutsugamushi was detected on DNA testing of a blood sample for pathogenic microorganisms (the relative abundance of Orientia was 71.91%, 400 sequences were detected relating to the genus, 400 sequences were detected relating to Orientia tsutsugamushi specifically, and the coverage was 0.88%), but Widal’s test, the Weil–Felix test, and a parasite antibody test were all negative. Thoracic and abdominal CT images showed bilateral pneumonia and pleural effusion, pericardial effusion, and a liver cyst. Therefore, the patient was ultimately diagnosed with ST and gastrointestinal bleeding.
Laboratory findings for case 2.
TBIL: total bilirubin; DBIL: direct bilirubin; IBIL: indirect bilirubin; PCT: procalcitonin; RBC: red blood cell; WBC: white blood cell; Hb: hemoglobin concentration; ALT: alanine aminotransferase activity; AST: aspartate aminotransferase activity; ALB: albumin; PT: prothrombin time; APTT: activated partial thromboplastin time; IL-6: interleukin-6; PCT: procalcitonin; CRP: C-reactive protein; BNP: brain natriuretic peptide; G test: 1,3-β-D glucan test; “O”: typhoid bacillus sycosis antigen; “H”: typhoid flagellar antigen; “A”: paratyphoid A flagellar antigen; “B”: paratyphoid B flagellar antigen; “C”: paratyphoid C flagellar antigen.
Initially, cefoperazone (3 g q8h for 2 days) and sulbactam sodium (0.48 g qd for 2 days) were administered empirically to treat an infection, but her temperature continued to fluctuate and remain high. After ST was diagnosed, the antibiotic treatment was changed to meropenem (1 g q8h for 6 days) and doxycycline (1 g q12h for 2 days), and omeprazole and famotidine were administered to inhibit gastric acid secretion. Subsequently, her CRP concentration (to 62.0 nmol/L), PCT concentration (to 0.11 ng/mL), IL-6 concentration (to 20.8 pg/mL), and WBC count (to 7.7 × 109/L) all decreased. After her fever had been relieved, octreotide acetate was administered to relieve her gastrointestinal symptoms, and the anti-infection medication was changed to piperacillin tazobactam sodium (4.5 g q8h for 10 days). The patient had a positive stool OB test, but a negative result for the second sample after continuing treatment, and she was therefore discharged. One year after discharge, a telephone consultation was conducted with the patient; who reported no diarrhea, fever, or melena; that her mental state, appetite, and sleep had returned to normal; and that she had no residual symptoms.
Case 3
A women in her 70s, who had a history of frequent atrial extrasystole, hypertension, hyperlipidemia, hyperuricemia, bilateral upper lung nodules, and degenerative disease of the thoracic spine presented to the hospital. She reported an increase in chest tightness during the preceding 5 days, with each attack lasting more than 30 minutes, and this was accompanied by a mild fever. No skin lesions, such as eschar or ulcer, were found on physical examination, and no other obvious problems were identified. After admission, her qSOFA score was 0. The patient was initially diagnosed with a “fever of unknown origin”, and on further examination (Table 3), there was evidence of liver damage (ALT 110.39U/L, AST 263.42 U/L, and ALB 392.7 μmol/L), mild anemia (Hb 102 g/L), inflammation (CRP 1.259 μmol/L, PCT 0.15 ng/mL, and IL-6 66.9 pg/mL), which indicate that the patient was in the acute stage of infection. In addition, her stool OB test was positive, but her urine culture, blood culture, and G test were negative. However, Orientia tsutsugamushi was detected by DNA analysis (the relative abundance of Orientia was 77.89%, the sequence number was 407, the sequence number of Orientia tsutsugamushi was 407, and the coverage was 0.90%). Chest CT showed bilateral lung inflammation and bilateral pleural effusion; but her abdominal CT was normal. Therefore, the patient was ultimately diagnosed with ST.
Laboratory data for case 3.

TBIL: total bilirubin; DBIL: direct bilirubin; IBIL: indirect bilirubin; PCT: procalcitonin; RBC: red blood cell; WBC: white blood cell; Hb: hemoglobin concentration; ALT: alanine aminotransferase activity; AST: aspartate aminotransferase activity; ALB: albumin; PT: prothrombin time; APTT: activated partial thromboplastin time; IL-6: interleukin-6; PCT: procalcitonin; CRP: C-reactive protein; BNP: brain natriuretic peptide; G test: 1,3-β-D glucan test.
Cefodizime sodium (1 g q8h for 3 days) was administered initially, but the patient continued to have a high fever, and after the administration of piperacillin tazobactam sodium (4.5 g q8h for 3 days), her temperature continued to fluctuate. When the diagnosis of ST was established, doxycycline (1 g qd for 12 days) and meropenem (1 g q8h for 8 days) were administered, and her body temperature returned to normal. Symptomatic treatment relieved the symptoms of hemorrhage. Her Hb concentration returned to normal (108 g/L), her body temperature fell below 37.3°C, and her symptoms were relieved. A year later, during a telephone consultation, the patient reported no fever or chest tightness; and that her mental state, appetite, and sleep had returned to normal. In addition, there were no residual sequelae.
