
Abstract
The global problem of venomous snakebite continues to attract attention despite it being described as a “neglected” issue. The current focus of the World Health Organization (WHO) remains anti– snake venom quality, although “availability and sustainability” of supply are consistently described as the key issues. Sustainability of antivenom supply has been elusive, with cost and pricing in developing countries being cited as the major reasons. The current WHO approach fails to explore the cost issue, but rather focuses on quality improvements, which may well adversely affect the costs of a product already perceived to be ‘unaffordable.’ The reference to cost and price indicates a marketing-based perspective may well give more relevant solutions to the snakebite crisis. This paper introduces a marketing model to examine global snakebite and to identify if the current approach is relevant and effective. The “4 Ps” model examines if the correct products are available, whether sufficient information exists concerning estimated market size, whether the assumptions frequently made about the costs of the product are correct and fully understood, if the product is promoted properly, and whether the method by which the product reaches the end user is optimum. The resulting analysis demonstrates that the current approach is characterized by a misunderstanding of the nature of the global snakebite problem. Further, a lack of implementation of key solutions, such as training doctors in developing countries with relevant protocols, has inevitably led to a lack of improvement in the snakebite arena over the last 30 years.
Snakebite has been described as a “Neglected Public Health Issue,” 1 and yet a PubMed search on “snake bite” retrieves 740 results, and a Google Scholar search shows 9480 entries in July 2008. Add to this the books that have been published and the World Health Organization (WHO) meetings and many other conferences 2 –4 that have been held and it is difficult to justify using the term “neglected.”
Recent WHO meetings, commencing in January 2007, have echoed this view, and attendees have again proposed that the primary consideration in achieving a significant reduction in snakebite mortality is the production of more and higher-quality antivenoms (ASVs). 1 This proposition, having been discussed many times in the past, is not new, and, particularly in some areas of the world, has been regularly made over a number of decades, 5 –18 to such an extent that this concept now dominates thinking about solutions to global snakebite issues. 19
Despite the fact that the discussion purports to be concerned with “snakebite” mortality and morbidity, it rapidly becomes focused on “ASV supply and quality.” 1 Proponents justify this because the history of ASV provision in the 2 key snakebite areas, Africa and Asia, comprises a record of 30 years of failure. Repeatedly products have been both proposed and produced, but the vital element of sustainability has yet to be achieved.1,7,17
The WHO's stated priority is the following (emphasis added): “
Despite the fact that the discussion concerns snakebite, it remains focused on a small section of ASV, namely more and better-quality controls systems. Indeed, the recent WHO document states that to “solve” and “guarantee” global supply, “low volumes of production,” “poor safety and efficacy of some products,” and “deficient or non-existent regulation or control” are the priorities that need to be addressed most urgently. 1 The implication is that if more and better-quality ASVs are produced then the snakebite mortality and morbidity crisis will be largely resolved. However, are the real factors determining effective sustainable supply 1) better production systems or 2) further control systems?
When terms such as sustainable, production systems, price, supply, private takeover, privatization, lack of financial investment, and cost are employed it emphasizes the fact that a market factor is involved and therefore that a marketing approach is required to lead us to the root cause analysis of the current snakebite problem. 1 This paper introduces a marketing-based analysis to demonstrate that, far from being neglected, the real issue with snakebite is that it has largely been misunderstood and, therefore, has a poor strategic marketing mix that requires fundamental changes.
The concept of the “4 Ps”
When considering product performance in the market it is useful to view the situation using the marketing tool of the “4 Ps”—product, price, promotion, and place. 20 These factors constitute the “marketing mix,” which, in turn, determines whether a successful strategy in satisfying customer demand can be achieved (see the Table).
