
Abstract
Objectives:
This study aimed to understand the field epidemiology, clinical findings, diagnostic reports and outcome of Scrub typhus patients admitted at Gedu District Hospital, Bhutan.
Methods:
The researcher extracted data from the records of patients admitted at the hospital from 1 January 2017 to 31 December 2020, with diagnosis of Scrub typhus. A total of 185 records were used to study the demographic distribution, results of rapid diagnostic test for Scrub typhus, presence of eschar, treatment outcome and duration of admission in the hospital.
Results:
The months of May to October had increased admissions of 137 (74%) patients with a peak in September. Three gewogs (sub-districts) had 173 (93.5%) patients; age range was 6 months to 84 years and a greater proportion of patients were females.
Conclusion:
Scrub typhus is endemic in the district. The absence of recorded fever or a negative rapid diagnostic test report may not exclude the diagnosis of Scrub typhus.
Keywords
Introduction
Scrub typhus is an acute febrile bacterial disease and a public health problem with an estimated 1 million new infections each year in the Asia-Pacific region alone. 1 It is a leading cause of treatable non-malarial febrile illness in Asia and has a seroprevalence ranging from 9.3% to 27.9% with a median of 22.2% with a median mortality of 6.0% for untreated and 1.4% for treated Scrub typhus patients. 2
The cause of Scrub typhus is a bacterium called Orientia tsutsugamushi which survives on the reservoir called chigger mite and these mites in turn live in the Rattus genre of the rodent family. 3 The bacterium is transmitted to humans accidentally as zoonosis by bite of infected chigger mites. The patients are more likely to live close to bushes and wood piles, and work on farms, have seen rodents at home or at work, reared domestic animals and are less likely to wash after work or change clothes to sleep.4,5
Scrub typhus has an incubation period of 10–14 days and the disease manifests with acute onset of non-specific fever, headache, malaise, swollen lymph nodes and maculopapular rashes by the end of the first week of fever. Diagnosis is often missed in absence of epidemiological and clinical knowledge leading to delay in initiating treatment and this may lead to preventable deaths. 6 Therefore, the diagnosis thus relies mainly on disease epidemiology, clinical competence, identification of eschar and further supplementation by laboratory tests. 7 Eschar is a tiny burn like lesion with a peripheral redness, which occurs at the site of bite by chigger mite which gives clinical clues for diagnosis of Scrub typhus. 8 The common tests available are serological tests for detection of specific human Immunoglobulin M (IgM) antibodies against O. tsutsugamushi in serum of acute febrile patients by enzyme-linked immunosorbent assay or by indirect immunofluorescence assay. 9 The medicine used for treatment of Scrub typhus are doxycycline or azithromycin or chloramphenicol. 10
In Bhutan, this disease had remained as an unrecognized, under-diagnosed and under-reported disease with often fatal consequences till it was reported in 2009. 11 Further, a case study showed that there was a delay in recognition of an outbreak of Scrub typhus in a remote primary school during August to October 2014 leading to two deaths due to complication of the disease. 12 A total of 3104 patients were admitted at Gedu Hospital from 1 January 2017 to 31 December 31 2020 and out of them 185 (6%) patients had a diagnosis of Scrub typhus.
This study was conducted to contribute evidence on field epidemiology, demographic profile, clinical characteristics and treatment outcome. The findings are expected to aid health workers for management of fever patients in limited clinical and diagnostic service facilities which are seen in most of the health centres in Bhutan.
Methods
The study is a retrospective descriptive analysis of records of patients who were diagnosed with Scrub typhus, admitted and treated at Gedu Hospital from 1 January 2017 to 31 December 2020. The study found 185 such records. The sources of data were the patient admission register and patient history sheets which were maintained at the medical record section of Gedu Hospital. All the records which showed diagnosis of Scrub typhus were used in the study and a separate inclusion or exclusion criteria were not followed.
The Gedu Hospital is located at a distance of about 119 km from the capital city of Thimphu and falls under Bongo Gewog (sub-district), Chhukha District, Bhutan. It is a 20-bedded district hospital which is managed by doctors with an MBBS qualification. It provides health services to about 38,000 people and to referred patients from other nine Primary Health Centres who are scattered over nine gewogs.
The patients are diagnosed by doctors. The laboratory tests that are conducted in the hospital are routine blood and urine tests, liver and kidney function tests and rapid diagnostic tests (RDTs) for Scrub typhus, typhoid, dengue and malaria. For diagnosis of Scrub typhus, Bioline tsutsugamushi RDT kits are used for detection of IgM. The diagnosis is also made based on other supportive blood and urine test reports when RDT kit is not available or the result is negative despite clinical suspicion. The blood test parameters used are elevated total white blood cells count to more than 11,000/mm3, decreased blood platelet count of less than 100,000/mm3 and elevated levels of liver enzymes or presence of protein in urine analysis. 13 Laboratory tests are conducted to exclude other febrile illnesses such as typhoid, dengue and malaria.
