
Abstract
The hump-nosed pit viper (HNPV) has historically been considered less medically significant, causing local envenomation, renal injury, and coagulopathy; however, now, it is known to cause life-threatening complications. We describe the clinical presentation, treatment, and complications of 3 confirmed HNPV bites from the state of Karnataka (southwest coastal India). Patient 1, an 88-y-old woman, reported with the live specimen and developed venom-induced consumption coagulopathy (VICC) and thrombotic microangiopathy leading to acute kidney injury requiring blood product transfusions and dialysis. Patient 2, a 60-y-old woman, reported 3 d after envenomation followed by treatment at another hospital where 30 vials of polyvalent anti-snake venom (ASV) were given. She developed VICC and acute kidney injury requiring dialysis. On Day 9 of treatment, she developed a pontine hemorrhage. She died after a transfer to another treatment center closer to her residence. Patient 3, a 25-y-old man, was brought to our emergency department 6 h after being envenomed. He received topical ayurvedic treatment before arrival. He was unconscious and found to have severe VICC with a massive middle cerebral artery infarct. All 3 patients received Indian polyvalent ASV, which does not cover HNPV envenomation, clearly demonstrating the absence of paraspecificity and neutralization in a clinical setting. To our knowledge, Hypnale hypnale envenomation has not previously been reported from Karnataka state. The diagnosis of HNPV envenomation in a country without snake venom detection kits, under-reporting despite serious complications, financial burdens on rural populations afflicted, and poor outcomes due to the lack of a specific antivenom are discussed.
Introduction
The hump-nosed pit viper (HNPV) is a venomous snake inhabiting Sri Lanka and the Western Ghats of India. Three species are known, Hypnale hypnale, Hypnale zara, and Hypnale nepa, of which only H hypnale is found in India. 1 Earlier believed to cause only local envenomation, it is now known to cause severe systemic toxicity and mortality. 2 -4 HNPV envenomation is under-reported in India. Identification of the culprit species often does not occur, and physicians are commonly uninformed about the biodiversity of regional herpetofauna, thereby adding to the paucity of data. Limited awareness about the specificity and clinical effectiveness of locally available antivenoms may subject the envenomed patient to ineffective treatment and unnecessary risk. We report the cases of 3 patients with H hypnale envenoming who presented to our emergency department and the associated concerns about treating patients affected by envenoming by this species in India.
Case Report
All 3 cases were managed in the emergency department and emergency intensive care unit by the authors and therefore identified for this report; evidence for identification was either the dead or live specimen or a photograph of the snake being produced by the family members. The specimens were identified on the basis of their morphology by an emergency physician (one of the authors, FMS) with expertise on venomous snakes in the region. The medical record file numbers were identified through the emergency department registers. An application for permissions to study the files and the electronic medical records of the patients was submitted to the institutional ethics committee. After approval, the files and electronic medical records were reviewed and data collected on a case proforma. Radiographic images and laboratory data were extracted. Informed consent was obtained from each patient/family to collect images at the time of presentation and further for the use of the images. Polyvalent anti-snake venom (ASV) used in these patients was produced by Bharat Serums Pvt Ltd. When reconstituted, each vial contains 10 mL; the manufacturer provides the following venom neutralization: 0.6 mg of Naja naja venom/mL of ASV, 0.45 mg of Bungarus caeruleus venom/mL of ASV, 0.6 mg of Daboia russelli venom/mL of ASV, and 0.45 mg of Echis carinatus venom/mL of ASV. This polyvalent ASV is not manufactured to neutralize the venom of H hypnale and is completely ineffective against it.
Case 1
An 88-y-old woman with no known comorbidities was bitten on her right hand while she was working in the garden. A glycerin magnesium sulfate dressing was applied to the bitten limb (Figure 1A). The snake was captured and brought to the hospital and was identified as an HNPV (Figure 1B). She was administered 38 vials of ASV in 4 separate infusions over the course of her treatment despite knowing that no ASV manufactured anywhere in the world specifically neutralizes HNPV venom. She developed hypotension during the first infusion, which was treated with antihistamines and adrenaline for anaphylactic shock. The second and third doses administered on Day 1 were given at 125 mL·h‒1, whereas the last dose of 8 vials was given at 40 mL·h‒1. She was found to have thrombocytopenia and anemia. A peripheral smear showed schistocytes, while coagulation and renal parameters, which were normal on Day 1, showed a progressive decline from the second day. She remained anuric until discharge. She underwent 3 cycles of saline hemodialysis: 1.5 h on Day 1, 3 h on Day 3, and 4 h on Day 4. Owing to the persistent coagulopathy, she received 1 packed red blood cell and 10 fresh frozen plasma transfusions (Table 1, Case 1). She was discharged against medical advice, with persistent acute kidney injury and coagulopathy. On telephonic follow-up, no clinical symptoms of renal dysfunction or bleeding diathesis were reported.

