
Abstract
Introduction
This study compared the casualties and types of rescues conducted on the main climbing route (MCR) and accessory climbing routes (ACRs) in Yushan National Park (YSNP) between 2008 and 2019.
Methods
We collected the following information for all documented mountain rescue operations conducted on the MCRs and ACRs in YSNP between 2008 and 2019: accident location, casualty type, victim number, and type of rescue. The victims were categorized as to injury, illness, mortality, or no medical problem (NMP) groups according to their condition at the time of rescue.
Results
Two-hundred forty-four rescue operations involving 329 victims were conducted during the 12-y study period. Among them, 105 (32%) did not require medical treatment, 102 (31%) were injured, 82 (25%) were ill, and 40 (12%) were deceased. Of the 82 individuals with illness, 69 (84%) had acute altitude sickness. The accident and mortality rates on the ACRs were significantly higher than those on the MCR (P<0.001; χ2). The ACR incidents involved significantly higher percentages of helicopter-based rescues and victims in the NMP group (P<0.001).
Conclusions
Acute altitude sickness accounted for most of the rescues. ACRs had higher injury and mortality rates and required more helicopter-based rescues for patients who did not have medical problems. This study may serve as a reference to reduce casualties and overuse of helicopters by educating tourists on the appropriate use of maps and the evaluation of trails in relation to weather conditions.
Introduction
Participation in outdoor recreational activities has increased in popularity in Taiwan in recent years.1,2 A 2018 national survey of recreation and the environment reported that approximately 45% of adults in Taiwan participated in some type of recreational activity in the mountains in the preceding year.
At a height of 3952 m, Jade Mountain is the highest peak in east Asia and is a common site for recreation. When engaging in outdoor recreational activities, individuals can risk activity-related injuries or illnesses that may require rescue. Rescue operations in Taiwan involve several organizations, including government and nongovernment organizations operating under the delegated authority of the fire administration. These operations are facilitated by ground-based rescue teams that collaborate closely with helicopter-based medical services.
Rapid evacuation and treatment can drastically improve the outcomes of mountain rescue operations.3,4 However, rapid rescues may be affected by the type of activity and environmental factors (eg, terrain and geological structures). 5 Reviewing and critically appraising historical rescue operations can help to more efficiently allocate future resources, optimize triage, and streamline protocols for rescue. 5 –11 The most recent study of mountain rescues in Yushan National Park (YSNP) was published in 2009 and concerned only victims who required medical treatment, excluding victims who called for help after becoming lost or trapped by weather conditions. 6
Our study compared the types of casualties and rescues conducted on both the main climbing route (MCR) to Jade Mountain and the accessory climbing routes (ACRs) in YSNP.
Methods
This study was approved by the institutional review board of China Medical University Hospital (CMUH110-REC2-116).
The national park is located in Taiwan’s central mountain range and, with an area of 1031 km2, comprises 10% of the total area of Taiwan. The park contains regions with altitudes ranging from 300 to 3952 m above sea level. Two-thirds of the park’s area has an altitude of >2000 m above sea level, and >30 of its peaks have an altitude of >3000 m above sea level. YSNP is becoming increasingly popular as a site for adventure recreation, and it has many climbing routes (Figure 1). The MCR is a route to Jade Mountain (red route on Figure 1); the other routes are termed ACRs. The most common type of climbing on both the MCR and ACRs is hiking uphill on trails. However, the routes have distinct environmental characteristics. The MCR is an adequately maintained trail with an elevation of 1342 m (from 2610 to 3952 m above sea level) and was the route used by most of the trekkers in YSNP in the study period. By contrast, the ACRs have high forest density and frequent landslides.