The patients’ temperature is measured by nurses with clinical thermometer. Blood pressure and pulse are measured by digital blood pressure apparatus during admission to the ward. The same vital signs are measured at 6 am and 6 pm daily and more frequently if advised by doctors. The doctors perform routine monitoring of the patients’ clinical status during daily rounds. The medicine administered to the adult patients is 100 mg of oral doxycycline capsules two times in a day for 5 days. Pregnant patients are administered 500 mg of azithromycin once daily for 5 days. Children are administered doxycycline syrup calculated as 4.5 mg/kg of body weight and divided into two equal doses at 12 h apart. The patients who are not able to take oral medicines are administered intravenous injection of chloramphenicol four times in 24 h.
The criteria for recovery and discharge are decided as subjective patient well-being, blood pressure in normal range, absence of fever for more than 24 h and improvement in blood platelets and liver enzymes as compared to level during diagnosis. Patients are also referred to the National Referral Hospital in Thimphu when doctors are not able to manage them at Gedu Hospital.
Procedure
Ethical clearance was obtained from the Research Ethics Board of Health (REBH) vide letter number REBH/Approval/2020/043 dated 15 September 2020 before commencing the study. The investigators did not contact patients for any additional or individually identifiable information. Waiver of informed consent was obtained during approval and the records were kept secured by the principal investigator.
Statistical analysis
Double Data entry was done in EpiData 3.1 version (EpiData Association, Odense, Denmark). These double files were validated and analysed by EpiData Analysis 2.2.2.182 version (EpiData Association, Odense, Denmark). The monthly trend of patients admitted over 4 years was represented by line graphs. The gewog-wise yearly distribution of patients was represented in tables and expressed as numbers and proportions. The variables measured were month of admission, age, sex, address of patient, method of diagnosis, temperature of the patient during admission, RDT reports, presence of eschar, medicines used, outcome of treatment and duration of admission. They were represented in frequencies and proportions. The presence of fever, findings of diagnostic tests and presence of eschar in males and females was represented in tables and expressed as numbers and proportions. The age breakdown was done as per the monthly morbidity report form of the Bhutan Health Management Information System. 14
Results
In the present study, Scrub typhus cases were found to occur throughout the year but months of May to October showed 137 (74%) admissions with a peak in September (Figure 1).

Monthly trend of admission of Scrub typhus patients at Gedu Hospital, Bhutan, 1 January 2017 to 31 December 2020, n = 185.
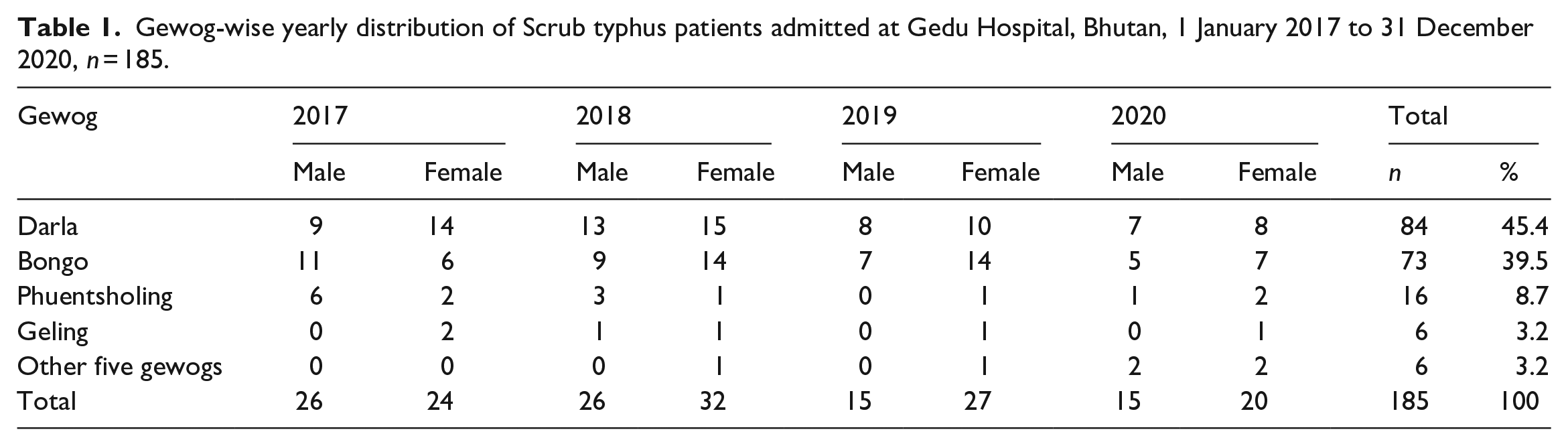
There were patients from all the gewogs but 173 (93.5%) patients were from Bongo, Darla and Phuentsholing gewogs (Table 1).