A, Bitten index finger of the right hand. B, Live culprit snake. Specimen location: Karkala (13.2151°N, 74.9962°E). Approximate distance from the hospital: 33.8 km.
Coagulation parameters, renal function, and treatment administered based on the findings of cases 1, 2, and 3
PT, prothrombin time; INR, international normalized ratio; aPTT, activated partial thromboplastin time; n/a, not available/not done; ASV, anti-snake venom; FFP, fresh frozen plasma; HD, saline hemodialysis; PRBC, packed red blood cell; CRYO, cryoprecipitate.
Case 2
A 60-y-old woman, a known hypertensive on 5-mg amlodipine once daily with no other comorbidities, was bitten by an HNPV (Figure 2A) while working in her garden, after which she developed signs of envenomation. She was taken to a local hospital on Day 2, where she was administered 30 vials of ASV. She developed anuria and vomiting because of which she was referred to our center on Day 3; she was found to have mild coagulopathy, thrombocytopenia, and deranged renal parameters for which hemodialysis was initiated with fresh frozen plasma transfusions (Table 1, Case 2). She was administered an additional 4 vials of ASV. On Day 9, she developed sudden-onset altered mental status after undergoing dialysis; a plain computed tomography scan of her brain showed a large pontine bleed (Figure 2B). The patient was discharged against medical advice on mechanical ventilation and was hemodynamically unstable. The family’s decision was due to an evidently poor outcome and increasing costs of care. On follow-up, she had passed away at a local hospital with minimal critical care.
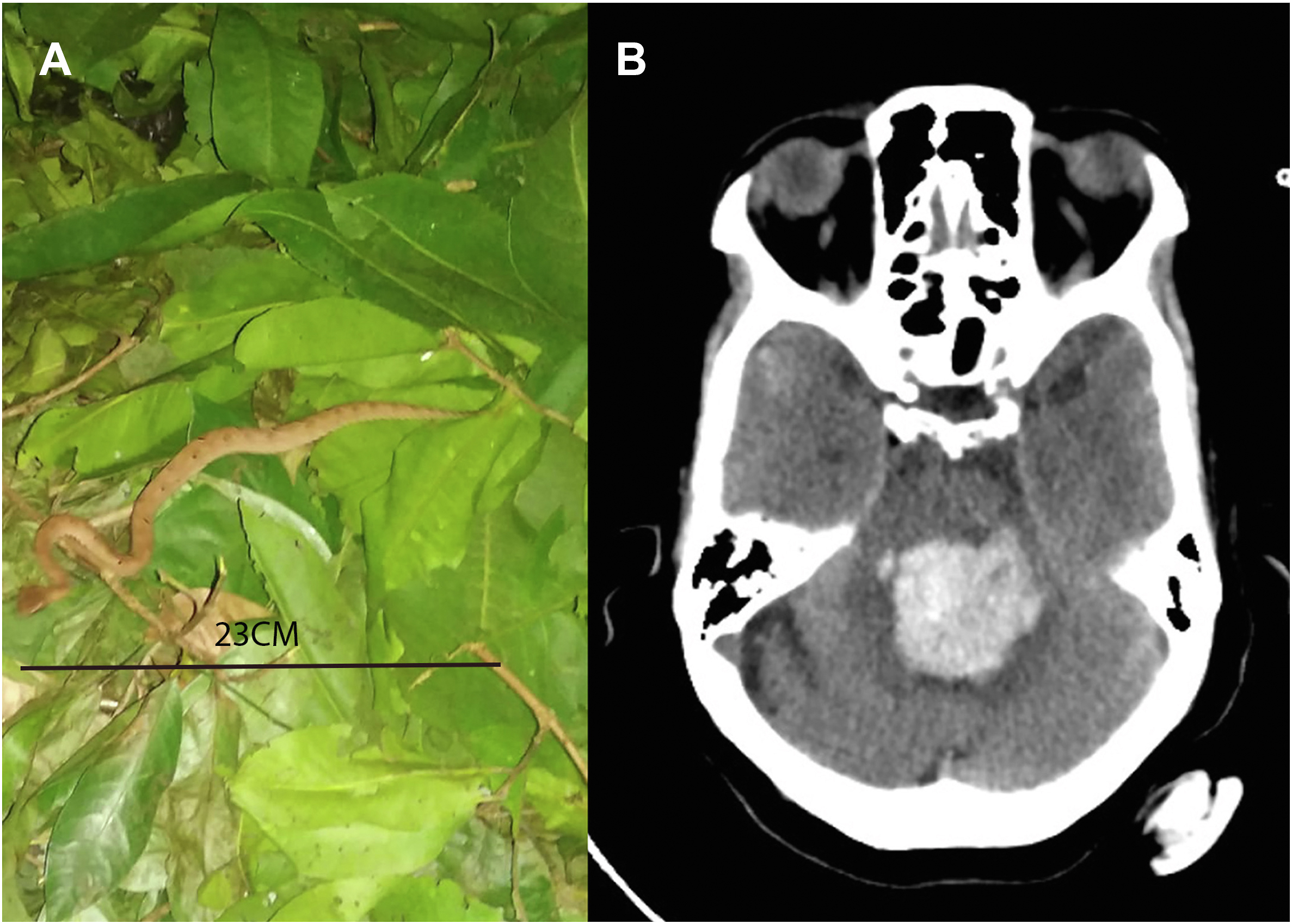
A, Photographic evidence of the culprit snake. Specimen location: Kundapura (13.6235°N, 74.6917°E). Approximate distance from the hospital: 61.2 km. B, Computed tomography scan of the brain showing pontine bleed.
Case 3