The “4 Ps” of marketing
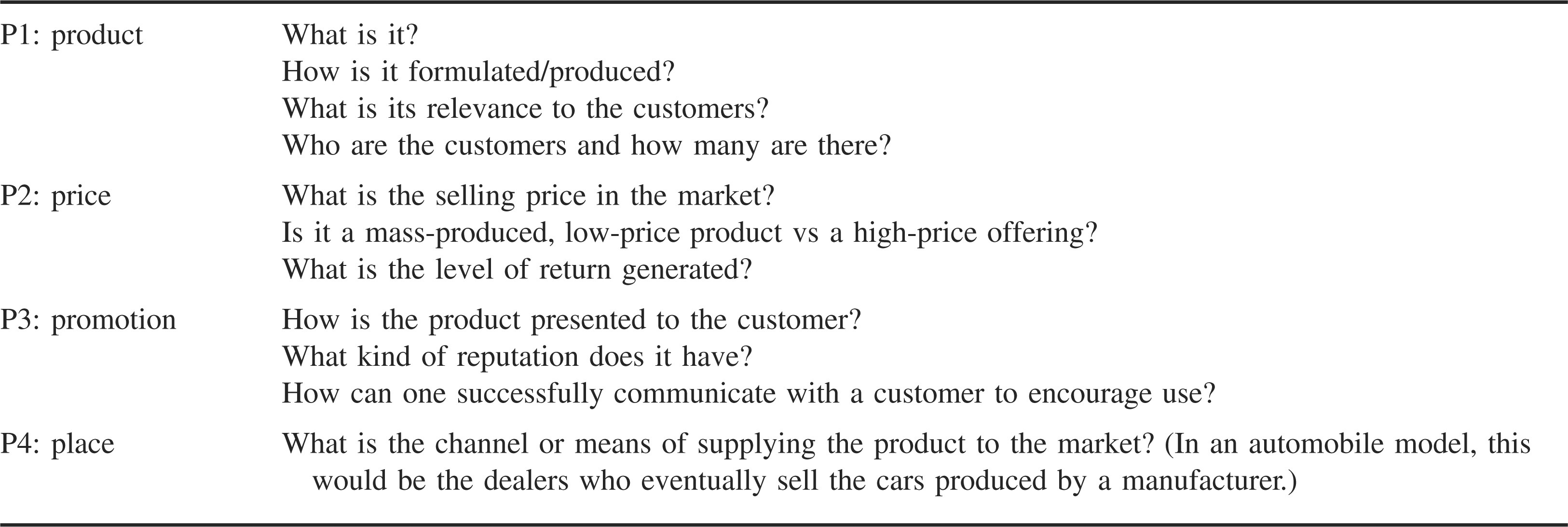
By generating the right combination of the 4 Ps successful strategies can be achieved to ensure a sustainable supply of the right product for the right customers. Creating the wrong marketing mix by having the wrong product or an ill-defined product, incorrect pricing, poor promotion, or an ineffective channel to market, either individually or in combination, can lead to disaster in terms of a failed strategy. In terms of snakebite management, what is the current marketing mix and does it suit the current strategy of reducing snakebite mortality?
The ASV “Product”
At first glance, determining the “product” in terms of ASV production might seem obvious, but this is far from being the case. Which ASVs are required and against which species should they be effective? Are they currently in place? It is very easy to ask for “more,” but more of what? It is interesting that a number of ASVs have been proposed that on closer inspection do not cover all species or the correct species for the area of concern.21,22 Even among the more experienced ASV producers, ASVs are designed that are clinically inapplicable as a result of a lack of understanding of the symptoms produced by different species. One such example from a leading ASV producer included the production of a “Bitis” ASV effective against Bitis arietans and Bitis nasicornis, with a second “Naja” ASV produced against Naja melanoleuca and Naja mossambica. Both ASVs were recommended for use in Mozambique, and yet the similarity of symptoms in victims envenomed by B arietans or N mossambica results in a lack of clarity in the mind of the physician as to which one to administer (unpublished). Snakebite envenoming is time dependent, and any hesitation results in greater time for the venom to bind. Physicians in areas in which these species are found require greater clarity in the case of a patient presenting with severe swelling produced by both species. 23
One Indian manufacturer attempted to penetrate the African market by obtaining the product insert of a current supplier of African ASV and by simply copying the species list contained within that ASV. Another manufacturer, invited to the WHO 2007 meeting, was cited for unscrupulously supplying ineffective ASVs to Africa, and an additional invitee is the regulatory body that presides over product insert literature that gives dangerous and outdated advice.24,25 It is therefore precarious to rely on the expertise of current ASV manufacturers as “authorities” in the provision of ASV. 1
What is required, but has yet to be provided by snakebite experts, is a comprehensive spectrum list of required ASVs with the species specified and the precise geographic area to which the ASV would relate.
Indian manufacturers have supplied to Africa ASV effective against related Indian species 26 –28 but ineffective against African species, and the results have been understandably and predictably poor. The selling price of this ASV in Africa is approximately 10 times the level in India; this cost elevation provides financial incentives to the manufacturer and is underpinned by the mantra of a “shortage of ASV.” One of the contributory factors that has enabled this practice to continue is the lack of clear guidance to purchasers and suppliers regarding what products are needed. Purchasing authorities simply ask for an effective ASV; they cannot determine whether the ASV is actually targeted at medically significant species within their country. There is often the assumption that ASVs are somehow universal and effective against all species. A clear example of this can be seen in African authorities purchasing Echis carinatus ASV when they should be purchasing a product designed for Echis ocellatus. While it is convenient to blame “unscrupulous marketing” for Indian ASVs appearing in Africa, no evidence is available that this was deliberate rather than an act of ignorance in an environment characterized by little guidance with regard to which ASVs should be supplied. 25 Further work needs to be conducted to determine a definitive required product list with respect to ASV before embarking on a greater or more expensive supply.
Product volume: The epidemiology issue, and how much do we really need?
A key aspect of product supply is the size of the market. However, the problem of epidemiology and quantifying snakebites—whether measured by number of envenomations or mortality—remains a major issue. 15 The recent WHO document mentions “low volumes of production” as a key weakness in maintaining a sustainable supply, and yet “low production” is determined vs what standard? 1 Various numbers have been suggested for envenomations: 2.7 million in a recent review, with world mortality estimated at 100 000 to 125 000 people per annum.1,30 The key consideration in terms of ASV production is that ASV providers rely on levels of envenoming in order to forecast supply, revenue, required assets, and cost of ASV production. If the numbers are incorrect, the resulting impact will be unsustainable supplies of ASV.