Gewog-wise yearly distribution of Scrub typhus patients admitted at Gedu Hospital, Bhutan, 1 January 2017 to 31 December 2020, n = 185.
The age range of patients was 6 months to 84 years with 44 (28.8%) patients below 14 years of age and 113 (61.1%) patients within the age group of 20–59 years (Table 2).
Age range of Scrub typhus patients admitted at Gedu Hospital, Bhutan, 1 January 2017 to 31 December 2020, n = 185.

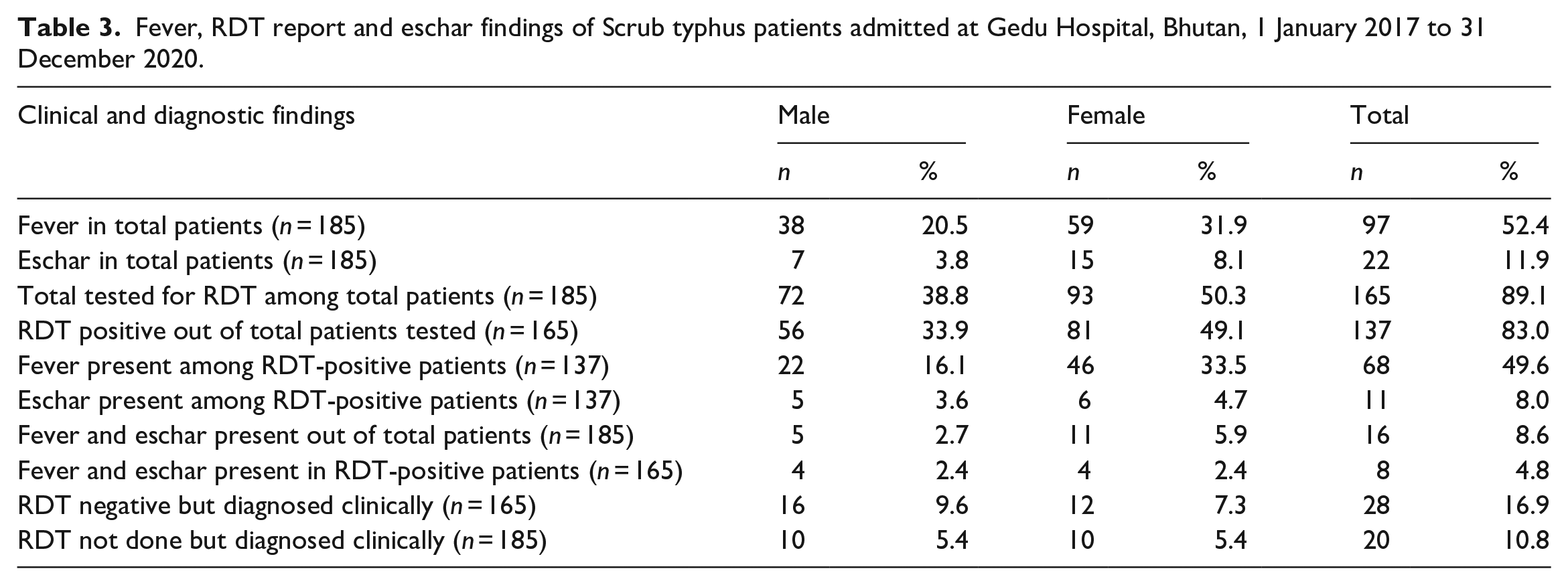
Ninety-seven (52.5%) patients had fever. The RDT report was positive for Scrub typhus in 137 (83%) out of the 165 patients tested. Eschar was present in 11 (8%) of the RDT-positive patients. Eight (4.8%) of the RDT-positive patients had both fever and eschar. Twenty (10.8%) patients were not tested with RDT but diagnosed clinically (Table 3).
Fever, RDT report and eschar findings of Scrub typhus patients admitted at Gedu Hospital, Bhutan, 1 January 2017 to 31 December 2020.
The temperature ranged from 99.5° to 104° Fahrenheit with a mean of 101.4° Fahrenheit.
One hundred and sixty-four (88.6%) patients were treated with oral doxycycline, 19 (10.3%) were treated with oral azithromycin and 2 (1.1%) were treated with chloramphenicol injection. Out of the 185 admitted patients, 2 (1.1%) of them were referred to National Referral Hospital, Thimphu while 183 (98.9%) of them were discharged from Gedu Hospital after recovery. There were no deaths. The duration of admission ranged from 1 to 10 days with a mean of 4 days and a median of 3 with standard deviation of 1.77.