A 25-y-old man with no known comorbidities or atopy was brought to the emergency department with an alleged history of snakebite 6 h before admission; after the bite, he had an episode of loss of consciousness and altered mental status. The patient received ayurvedic treatment (Figure 3A) and later was evaluated at a local hospital before being referred to our hospital for further treatment. In the emergency department, he was intubated owing to a low Glasgow Coma Scale score (E1V1M5) and was found to have severe coagulopathy with a prothrombin time of >120 s. Treatment with polyvalent ASV was immediately started; however, anaphylaxis developed in him, for which antihistamines and adrenaline were administered. Treatment with ASV was restarted once he stabilized. On further evaluation, he was found to have right-sided hemiparesis. A plain computed tomography scan of the brain was obtained, which revealed a massive left middle cerebral artery territory infarct with cerebral edema (Figure 3B). A neurosurgical opinion was taken to consider decompressive craniotomy. In spite of 30 vials of ASV transfused, there was no improvement. Initially suspected to be a Russell viper bite on the basis of the syndrome, it was later identified as an HNPV envenomation on the basis of the lack of response to ASV and the identification of the specimen, which was later found and produced (Figure 3C). The family members were requested to locate and bring the killed specimen, which had been discarded at the location where the bite occurred. Therefore, further doses of ASV were withheld. Measures to control the brain edema (mannitol, blood pressure control, and head end elevation) were initiated, and antiplatelet therapy was withheld because of the coagulopathy. A decompressive craniotomy was considered, in view of the raised intracranial pressure and significant midline shift; however, it would be considered only after correction of the coagulopathy. Owing to the unresolved venom-induced consumption coagulopathy (VICC), which showed no response to 30 vials of ASV, cryoprecipitate and fresh frozen plasma were administered, after which the international normalized ratio improved to 2.24 (Table 1, Case 3). However, the family members were not willing to consent to a craniotomy in view of a poor prognosis and high risk of death and requested that the patient be discharged against medical advice. The family members took the patient home. No further in-hospital care was provided.