Discussion
With improvements to quality of life and progress in medical treatment, the mortality associated with ST has decreased. Nevertheless, in some underdeveloped areas, owing to limitations in medical technology, ST may not be treated in a timely manner, meaning that the disease may progress further, such as to multiple organ dysfunction syndrome (MODS) 6 . Orientia tsutsugamushi enters cells and propagates, causing local skin lesions, such as eschar and ulcer. After 10 to 40 days, Orientia tsutsugamushi enters the circulation through the lymphatic system, and propagates in vascular endothelial cells and mononuclear macrophages. It produces an exotoxin, which attacks all the organs of the body, causing inflammatory lesions that generate a series of clinical symptoms. ST-induced fever is generally in the form of a remittent fever, which is accompanied by symptoms of systemic poisoning. On physical examination, erythema of the face, neck, and chest is common, accompanied by conjunctival congestion, eschar or ulcer, lymphadenomegaly, rash, and hepatosplenomegaly. As the disease progresses, multiple organs can become dysfunctional, including the nervous system, circulatory system, and respiratory system. Appropriate treatment with antibiotics causes the patient’s body temperature to return to normal and ameliorates the condition. However, if the disease progresses to MODS because of a lack of a timely diagnosis and treatment, the mortality rate can be as high as 70%. 7 The most characteristic physical symptoms of ST are eschar and ulcer, which can appear in any part of the body, but mostly in areas that perspire significantly. Most patients have a single eschar, which is round or oval, dark in color, with a diameter of 4 to 10 mm and slightly raised margins. It typically appears like a dike, and is surrounded by an erythematous ring, but there is no pain or effusion. After the eschar is shed, the central depression forms an ulcer. 8
None of the three patients described herein mentioned having been bitten by arthropods, but one recalled visiting an orchard, and his eschar only appeared after the identification of Orientia tsutsugamushi. However, no eschar was identified in the other two patients on physical examination. It is worth noting that all three patients had anemia and hemorrhage. The male patient had an abdominal hematoma, and the two female patients had gastrointestinal hemorrhage, indicated by a positive stool OB test. All of the three had a continuous fever (Figure 2), signs of liver damage, and pulmonary inflammatory lesions, suggesting that organ damage is a feature of acute ST infection. Fortunately, the three patients were diagnosed using DNA analysis during the early stages of their disease. After combined treatment with antibiotics suitable for the treatment of ST infection, such as doxycycline, the symptoms of hemorrhage were controlled, the body temperatures of the patients returned to below 37.3°C, and the values of inflammatory indices, such as WBC count, CRP, and PCT, decreased. We believe that the timing of the diagnosis of ST determines the prognosis of the patients.

Body temperatures of the three patients during their hospitalization.
The case of a 28-year-old with ST complicated by cerebral hemorrhage was reported in 2020. 9 He was hospitalized for 2 weeks, owing to fever, headache, sensory abnormalities, and diarrhea. After admission, his condition quickly progressed to multiple organ disease, including disseminated intravascular coagulation, acute respiratory distress syndrome, and acute kidney injury. Serological testing revealed positivity for anti-ST IgM antibody. Unfortunately, despite the administration of doxycycline, because of the late detection of the pathogen, the patient’s poor general condition, and other factors, the patient developed MODS and eventually died because of renal failure and severe respiratory acidosis. Therefore, it is crucial to diagnose ST during the early stage of the disease and to administer appropriate antibiotics in a timely manner to improve the prognosis of ST. Early research showed that high values of endothelial and macrophage markers are related to the severity of and mortality associated with ST, 10 and that the examination of the abdominal and pelvic lymph nodes by abdominal CT may be helpful for the early diagnosis of the disease. The enlargement of the perigastric lymph nodes may also be a sign of severe ST with liver dysfunction.10–12 The finding of IgM antibodies to Orientia tsutsugamushi has some diagnostic significance. 13 However, these findings are not a basis for the diagnosis of ST. Rather, the identification of pathogen DNA is more specific. Kim et al. found that the genotype and DNA load in the patient's circulation are useful markers of the severity of ST. 14 For the present three patients, blood or body fluid samples were collected for analysis of the microbial DNA. As a result, their disease was diagnosed in a timely manner and appropriate drugs were administered. A review of multiple clinical studies showed that doxycycline is effective for the treatment of ST, 15 and its therapeutic effect was confirmed in the three patients reported herein. After a diagnosis of ST is made, the values of inflammatory indices, body temperature, and other indices can be used to predict the prognosis. In addition, the serum tumor necrosis factor-α concentration is predictive of the prognosis of patients, with increases in concentration indicating that the prognosis is poor. 16
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231204430 - Supplemental material for Three cases of scrub typhus with hemorrhage: a case report and literature review
Supplemental material, sj-pdf-1-imr-10.1177_03000605231204430 for Three cases of scrub typhus with hemorrhage: a case report and literature review by Ziren Chen and Shi OuYang in Journal of International Medical Research
Footnotes
Acknowledgements
The authors would like to thank the patients for agreeing to the use of their medical data for scientific research, Hiro Zhang for polishing and proofreading the article, and the staff of The Fifth Affiliated Hospital of Guangzhou Medical University for their support.
Author contributions
ZC was responsible for the study conception, data acquisition, and the writing of the case report. SO was responsible for the writing and revision of the case report, approved the submitted version, and agrees to be personally responsible for its contribution and any problems related to the accuracy or completeness of any part of the work.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
The study was approved by the Ethics Committee of The Fifth Affiliated Hospital of Guangzhou Medical University (approval number GYWY-L2023-127). Written informed consent was obtained from all the participants for their treatment and the publication of the manuscript.
Funding
This study was supported by the Key Laboratory of Guangdong Higher Education Institutes (2021KSYS009), the Key Medical Disciplines of Guangzhou (2021-2023) Project, the Plan for Enhancing Scientific Research of Guangzhou Medical University, Guangdong Province Department of Education (2021ZDZX2063), and the Guangzhou University Foundation (202102010100).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.