Numbers of bites/envenomations/deaths are usually derived from either government hospital statistics or from population surveys of small areas, with a subsequent extrapolation to national levels. 31 –33 Some authorities have argued that these 2 methods are the only methods available. 29 In many instances deaths per 100 000 figures from 30 to 50 years ago are applied across current populations, which have substantially increased. The underlying assumption is that more people equates to more snakebites. Yet there is no empirical evidence to support this theory. 34 The rapid increase in population, with the increased land clearance for food, may have resulted in a decline in the total number of snakes and bites. It is just not credible to use historical mortality rates and factor them across current populations. 34
Hospital statistics are notoriously unreliable given that recording processes, particularly in developing countries, are not robust. 35 Population surveys are given more credence by some as a result of their apparent reliance on prime data gathered during interviews with the population concerned.17,36 However, choice of population and reliability of both memory and identification of snakebite as the cause of death are highly variable. For example, the work of Hati et al 37 in West Bengal, used in the Chippaux 29 evaluation of world mortality levels, is based on a known peak snakebite district. Figures derived in this manner cannot be used to extrapolate the levels of mortality in all of India. 29 The sensitivities are just too great to merit using these figures as a guide to national statistics. As an indication, in a theoretical village survey of 20 000 respondents, a single mistakenly identified snakebite death yields a mortality rate of 5 out of 100 000 population. Factored across a population of 40 million this becomes a death toll of 2000 per annum, and yet these types of surveys are given undeserved credence.17,36
The notion that hospital-based figures are underestimates, as the majority of victims seek traditional treatment and may die at home unrecorded, is a long-standing, pervasive belief based on a small number of studies.1,4,10,35 This belief underpins the view that reported figures always “greatly underestimate the real impact.”1,17 However, 70% of all snakebites are from nonvenomous species, and of the remaining 30% resulting from venomous species, 50% require no ASV, as there is no envenomation.4,5,38 Traditional medicine treatments may cause no harm in these cases. However, victims who seek traditional treatment and are envenomed have been reported to seek allopathic solutions once they recognize that the traditional treatment has failed.2,39 It is therefore unsubstantiated to argue that the reported envenoming and mortality numbers should be inflated to reflect “the real impact.”1,17 The real issue, therefore, with traditional treatment is not that it understates the envenoming numbers but that it delays treatment to victims who are envenomed.
A principal drawback, which is overlooked in both these methods, is the reliance on terms such as envenoming as clear, unambiguous concepts. Numbers of envenomings are frequently reported alongside mortality figures.16,29 The notion of envenoming, however, is ambiguous. For example, those doctors in the developing world who gain their snakebite treatment guidance from Harrison's Principles of Internal Medicine 40 report envenoming to be defined by the following: “puncture wounds, pain, soft tissue swelling confined to the bite site.” However, in many developing countries, local swelling is not an indication of envenoming requiring ASV.27,41 In these areas, swelling must be severe and must fulfill a number of other criteria, including rapidly crossing a joint or involving half the bitten limb. The net result is that envenoming statistics are massively overstated and serve only to confuse and magnify the issue.1,29
The definition of envenomation should therefore be standardized as follows: “A victim receiving a sufficient level of venom to require the administration of ASV, as defined by criteria for administration applicable in that country or region.” Failure to accurately define envenomation serves only to support the erroneous view that more ASV is the solution to the problem of snakebite and misleads suppliers as to their likely sales volumes.
Alternative methods of mortality estimation
In terms of the key target areas (ie, Africa and parts of Asia), it is not credible that reliable statistics will be available in the required time frame to solve the problem of ASV supply. National data-gathering statistics are not robust and will therefore not be useful for demand forecasting for years to come. If more manufacturers are to be encouraged to enter the market and provide ASV they must be assured that it will be a sustainable activity with acceptable financial returns. In order to achieve this aim, volume forecasting must be more realistic and therefore more conservative.
For example, the key biting species with similar symptoms south of the line between the north Gabon border, Democratic Republic of Congo, and the northern border of Kenya are Bitis arietans, Naja nigricollis, N mossambica, Bitis gabonica, B nasicornis, and Hemachatus haemachatus. As they have similar symptoms, they would constitute an excellent polyvalent ASV with clear clinical guidelines as to usage. 23 Epidemiological information for this area is scarce, and, therefore, accurate statistics for envenomings are unavailable. However, it is possible to generate a basis for production. The population for the region is approximately 267.2 million; the work of Snow et al 42 on Kenya estimates 151 general snakebites per 100 000 population, with 20% from venomous species. Odio and colleagues 43 identified 80 (per 100 000 population) bites in the Democratic Republic of Congo. Blaylock 23 suggests an ASV administration percentage of 10% for species with symptoms of progressive painful swelling, the species that cause the majority of bites in the area, which would imply that approximately 10 885 victims require ASV. Based on a required dosage of 5 to 10 vials per victim, this would indicate a required ASV volume for the selected region of 50 000 to 100 000 vials.
