
Abstract
Snakebite in India is often attributed to the “big 4,” for which polyvalent anti-snake venom is effective. Also significant and less known is the burden of other venomous snakes, one of which is Trimeresurus malabaricus. We report a bite to the face of a tree climber by Trimeresurus malabaricus in the Western Ghats of India, which caused severe local envenomation in the form of facial edema and systemic signs of envenomation, including coagulopathy and hypotension. We discuss the role of thromboelastogram, infrared thermography, and routine diagnostics in this case, which led to the administration of Indian-made polyvalent anti-snake venom. The patient recovered and was discharged without any clinically evident physiological or physical dysfunction.
Introduction
Snakebite is a neglected tropical disease, with India burdened by the highest number of deaths globally. Snakebite is attributed most commonly to the “big 4,” namely, the Russell’s viper (Daboia russelli), spectacled cobra (Naja naja), common krait (Bungarus caeruleus), and the saw-scaled viper (Echis carinatus). However, many other snakes of medical importance have been described over the years. 1 -5 In the Western Ghats of India, the malabar pit viper (MPV) (Trimeresurus malabaricus), bamboo pit viper (Trimeresurus gramineus), and large-scaled pit viper (Trimeresurus macrolepis), known Trimeresurus spp, are venomous and predominantly arboreal. 4 No specific anti-snake venom (ASV) exists for these species in India.
MPV envenomation remains largely unreported from the Western Ghats and coastal regions of southwestern India. In a hospital-based registry from the hospital that treated this case, MPV envenomation was more common than Echis carinatus and Bungarus caeruleus envenomation. We report a case with multiple bites to the face, potential upper airway obstruction due to severe cellulitis caused by the envenomation, coagulopathy caused by MPV, the potential neutralizing capacity of poly-specific Indian ASV in the treatment, and the role of thromboelastography in assessing the coagulopathy of MPV envenomation.
Case Report
A 44-y-old male, with no known comorbid conditions, from Honnavara, North Karnataka presented to the emergency department with swelling of the left side of the face after experiencing a snakebite while climbing a coconut tree at 1100. He was bitten twice, after which he immediately withdrew, killed the specimen, and presented to a local hospital where he was given tetanus immunization, diclofenac, and chlorpheniramine maleate and transferred to our hospital.
The patient arrived 6 h after the bite to the emergency department. The dead specimen was identified as an MPV (Figure 1) based on morphologic characteristics and the physician’s knowledge of species distribution in the region. On examination, he was conscious, oriented, and hemodynamically stable with a pulse rate of 60 beats·min-1, blood pressure of 120/70 mm Hg, hemoglobin oxygen saturation of 100% on room air, and respiratory rate of 18 breaths·min-1. An airway examination indicated no immediate threat to his airway. The local examination was painful with a diffuse swelling of the left cheek with multiple fang marks (Figure 2). Other systemic examinations were unremarkable.

(A, B) Killed specimen, identified as malabar pit viper (Trimeresurus malabaricus): green morph from Honnavara district-Near Sharavati, 14.2°N, 74.5°E. (C) Oral cavity of the specimen showing 2 fangs on the right with the left fang broken off. (D) Killed specimen. Full length of 57 cm with the typical black/brown spots over the dorsum arranged in a bold zig-zag pattern.

(A) Fang marks: 2 sets of fang marks with 1 indistinct over the cheek. (B) Victim’s face showing fang marks on the left cheek with edema extending to the neck.