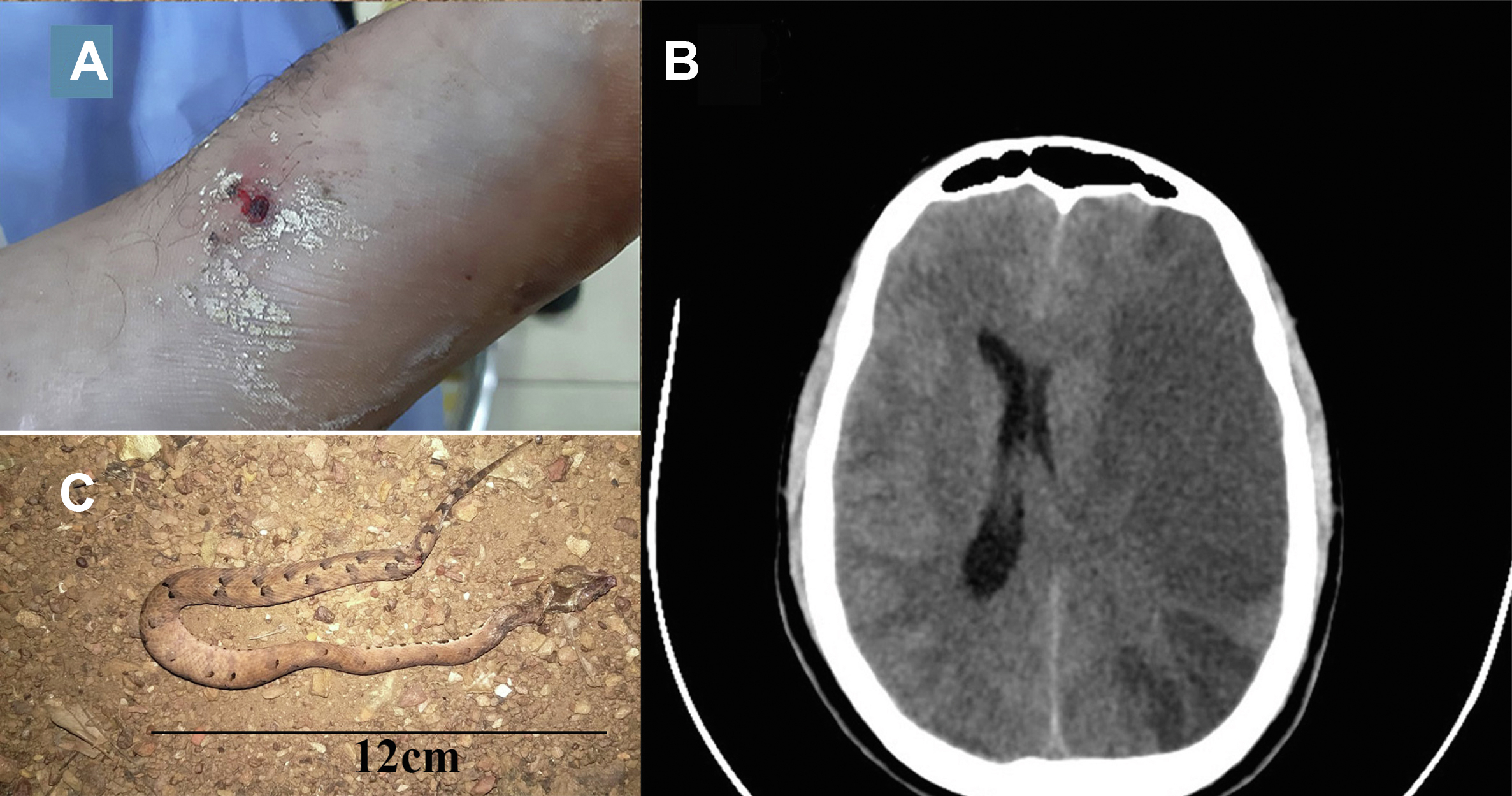
A, Bite site showing fang marks with oozing blood. B, Computed tomography scan of the brain showing large middle cerebral artery territory infarct with midline shift. C, Photographic evidence: snake killed and photographed. Specimen location: Bhatkal (13.9993°N, 74.5408°E). Approximate distance from the hospital: 93 km
Discussion
In the Western Ghats, there is no antivenom available for several species of medically important venomous snakes, including the HNPV (H hypnale), Malabar pit viper (Craspedocephalus malabaricus), bamboo pit viper (Craspedocephalus gramineus), large-scaled pit viper (Craspedocephalus macrolepis), and king cobra (Ophiophagus hannah).5,6 In a proteomic study, the investigators reported that monovalent Calloselasma rhodostoma (Malayan pit viper) ASV from Thai Red cross partially neutralized HNPV venom in vitro. They also reported that HNPV venom is geographically variable, emphasizing the need for venom analysis of H hypnale occurring in southwest coastal India.7,8
Syndromic similarities of juvenile Russell viper, saw-scaled viper, and HNPV envenomation pose a challenge. 9 The absence of a regionally specific molecular diagnostic kit to differentiate envenomations from a region is a burden of great significance. 10 Delayed onset of coagulopathy, as seen in Patients 1 and 2, is common and may not be detected by a 20-min whole blood clotting test. 11 Public awareness about capturing photographic evidence to aid physicians in the treatment of snakebites is variable. In some communities, an offending snake is burned and buried. In Case 1, the live snake was produced at the hospital—apart from identification, the snake had to be held captive and later released. The family members of the patient in Case 2 produced a low-quality image of the culprit snake but with just enough detail for a morphological identification. In Case 3, the culprit snake was killed but no photographs were taken and the snake was not brought to the hospital; the family members had to travel 93 km one way to retrieve the decaying and damaged specimen for identification, by which time standard therapeutic measures were complete.