These data are critical for suppliers, although they are not “accurate” in the sense that they are clearly correct! We are many years away from the “correct” number, and it will probably never be available. However, the above analysis shows that 50 000 vials of a credible ASV are justifiable. Whether it is economically sustainable to produce this volume and, if it is, at what price must it be sold are part of the next “P”—price.
Anti–snake venom “price” and economics
One of the key reasons cited for the consistent failure to provide sustainable ASV to key parts of the world is the cost of the product (ie, the purchasing price to governments and hospitals).1,44 Anti–snake venom is described as expensive and difficult to produce. Consequently, sustainable supply has been elusive, and pharmaceutical suppliers can be forgiven for a less-than-enthusiastic response to the issue.
Looked at differently, assume that a CEO of a successful pharmaceutical company has $5 million to invest in a new project. A team arrives to present a sales proposal for investment. The argument proceeds as follows: There is an unsatisfied demand for this product. Nobody has ever managed to provide it sustainably before. It is expensive and nobody has ever made money doing it. This product purportedly harms a great many people with adverse reactions. The product that was uneconomic before is about to be subject to a new level of unquantified costs for quality standards that are unproven. The level of demand for the product is unknown and the estimates are widely variable.
Despite the obvious weakness of this argument, this is the team approach of the WHO Department of Medicines Policy and Standards supported by a small group of selected advisors, who are proposing to focus on increasing control without any appreciation of current costs or the impact of the additional controls. 1
Anti–snake venom providers typically fall into 2 groups: 1) government producers for domestic consumption45,46 and 2) private producers for domestic and international consumption. Governments are prepared to subsidize ASV production to fulfill their own needs, and there are many examples in which this method has been successful (eg, India, Brazil, Mexico). Anti–snake venom is produced on a cost-only basis and is supplied free to government hospitals that deal with the majority of snakebites in developing countries. 46 However, if they are going to invest domestic funds for nondomestic uses, they will be compelled by market economics to generate profit, as these funds become investments and will be compared to alternative investments available. In this instance they become private suppliers and have private supplier incentives.
In many regions private manufacturers either supplement this production or provide the total supply (eg, Africa). The basis of this supply is of course market economics and the desire to provide shareholders with the market-required level of return. This is measured in terms of return on assets (ROA). When ASV is described as being “uneconomic” to produce, it is translated in corporate terms as generating an insufficient ROA, which leads private companies to seek investment of funds elsewhere in higher return products.
Return on assets is measured by comparing “return” (ie, profit) as a percentage of “assets” invested by shareholders and thus can be simply compared to interest on an investment in a bank. Despite ASV being described as “expensive to produce” and “uneconomic,” no analysis has been conducted to establish why this is the case. 47 It now seems to be an a priori assumption that “ASV is uneconomic.” 9 However, on what basis is this notion being derived?
Principally it is the African experience that is driving this line of reasoning.
1
Large Western pharmaceutical companies have withdrawn or are withdrawing from ASV production. The reasons for this are more complex than simply “unprofitability” and require deeper analysis. If return is defined in terms of ROA and if ROA = Profit/Assets×100%, a number of alternatives are possible as to why this equation is delivering a poor return: The price possible in the market is not sufficiently high to cover costs and generate sufficient profit.9,48 Costs of production are too high and thus inhibit generation of enough profit.18,45 The level of assets required to produce ASV is so large that it reduces the level of possible return. The volume of sales required to generate sufficient revenue, and therefore return, is not present in the market. A combination of any or all of the above are in effect.
18
Regardless of which of the above are operating, it clearly makes little sense to propose greater controls and therefore greater cost without understanding the current economics and the effect of any additional imposed costs.
The relationship between price and “cost” of ASV
The effects of any or all of these arguments would be easy to identify and quantify if the economics of ASV was actually known (ie, we could produce a profit and loss account and a balance sheet for ASV production). The fact is that such data have not been previously calculated, and an expected business case is unavailable for presentation to suppliers or potential suppliers. The concept of “ASV cost” is reminiscent of the ghost in Hamlet; it has a tremendous impact on proceedings, the audience never sees it, and yet 1 or 2 characters wander muttering about it, leaving death and suffering in their wake!
There are a number of available methods that are most widely used for ASV production: 1) ammonium sulfate precipitation of F(ab)2 fragments, 49 –51 2) ammonium sulfate precipitation of whole immunoglobulin G (IgG),49,50 3) caprylic acid precipitation of F(ab)2 fragments, 52 and 4) caprylic acid precipitation of whole IgG.21,48–50,53 Each of these methods will require an equipment profile, various chemical components, and staffing levels and will have varied yield statistics. The cost profile to produce ASV may well be very different under each method.