A 20-min whole blood clotting test on admission was positive. A prothrombin time with international normalized ratio (PT-INR) was normal, and the thromboelastogram (TEG) revealed a mild hypocoagulable state with primary fibrinolysis with a normal R time (Figure 3A). ASV was not started. He was admitted in the emergency intensive care unit for further evaluation and observation and because of the high possibility of the need for airway intervention. A serial PT-INR done 14 h after the bite was prolonged, and TEG revealed a hypocoagulable state without hyper fibrinolysis (Figure 3B). He was also hypotensive with a blood pressure of 70/50 mm Hg. Ten vials of ASV (Bharath serums) were administered and a fluid bolus was given, to which he was found to be responsive. Intravenous amoxicillin-clavulanic acid, trypsin chymotrypsin, and paracetamol were given. A serial decline in platelets and hemoglobin was managed conservatively (Table 1). The elevated creatine kinase levels, serial serum creatinine, and urine analysis did not confirm renal injury. A peripheral smear done on Day 1 showed normal red blood cell morphology. He maintained normal urine output throughout the hospital stay. Serial PT-INR tests showed an improvement over the next 4 d (Table 2). Serial infrared thermography indicated a lower body surface temperature of the bitten cheek as compared to the left cheek and a normal temperature bilaterally on Day 3 (Figure 4). He did not develop any bleeding manifestations, renal injury, or airway compromise. He improved and was discharged on Day 4.
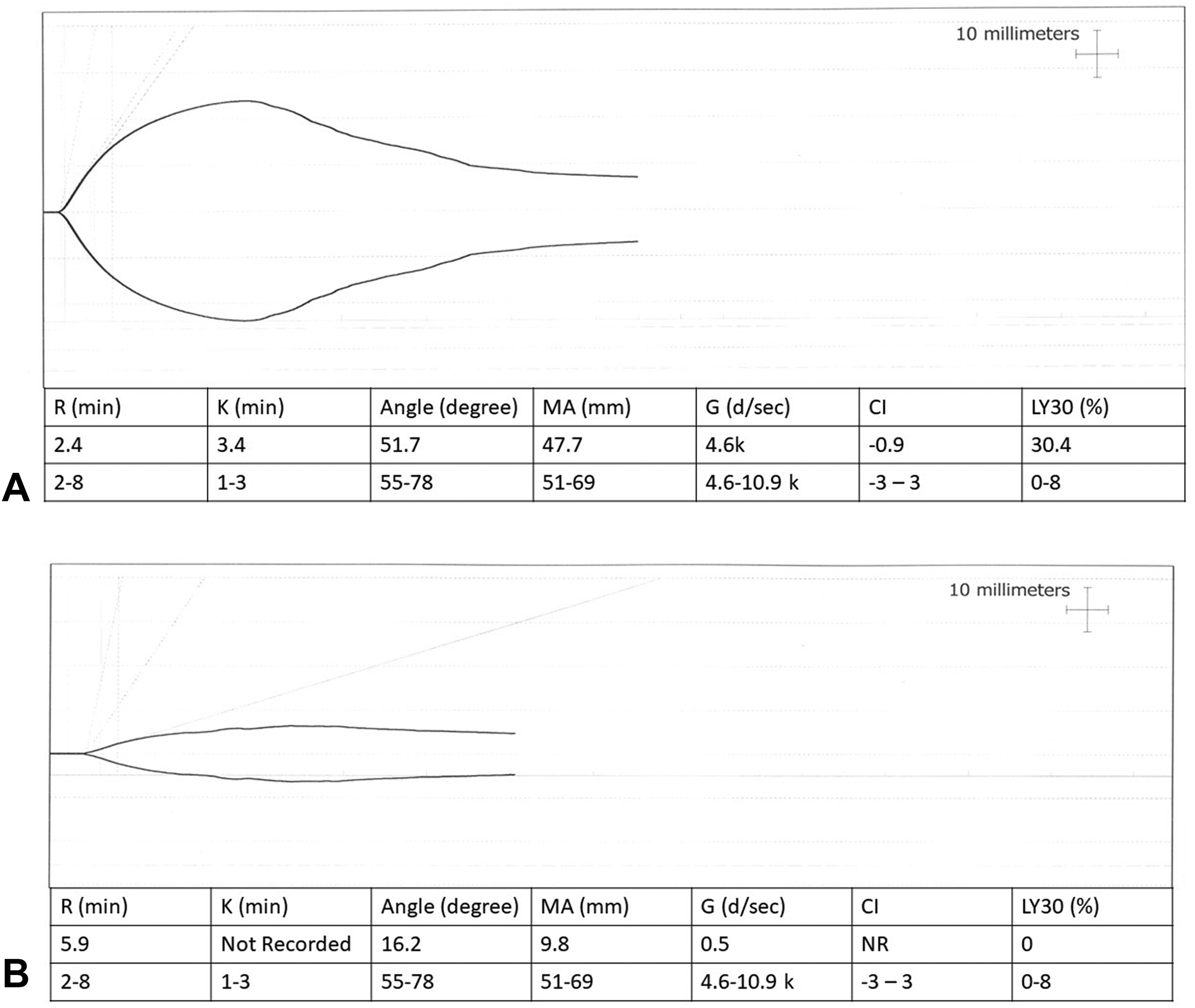
(A) TEG at the time of admission showing a mild hypocoagulable state with primary hyperfibrinolysis. (B) TEG after 24 h showing a severe hypocoagulable state, probably due to fibrinogen deficiency and no fibrinolysis.