Discussion
The study found that there was a temporal pattern in the admission of Scrub typhus patients and 74% of patients admitted between May and October with a peak in September every year. These months of the year coincided with the monsoon and farming season which could have favoured the density of the chiggers due to abundance of bushes and farming activities.
The spatial distribution showing 177 (93.5%) patients from Bongo, Darla and Phuentsholing gewogs alone could be due to abundance of scrub vegetation and cardamom fields. Zangpo et al. 15 in their study have reported that cardamom-related works were associated with Scrub typhus. Further, the history mentioned in the medical record sheets of patients had reports of them having worked in a cardamom field 10–14 days before the onset of symptoms. This disease pattern may be possible in other parts of the country which share similar vegetation because a study had reported Scrub typhus from the Tsirang district which has a similar agricultural pattern like the Gedu area. 16
The patients in the age group of 20–59 years form an active workforce for outdoor and agricultural works. The infection in patients who were below 14 years of age could be due to staying outdoors and moving into bushes because such activities were found as risk factors for acquiring Scrub typhus as per a study conducted in Uttar Pradesh in India. 17
Regarding clinical features, we analysed only fever and eschar in our study because only those records were consistent in the entire medical document. The presence of fever only in 52.4% could be due to the intermittent nature of fever. Another clinical clue to diagnosis was the presence of eschar, a painless sore that the patient may not notice unless searched keenly for its presence. Eschars are located mostly over the covered areas such as the groin, genitalia, inframammary area and axilla. 7 The absence of eschar did not exclude the diagnosis of Scrub typhus because only 8% of the RDT-positive patients had eschar. The RDT kit which was used for the diagnosis had a sensitivity of 95.2% as per the manufacturer’s details but in our study 137 (83%) patients tested positive for Scrub typhus. The negative result in 28 (17%) patients indicated that antibodies to the bacterium were either absent or present in lower levels for the RDT kit to detect in patients who presented during early stages of infection despite having clinical features of Scrub typhus. 18 The reference standard test for diagnosis of Scrub typhus called polymerase chain reaction was not available at Gedu Hospital. The treatment was effective except in 2 (1.1%) patients which shows that the majority of the patients can still be treated as per the guideline of the Ministry of Health, Bhutan on the management of Scrub typhus. 19 In the present study we could not conduct drug sensitivity tests as the facility was neither available in the hospital nor it was in the scope of the study.
Limitations and bias
Sample size calculation was not done and all the records which showed diagnosis of Scrub typhus were used in the study. Inclusion and exclusion criteria were not followed because all the records which mentioned the diagnosis of Scrub typhus were used in the study. The study could not explain the reason for greater proportion of female patients or more female patients with eschar. A prospective study may be conducted to understand this finding. A possible bias could have occurred in diagnosis during shortage of RDT kits in the hospital. Being a retrospective study, some of the information such as occupation, other blood test report details and other set of examination findings were not consistent and could not be analysed in the study.
Strength
We adhered to Strengthening and Reporting of Observational Studies in Epidemiology (STROBE) guidelines in conducting and reporting the study. 20 It provided evidence to health workers on field epidemiology, diagnostic and management approach to patients presenting with acute febrile illness. This evidence is important in a facility where tropical medicine specialists or definitive diagnostic services are limited or absent. The study also shows the way forward for public health intervention in the gewogs.
Conclusion
Scrub typhus is an endemic disease in the district infecting both children and adult populations. A greater proportion of patients are female. The number of patients increased from May till October with a peak in September. The absence of recorded fever during examination may not exclude the diagnosis of Scrub typhus. Eschar may be found when looked for in patients irrespective of RDT reports.
What we already know
Scrub typhus disease is diagnosed mostly in adult males who work in fields and bushes.
Diagnosis of Scrub typhus from other acute febrile illness is difficult due to non-specificity of the clinical findings.
What this article adds
Scrub typhus is diagnosed in both children and adults and a larger proportion of patients were female.
Epidemiological and clinical competency with detailed history and patient examination for eschar and not relying completely on negative diagnostic test report could aid to early diagnosis of Scrub typhus.
Footnotes
Acknowledgements
We acknowledge the contributions made by Mr Karma Dorji and Mrs Karma Choden, staff nurses of Gedu Hospital, Chhukha, Bhutan for retrieving the patients’ case sheets and collecting the data for the study.
Authors contribution
TN designed the research protocol, coordinated the research and drafted the article. GC helped in data collection, analysed the data and worked to finalise the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from *Research Ethics Board of Health (REBH), Bhutan as per approval number REBH/Approval/2020/043 dated 15 September 2020 before commencing the study.
Informed consent
Informed consent was not sought for the present study because this study was a retrospective analysis of the hospital data and patients were not contacted during this study. No identifiable data were mentioned in the study. Waiver of consent was also sought approval from the REBH.