For example, it is well reported that caprylic acid antibody precipitation provides a 2-fold greater yield than does ammonium sulfate, and yet many manufacturers continue to use ammonium sulphate.46,52 At least a million vials are produced annually using ammonium sulfate, which implies that a further million vials are potentially available without increasing capital or production costs significantly. Indeed, the increase in yield on the same amount of base product (ie, plasma) may present the opportunity of increased supply at reduced costs. If we believe that there is a shortage of ASV, it seems only sensible to maximize the ASV return on the plasma generated, and yet clear recommendations in this regard from experts or the WHO have been conspicuously absent. 1
The obvious conclusion is that current ASV suppliers that use ammonium sulfate precipitation should be encouraged to transition to caprylic acid as soon as possible. New suppliers or processes should be caprylic acid–based, as this provides the most efficient yield and therefore the greatest amount of ASV. 52
A practical model
In the absence of a preexisting tool to assess the economics of ASV production it is useful to explore a likely scenario based on what published work is available, which, although exclusively from government suppliers, can nevertheless give useful insight as to the market case. The capital asset costs of setting up an ASV production facility in a developing country have been estimated at $2.1 million, excluding both land costs and a modern equipment array. 54 If the costs of land are added in, assuming market rates and an allowance of 0.5 acres per horse for pasture, and with a modern equipment array, the asset costs are approximately $4.3 million. Government models assume land will be given free of cost as the entity is a government concern; private companies, however, have to record the cost of the asset on the balance sheet, as it represents an asset of the business.46,54
The financial asset base is therefore $4.3 million, and this is the investment upon which private shareholders will expect a return of 20%. This implies that a return of $0.8 million is required each year in order to achieve acceptable and therefore sustainable returns (ROA = 20%).
47
It is now possible to model this required profit over a number of production volumes: 25 000 vials per annum = $32·vial−1; 50 000 vials per annum = $16·vial−1; 75 000 vials per annum = $11·vial−1; and 100 000 vials per annum = $8·vial−1.
These figures show only the profit element required in achieving acceptable and therefore sustainable returns. If we now include the cost element to produce the volume, it has been reported that $3.8 per vial has been identified as the cost of producing 60 000 vials of caprylic acid– precipitated ASV, at low titer levels, which is the most sensible level to assume for planning purposes. 46 These costs, however, are based on highly conservative government accounting rules, such as depreciating buildings over 50 years, plus costs assuming that only part of the building and people are going to be assigned to the project. 46 This is a perfectly valid argument if the facility is multifunctional and producing other products, but it will understate the true costs for a stand-alone unit. For the purposes of this analysis, only ASV production is being considered, so the costs need to be accounted for on a stand-alone basis. In addition, the costs of including key filtration and purification consumables (eg, Mobius Mixer disposable serum precipitation bags, Millipore Corporation, Billerica, MA, USA) and venom purchased from a reputable supplier for a 6-species African polyvalent ASV have been included, as they contribute to the purity of the product. Normal costs of a private supplier, such as marketing, clinical trial, and promotional costs, have also been included. When this is recalculated, costs per vial are approximately $9.8 for the first 100 000 and $4.3 for the next 100 000 vials as a result of the incremental costs required to produce them (I. D. Simpson, unpublished data).
So the likely cost to the end consumer per vial, including both costs and profit, can be calculated as follows: 25 000 vials per annum = $32 + 9.8·vial−1 = $42·vial−1; 50 000 vials per annum = $16 + 9.8·vial−1 = $26·vial−1; 75 000 vials per annum = $11 + 9.8·vial−1 = $21·vial−1; 100 000 vials per annum = $8 + 9.8·vial−1 = $18·vial−1; and 250 000 vials per annum = $3.2 + 4.3·vial−1 = $8·vial−1.
These costs show the
It is now possible to make some key observations: These economics show the effect of caprylic acid precipitation. If ammonium sulfate is used the volume is reduced by 50% as a result of yield effects (ie, for the same volume of serum, only half the number of vials is achieved; eg, $18·vial−1 becomes $26·vial−1. It is interesting that the 2 largest suppliers of ASV, who also provide it at the lowest cost, both use caprylic acid precipitation, whereas the lower-volume, higher-cost providers use ammonium sulfate (D. Narwate, oral communication, 2007). If volume predictions (ie, epidemiology) are overstated, then disaster in terms of sustainability ensues. Prices set at $18·vial−1 to ensure acceptable return at 100 000 vials are catastrophic if only 50 000 vials are sold, as profit and return are reduced by 50%. Shareholders will redeploy funds and the business will fail. Government producers do have an advantage, as land costs are often zero and it may be possible to exclude asset costs from the asset total for land and thus reduce the amount of return required.