Laboratory findings
CPK, creatine phosphokinase; Cr, creatinine; Hb, hemoglobin; LDH, lactate dehydrogenase; na, not done/not available; PLT, platelet count (lakh); TLC, total leukocyte count; hpf, high power field.
Coagulation parameters
aPTT, activated partial thromboplastin time; INR, international normalized ratio; na, not done/not available; PT, prothrombin time; TEG, hromboelastography; 20WBCT, 20-min whole blood clotting test.
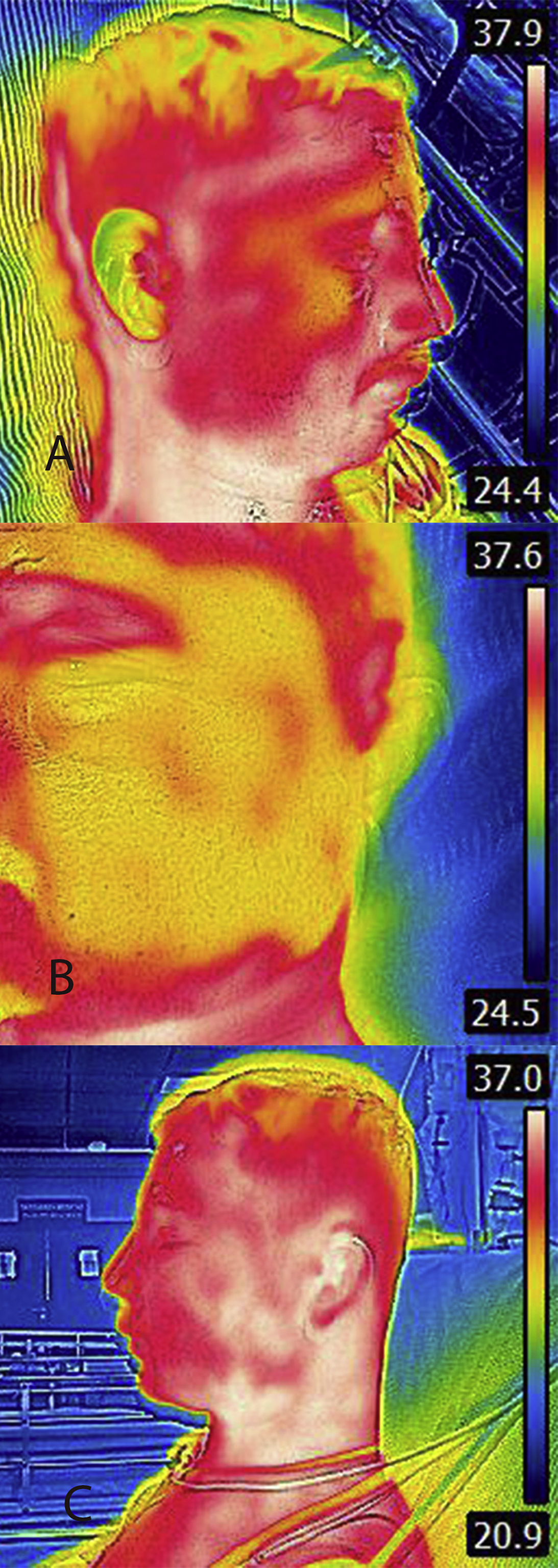
(A) Image of the opposite side of the face at the time of presentation. (B) Thermographic image of the bitten site showing lower temperature at the edematous area and higher temperature in the surrounding areas. (C) Image of the bitten side of face showing decrease in edema and swelling after ASV.