HNPV envenomation shows some clinical features that are common to D russelli, E carinatus, and C malabaricus. 9 Common to all 4 are VICC and cellulitis or edema of the bitten part. Acute kidney injury is common in Russell viper and HNPV envenomation and rare in saw-scaled viper bites. The time of onset and progression of coagulopathy and acute kidney injury is variable, which can be hours, as seen in Case 3, and days, as in Case 1. 11 Thrombotic microangiopathy, seen in Patients 1 and 2, is a known complication of HNPV envenomation. 12 Patient 1 developed severe renal dysfunction but eventually improved and was free of symptoms after discharge. Patient 2 developed renal injury requiring hemodialysis and, on Day 9, developed a pontine hemorrhage. VICC may increase the incidence of hemorrhagic stroke in patients, especially those with risk factors, such as hypertension, which was present in this case. Patient 3, a young man with no comorbidities, developed a massive ischemic stroke within hours of being bitten. As the evidence of the culprit snake was initially unavailable, 30 vials of ASV were administered but clearly did not lead to improvement in coagulopathy, demonstrating ineffective neutralization of the circulating venom. The venom of HNPV contains phospholipases, C-type lectins, and L-amino acid oxidases, which are anticoagulants; however, it also contains thrombin-like enzymes that can cause thrombotic effects such as ischemic stroke.13,14
Local, vascular, hematological, cardiac, direct neurotoxicity, ischemic stroke, pulmonary, and renal manifestations have been described with regard to HNPV bites.3,12,14-18 However, the frequency of systemic manifestations from India is more than that from Sri Lanka. 19 Coagulopathy was common with H hypnale compared with H zara and H nepa. 17 Only H hypnale is found in India, which may explain the higher incidence of systemic toxicity. Other known complications associated with H hypnale bites include ischemic and hemorrhagic stroke, acute coronary syndrome and toxic myocarditis, atrial fibrillation, and seizures.14,20-22
None of the 3 patients responded to Indian polyvalent ASV. ASV is often administered because of a delay in the identification of the species (as in Case 3). It is clear in all the 3 cases that administration of Indian polyvalent ASV may actually do more harm than good in HNPV envenomation. 23 Coagulopathy may be corrected with blood products in the presence of life-threatening bleeding manifestations, although the addition of clotting factors may result in an increase of systemic clot burden without prior neutralization of the venom. 24 Severe life-threatening VICC detected early may be treated with therapeutic plasma exchange and replacement of coagulation factors because of the absence of any antivenom. It is associated with a high risk of complications along with limited clinical benefit.25,26
In general, Hypnale envenomation is not widely known, resulting in under-reporting and delayed hospitalization. There is a preference for alternative medicine, as seen in Case 3. The economic burden on rural populations is high, which is highlighted in these cases, in which premature discharge was taken in Cases 1 and 3. Patients 2 and 3 required prolonged critical care with poor outcomes. Healthcare schemes for farmers and populations at risk can be customized to include therapeutics such as hemodialysis, therapeutic plasma exchange, and surgical interventions in some complex cases of snakebite so that discharges against medical advice and resultant tragic outcomes are avoided.
Conclusions
There is a need for H hypnale antivenom. In the interim, treatment including transfusion of blood products and plasmapheresis may be considered in severe cases only. The delayed onset of systemic manifestations warrants observation and frequent evaluation over 48 to 72 h. Involvement of the primary care system in the monitoring of such patients with 20-min whole blood clotting test or prothrombin time with international normalized ratio tests and renal function tests should be considered, particularly in rural and remote regions to identify cases with delayed systemic envenomation. Identification of the culprit snake must not be missed wherever possible. HNPV envenomation may result in complications such as VICCs, strokes, and thrombotic microangiopathy with acute kidney injury.
Footnotes
Acknowledgements
Acknowledgments: The authors thank Nirmal Kulkarni, Gerry Martin, Rom Whitaker, and Ramesh Zarmekar for sharing their knowledge and field experience on hump-nosed pit viper and the Departments of Emergency Medicine, General Medicine, and Nephrology at Kasturba Medical College, Manipal, for their support.
Author Contributions: original draft of manuscript, imaging of snakes and bite site, identification of snakes, institutional ethics committee approval (FMS); draft of manuscript, review, and editing (VL); critical review of manuscript (JMB); approval of final manuscript (FMS, VL, JMB).
Financial/Material Support: None.
Disclosures: None.