54
Land costs are a large part of the asset base. Each reduction of $1.0 million in the asset base results in a reduction of $200 000 (ie, 20%) in the profit element. On a production volume of 50 000 vials, this would equate to $4 saved per vial. The potential drawbacks of government production, however, have been reported previously,
47
and government producers have been present for decades and have not provided the desired sustainable solution. Indeed, despite the failure of government suppliers to solve this problem for many years, some still lament that the privatization of ASV suppliers is detrimental.9,55 The impact of volume is critical. The higher the possible volume the better the economics. However, there are few places where production of high volumes can be achieved in one country, and developing ASVs for use in a single country makes little sense. India represents such a location, with an annual production in excess of 1.0 million vials. It is interesting, however, that even with a production volume by a single supplier of 500 000 vials per annum, the required profit to achieve an acceptable return in normal corporate terms is $1.6·vial−1 plus the cost of production. At the current selling price of $3.75·vial−1 offered by some suppliers in India, this would imply production costs of only $2·vial−1 (ie, 25% of the assumed level above). The above cost and profit figures demonstrate that ASV generates a high relative level of profit vs final cost per vial. The profit margins are in excess of 40% in all cases! This is a function of achieving a sustainable return on assets, and it makes no sense to criticize this and demand price reductions solely on the basis of the margin made by producers. The focus should not be on the percentage level of profit but on the overall level of return. The above costs are based on a stand-alone unit. If this unit is managed by a major Western corporate pharmaceutical company, then an element of corporate overhead may well need to be absorbed by the unit, which will further increase costs.
Unless a model can be developed in which ASV can be produced at an acceptable level of return, suppliers who enter the market will be short-term providers, as the lack of acceptable return will eventually cause them to leave. The lack of clear guidelines as to which methods to use to most effectively produce ASV is a key contributor to the shortage, and snakebite experts must take responsibility for this issue.
“Promotion” of ASV—What does this mean?
Anti–snake venoms in general have a poor reputation in the market; this reputation is largely driven by expert opinion over the risks of adverse reactions associated with using ASVs.1,6,17,56,57 The recent WHO publication states that early adverse reactions may be as high as 85%, despite the fact that the referenced texts show only 54%.1,6 In view of this, the expectation is that compelling evidence would be available that ASV reactions are a serious problem and that there are available statistics concerning the level of reactions and the number of life-threatening or fatal reactions; however, this is not the case.
Doctors have certainly been influenced by this “expert” opinion. Survey data in India and Pakistan revealed that 66% of doctors regard ASV reactions as a severe risk in snakebite treatment, and 91% would resort to giving a test dose, despite its lack of sensitivity or specificity, to try to predict an adverse reaction. 58
The quality of ASV is a key driver in the ASV provision debate, but unfortunately, the true impact on patient care of ASV is not well understood.15,48 No substantive work has been done to adequately quantify 1) the true incidence of adverse reactions, 2) the impact of such reactions in terms of morbidity and mortality, and 3) the cost-benefit comparison of choosing between a lower-cost ASV, which may cause more reactions (treatable with cheap, available medications; ie, adrenaline), vs a more-expensive ASV with fewer reactions. 59 –62
In this environment of supposition and unsubstantiated opinion, the topic of “improving ASV quality” remains the key focus. 1 And yet, “quality” remains poorly defined. In some cases the term quality refers to how well an ASV neutralizes venom, 28 and in others, it refers to the propensity for the ASV to cause adverse reactions. For clarity, the ability of an ASV to effectively neutralize venom should be termed effectiveness, 18 while the term safety should be used for the rate of adverse reactions caused by the product.
While it is true that some ASVs produced in the developing world tend to generate a higher rate of adverse reactions than those produced in the developed world, the cost differential illustrates the substantial relationship between cost and quality.56,63,64 Stressing the improvement in quality of ASV to levels present in the developed world has significant risks that are commonly overlooked, particularly when the need for such quality is undemonstrated and uncosted. Papers have recommended that more attention be paid to viral threats from ASV, and yet no evidence to quantify or even establish a risk has been produced.1,65 The cost impact per vial of viral filtration can be as high as $2, which is a significant extra cost, based on nonsubstantiated opinion. 1
The single most important factor in ASV supply in the developing world is cost. Many underdeveloped countries or states within the more advanced developing countries simply cannot afford an increase in the cost of ASV unless there is a clear demonstrable need.33,59,66 Indeed, there is evidence that ASV cost is a potential hindrance to use and availability even in wealthy developed nations. 11
Even basic elements of the quality debate remain unresolved, such as the absence of clear guidelines on the similar results for numbers of adverse reactions produced by F(ab)2 and whole-IgG ASVs. 48 By their nature, whole-IgG ASVs are easier to produce, and yet, in the absence of definitive evidence, the view persists that F(ab)2 ASVs are “safer.” 9
The current WHO approach to increase quality standards in an uncontrolled and economically uninformed way, with a subsequent increase in cost in countries without the resources to purchase current products, will be counterproductive and will ensure that either less ASV is purchased and used or that the standards will be ignored.1,46,66
Product “place,” medical education, and training
The final “P” concerns how the product eventually reaches the end customer, in this case the victim. A car manufacturer analogy demonstrates that even with a good product, if the dealers who are actually selling the vehicle are ineffective, the strategy will fail, no matter how good the product, price, and promotion (the Table). Anti–snake venom availability is only one component of snakebite treatment. It is not the endpoint, although this is where discussions typically end, without significant consideration for how the ASV is used by the medical care provider.1,17 In order to effectively treat snakebite, ASV must be used efficiently, although this is not identified in the recent WHO report as one of the key weaknesses to ensuring a sustainable supply. 1 Even if ASV is available, it will not contribute to patient care unless it is used when, and only when, it is required and it is used effectively. This element of snakebite management relates to medical education and doctor confidence.