Discussion
The Western Ghats of India, one of 10 biodiversity hotspots, span over 1600 km, from Gujarat to Kerala, with an average elevation of 1200 m and the highest peak being 2695 m above mean sea level. The area is host to a wide range of endemic species. 6 The MPV is found in Maharashtra through Goa, Karnataka, and Kerala. It is arboreal, well camouflaged, and preys on amphibians and small reptiles.4,7 It is locally known as happatte havu. These bites are often unreported owing to the perception of their venom as being nonlethal.
Our patient was engaged in agricultural activity when he was bitten, after which he developed local edema that spread over the bitten half of his face and neck, impairing eye opening. In this situation, a potential airway compromise was anticipated; however, he maintained his airway and the edema subsided. Chymotrypsin and topical glycerin magnesium sulphate were applied, but it remains unclear as to how much benefit they offered in resolution of symptoms. Venom ophthalmia is caused by ocular contamination with venom (eg, by spitting cobras), 8 but facial bites by other venomous snakes may cause severe local envenomation and may secondarily compromise vision. 9 There was no evidence of venom ophthalmia in this patient.
Embedded fang fragments may be retained and result in infection or ulceration and hence should be looked for using x-ray or ultrasound. 10 In this case, ultrasound did not show evidence of the embedded fang.
Envenomation is mediated by phosphodiesterases, metalloproteinases, L-amino acid oxidases, and cysteine rich proteins, which may cause myonecrosis, hemolysis, platelet dysfunction, endothelial damage, and ion channel blockage.11,12 This patient’s creatine phosphokinase, renal function, and electrolytes were monitored; creatine phosphokinase was elevated. His hemoglobin dropped from 14 g·dL-1 on Day 1 to 11 g·dL-1 on Day 4, but there was no apparent bleeding or hemolysis, as evidenced by the work-up. The only attributable causes were blood sampling for diagnostic testing, rehydration, and mild extravasation at the bite site. MPV venom, as compared to Naja naja and Daboia russelli, can cause severe local tissue degeneration. 12 Ion channel dysfunction and myonecrosis may cause electrolyte imbalances.
Infrared thermography has been studied and used as a diagnostic and monitoring tool in many situations,13,14 including local envenomation. The device used was an FLIR E8 camera with an image resolution of 320×240 pixels and a thermal sensitivity of <0.05°C (0.09°F)×<50 mK. Although there was a significant difference in temperature between the normal and the affected side, the temperature was actually lower around the bite site, which is attributed to the edema fluid and low ambient temperature.