Medical education in the developing world, including the topic of snakebite management, is often based on textbooks from the developed world. These usually contain guidelines and recommendations that are inapplicable in a developing world scenario because of the general focus on well-equipped tertiary hospital treatment (rather than on treatment in primary care centers, which are closer to the victim but less well equipped).36,40,67–70
For example, Harrison's Principles of Internal Medicine is widely used for snakebite treatment advice in the developing world (India, Pakistan, China, and Nepal), even though its stated focus is North American snakebites.40,45,70 Research in India and Pakistan has shown that 94% of doctors gain their knowledge of how to treat snakebite from this key US textbook or from inappropriate local textbooks written by forensic medicine specialists who do not treat snakebite.40,68,71 Nearly 40% of doctors expressed no confidence in their ability to treat snakebite, and origin of knowledge and self-confidence to treat snakebite did not improve scores in tests of key snakebite knowledge. 58 Less than 50% of doctors recognized that incoagulable blood and visible neurological signs, key findings of significant envenomation, were indications for administration of ASV. Of the doctors who had gained their knowledge from the US textbook, 67% opted for a suboptimal dose of ASV, choosing doses prescribed in the textbook for North American snakebites. 58
Use of inappropriate training material, with unclear criteria on when ASV is required, leads to early use of ASV when it is unnecessary or, conversely, to delayed use when ASV is urgently indicated.10,27,38,72,73 Research in India has quantified ASV over usage. In one hospital it was determined that use of relevant local management guidelines reduced ASV utilization by 66%, saving approximately 19 000 vials. 41 Such wastage of ASV is not restricted to the Indian subcontinent. It occurs in southern Africa as well (R. Blaylock, oral communication, 2008) and is likely common in many developing regions.
Guidelines for snakebite management must include recommendations concerning 4 key aspects of ASV utilization: 1) criteria for administration, 2) dosage, 3) repeat dosage methodologies, and 4) clinical endpoints for ASV administration. These are, however, completely inappropriate or not covered in sources of medical education or guides prepared without significant local involvement.10,27
India and Pakistan have responded to these concerns by producing and implementing protocols developed with reference to the local conditions and involving local expertise, supported by bedside material and training that is workshop based and that involves all layers of health provision. 58 Both of these protocols have been launched since the 2007 Geneva meeting, but no others have been forthcoming. This is a key area requiring urgent action. The positive impact of implementing such locally developed protocols has been very encouraging.41,58,74,75 Development of national protocols, cascaded to the doctors at the front line of snakebite treatment, is key to reducing mortality and morbidity and to ensuring that treatment is not just effective but also efficient in terms of health resource and ASV utilization.15,76
In India and Pakistan, the development of protocols targeted at each segment of the health service has had a major response in encouraging primary care institutions to effectively treat snakebite. 74 Protocols need to be developed that match the actual treatment structure on the ground, recognizing that the closer to the bite that the victim can be treated, the more successful the outcome can be. 77
Local protocols also largely address another key concern of developed world experts—infrastructure. If a patient is noted to take 6+ hours to reach the hospital, the assumption is that access to vehicles and road conditions are the key barriers. 78 However, while infrastructure does play a part in terms of road transport, more significantly the delay is often caused by the fact that care providers in closer hospitals are not adequately trained to treat snakebite and lack confidence to do so. These care providers, therefore, resort to immediately sending patients on to more distant, better-prepared facilities for care. It is useless to point out that ASV is not available in peripheral hospitals if the doctors are not trained or confident to use it. 1 This, of course, lengthens the time it takes patients to reach the first effective medical contact. 79 In addition, innovative solutions can be developed locally, such as the process of rapid transport in Nepal; such solutions may be beyond the experience of developed world experts. 36 Infrastructure is too crude a concept to be used without identifying some of the underlying root causals that affect the delay in reaching medical care. 15 Proper training of staff at the primary point of contact reduces the impact of infrastructure.
Conclusions
Despite the fact that the historical focus on ASV production and control has been determined to be key, no discernable change has been evident in either ASV provision or, more seriously, snakebite mortality.3,65 The required marketing mix to achieve significant reduction in morbidity and mortality is not yet present, and of concern are those current initiatives that seem targeted at repeating past mistakes. 1 The recent WHO document identifies 7 essential components of a strategy to solve the ASV availability problem. The first 4 components deal with ASV guidelines, production, and control; the fifth component deals with improved clinical management of envenomings; the sixth component deals with ASV distribution; and the final component deals with identifying a financially sustainable strategy. 1 The targets and prioritization reveal a fundamental misunderstanding of the problem, with medical training and financial sustainability receiving significantly less focus and energy than do production, regulation, and control issues.
What is required is a new marketing mix with the following elements: A commitment to implementation of a practical solution: Many of the recommendations have been present for several decades, and yet the situation, discussion, and even the participant groups remain unchanged.1,2 This is partly attributable to the organizational approach, which is fragmented in the case of the WHO. The Department of Medicines Policy and Standards group refers to many aspects of the snakebite problem over which they have no authority or ability to deliver solutions. Hence, progress remains elusive, and a central focus point is needed to handle the total snakebite issue. The WHO, however, concentrates in isolation, in attempting to “improve” a product, when they themselves argue that the top priority is “sustainable availability” and “long-term and sufficient supply of safe antivenoms.”
1
It is vital that the current exercise, being carried out by the Department of Medicines Policy and Standards Group, provide clear guidelines as to how ASVs should be produced; these guidelines should include recommended equipment arrays, costed outcomes to ensure sustainability, and sensible product requirements. A detailed list of products required for key areas with known shortages, such as Africa and Asia: These products or required ASVs should contain a list of the required species they are to be effective against and the geographic area to which they are applicable. Volume requirements should be established in a practical way, accepting that the “correct” number of envenomations is less significant than a reliable and sustainable estimate for ASV producers. The volume requirements should be based on the profile of the required ASVs in order to ensure that sustainable volume exists in each area. The economics of production should be rapidly calculated to determine the best production method, equipment profile, and likely prices for ASV in the market place. The lack of implementation is again the major issue, as cost-benefit analysis is referred to but never delivered; instead the unfounded assumption that “ASV is unavailable and unaffordable” is propagated without an attempt to address that issue.
1
Indeed, the WHO 2007
1
document concludes that the economic provision of ASV is best handled by soliciting charitable contributions from nongovernmental organizations or international agencies, without consideration of economic sustainability from manufacturers. In the absence of evidence to the contrary, the caprylic acid precipitation method should be advocated for new ASV producers, and current producers should be encouraged to migrate to this method in order to increase yield.
52
Quality improvements must be justified on the basis of cost-benefit analysis. Adding new control steps in an uncosted way is perilous, particularly when this method is not justified by facts.66,80 Clear guidance to producers and users of ASV that whole-IgG ASVs and F(ab)2 ASVs have similar safety profiles: In countries in which the current pharmacopoeias do not reflect this, updates should be made to enable whole-IgG ASVs to be produced and used.49,50 To support the list of desired products, a recommended equipment array for production would also benefit potential suppliers. This array may well be capable of being sourced from a single supplier, such as Millipore Corporation, which has extensive experience in providing these kinds of solutions and can provide technical support postinstallation. Interestingly, equipment suppliers were not invited to the January meeting, where they may well have been able to provide useful input and assistance.
1
The current lack of coherent guidelines (despite the inaccurate view that these are in the public domain) leads to developing world suppliers utilizing a variety of options that are not optimal in terms of quality or cost.
1
This item has been previously proposed by McNamee
44
but is still outstanding 7 years later.
54
Quality improvements must be presented to suppliers in terms of the overall economics of production. If yield can be increased, the improved profitability can be used to fund additional quality steps. Any attempt to mandate or recommend quality improvements without reference to overall economics will encourage current suppliers to reject them as a result of the cost or to leave the ASV market. Clear guidelines must be given to purchasing authorities regarding precisely which snake species should be covered by the ASVs they are sourcing and emphasizing that ASVs sourced from outside their geographic area will be ineffective. Once the product spectrum list detailed above is finalized, the list should be circulated to all purchasing authorities. Medical protocols to treat snakebite should be developed with major input from experienced, local care providers.13,76 The reliance on general textbooks and nonrelevant guidelines has resulted in poor treatment and wastage of ASV.10,41 This item having been referred to for more than 27 years strikes at the heart of implementation, yet it remains unresolved.1,2,4 In the 19 months since the original Geneva meeting in January 2007, 2 major snakebite countries (ie, India and Pakistan) have approved locally developed protocols.81,82 Local/regional protocols should contain clear guidelines based on the best available evidence on 1) snakebite first aid5,6,10,64,83–96; 2) medically significant species in a defined area; 3) establishing the 4 key criteria for ASV utilization
27
(ie, criteria for administration, dosage, repeat dosage methodologies, and clinical endpoints for ASV administration); 4) managing adverse reactions to ASV effectively11,19,61,62,97–100; 5) additional drugs for managing neurotoxic species, with a focus on drugs that are actually available locally, such as neostigmine methylsulfate10,83,101,102; 6) the proper use or avoidance of support drugs such as coagulants, pain relief, anticoagulants, etc; 7) specific guidelines for managing snakebite in nontertiary settings
92
; and 8) effectively and practically managing the airway, particularly in peripheral hospitals.
83
Training initiatives should support these guidelines, and practical bedside guides to treatment, applicable for the hospital setting (ie, primary, district, or tertiary care) need to be developed.
It is time to develop a new marketing mix that addresses all aspects of the problem, rather than focusing effort solely on a small aspect of ASV provision. The topic of snakebite has not been neglected, but pragmatic efforts to make significant reductions in mortality and morbidity certainly have been.
Footnotes
Acknowledgment
Prior to publication, this paper was submitted to the Director General of the WHO on August 13, 2008, to provide an alternative perspective to the exercise currently being carried out by the WHO.
*
No grants were received in connection with this paper.