The mild coagulopathy caused by MPV venom is primarily fibrinolytic, mediated by phosphodiesterases, metalloproteinases, and serine-protease like proteins such as malabarase. 15 Although the patient had a positive 20 minute whole blood clotting test (MWBCT), the INR was only marginally elevated and TEG showed a mildly hypocoaguable state. 16 MPV venom has potent thrombin-like enzyme (TLE). 11 TLE acts mostly on the alpha and to a lesser extent on the beta domain of fibrinogen, leading to consumption of fibrinogen without fibrin production. The fibrinogen consumption was evident from the first TEG; the graph showed evidence of ongoing clot lysis and decreased clot strength with normal clot initiation (normal R time). TEG assesses the coagulation cascade in clot initiation (R time), clot kinetics (K time and alpha angle), clot dynamics (maximum amplitude [MA], G and coagulation index), and clot resolution (Ly 30) and hence provides a clear picture of the dynamics of in vivo clot formation, unlike PT or activated partial thromboplastin time (aPTT), which are static tests. The patient had signs of coagulopathy at the time of admission (Figure 3A), which later completely evolved into a severe hypocoaguable tracing in TEG because of the fibrinogen consumption by TLE (Figure 3b). The fibrinogen-fibrin-platelet crosslinking is traced by the parameters K time and alpha angle, whereas 80% of MA is contributed by platelets and the remainder by fibrinogen. 17
K time and angle were in the normal or low normal range in TEG (3.4 and 51.7 min) and MA was slightly reduced (47.7 mm) at the time of admission, with a fibrinolysis value of (Ly30–45%) indicating fibrinogen consumption due to venom-induced consumptive coagulopathy (Figure 3a). The repeat TEG had revealed more evolved coagulopathy in terms of unrecorded K time and a severely reduced angle (16°) as well as MA (9.8 mm) without evidence of ongoing clot resolution, indicating that venom-induced consumptive coagulopathy had completely evolved by that time (Figure 3b).
A normal R time in TEG meant the clot initiation was normal, which was also evident from a normal PT and aPTT on admission. The hyperfibrinolysis could be attributed to the defibrination by the TLE. Coagulopathy by TLE affects fibrinogen; the early coagulation screen by PT or aPTT may be normal and might lead to unwarranted consumptive coagulopathy if left to evolve fully. The authors also believe that measuring fibrinogen levels in Trimeresurus malabaricus bites might prove beneficial in establishing early consumption, where viscoelastic tests are not available considering the Indian landscape and resources. 18
ASV was initially withheld but, owing to the deranged coagulation profile the next day, 10 vials of Indian polyvalent ASV (Bharat Serums, Navi Mumbai, India) were administered. The ASV as per the manufacturer is only effective against the “big 4,” but there is some evidence of paraspecificity (Haffkine’s, 19 Virchow, and VINS 11 ). In vitro studies show the EC50 of ASV against MPV is significantly higher. 11
The patient was hypotensive on the first day but gradually improved on the second day. The 5’ nucleotidase in the venom is a hypotensive agent. 11 As analgesia, nonsteroidal anti-inflammatory drugs such as diclofenac are often used, but caution is recommended because they are associated with platelet dysfunction, anaphylaxis, and renal injury. 20
Although species identification is important, it may also lead to complacency. It is therefore important to identify and recognize the possibility of life-threatening envenomation in pit vipers. Trimeresurus malabaricus also presents a challenge in identification owing to its shared habitat with other Trimeresurus species and its varied morphologic features (at least 6 known color morphs). Syndromic identification is of limited value; therefore, there is a need for rapid diagnostic kits and species-specific/region-specific/pan-specific ASV.
Conclusions
We recommend that all Trimeresurus envenomations be considered medically significant. Thromboelastography is a useful tool for detecting and monitoring coagulopathy. The time to onset of systemic envenomation requires study, and the recommended period of observation should be modified accordingly. The role of Indian polyvalent ASV in these cases requires further in vitro and in vivo studies. Species identification is imperative for recognition of the burden and appropriate management of these cases. Research must focus on rapid diagnostic kits such as Dot-enzyme linked immunosorbent assay (DOT ELISA), 21 and species-/pan-specific antivenom needs to be developed as early as possible.
Footnotes
Acknowledgments
We thank Nirmal Kulkarni for his guidance and support on studies on pit vipers in the Western Ghats.
Author Contributions: Original draft of manuscript, imaging of snake and bite site, identification of snake (FMS); drafting of manuscript, reviewing, and editing (VL); IR imaging (CAS); TEG analysis (GM); critical review of manuscript (SS); approval of the final manuscript (all authors).
Financial/Material Support: None.
Disclosures: None.