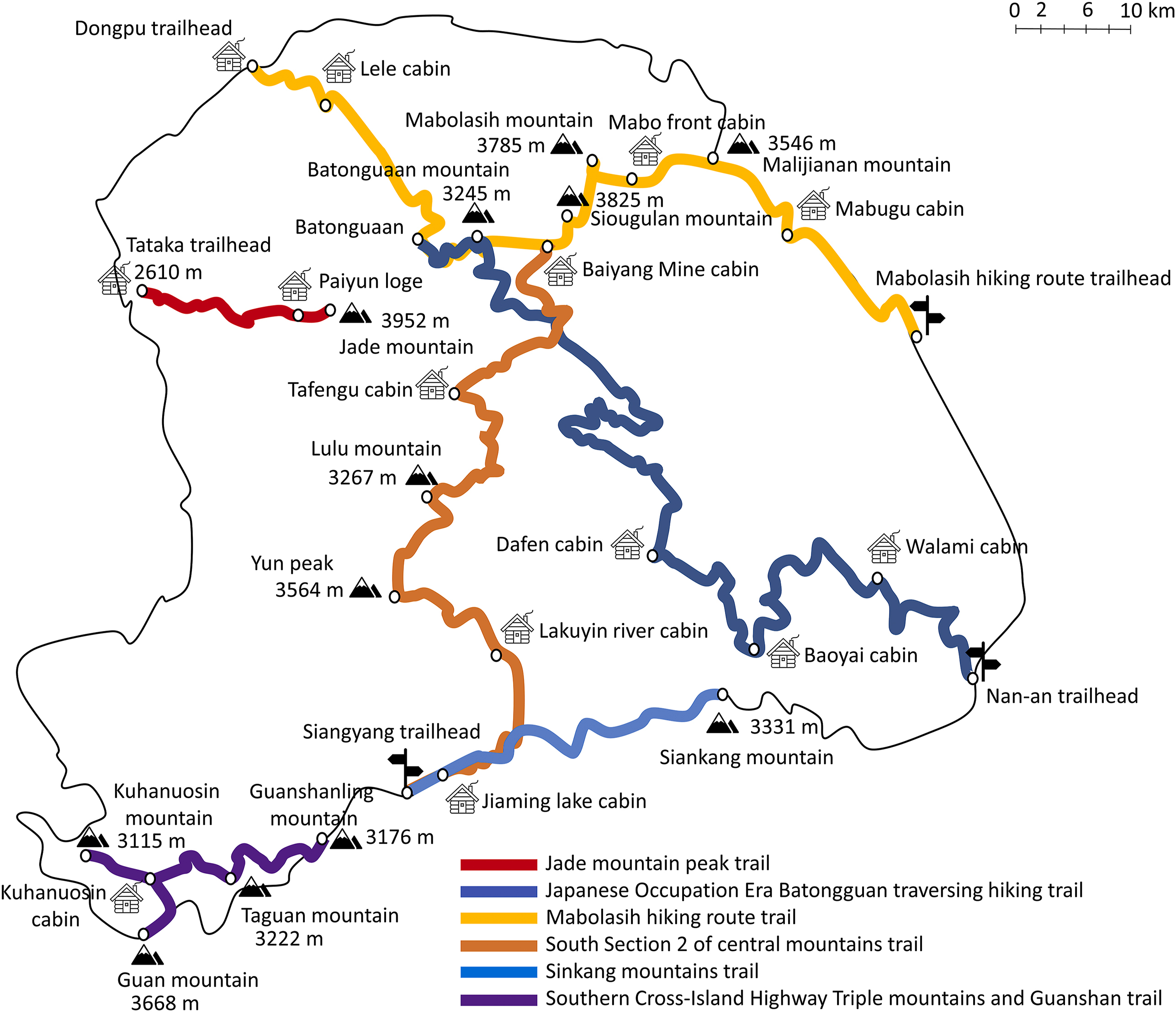
Trail map of Yushan National Park. The main climbing route is a route to Jade Mountain (red route); the other routes are accessory climbing routes.
This study involved retrospective collection of documented mountain rescue operations conducted in YSNP between 2008 and 2019. Incident data were gathered from standardized report forms generated by medical and rescue personnel at the scene of each incident. We excluded patients seeking medical services at mountain lodges without interventions from the mountain rescue teams. The data collected for each incident were the ages of the victims, the incident location and date, the type of rescue (ground- or helicopter-based), and the descriptions of the incident and associated fatalities, injuries, or illnesses. The victims were categorized into groups according to injury, illness, mortality, or no medical problem (NMP) at the time of rescue. Patients in the injury group were involved in accidents in which they sustained physical trauma, patients in the illness group were involved in accidents in which casualties occurred that required medical attention but were nontraumatic, those in the mortality group were involved in accidents in which a victim died before the rescuers arrived, and those in the NMP group were rescued without requiring medical support.
The primary outcome of our study was to analyze the types of casualties and means of rescue on the MCR and ACRs in YSNP between 2008 and 2019. The secondary study outcome was to investigate the evolution of mountain rescue medical care in an increasingly popular area known for outdoor recreation by analyzing rescues in YSNP.
Descriptive statistics were used to analyze variables in each category: the differences between categorical variables and odds ratios were analyzed using a ꭓ2 test. Statistical significance was set at P<0.05, and SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA) was used for the analyses.
Results
This study analyzed 244 rescue operations involving 329 victims over the course of 12 y between 2008 and 2019. The proportion of helicopter rescue interventions was highest in 2008 (70%) and lowest in 2011 (31% Figure 2), and the incidence of rescue operations increased in 2015.
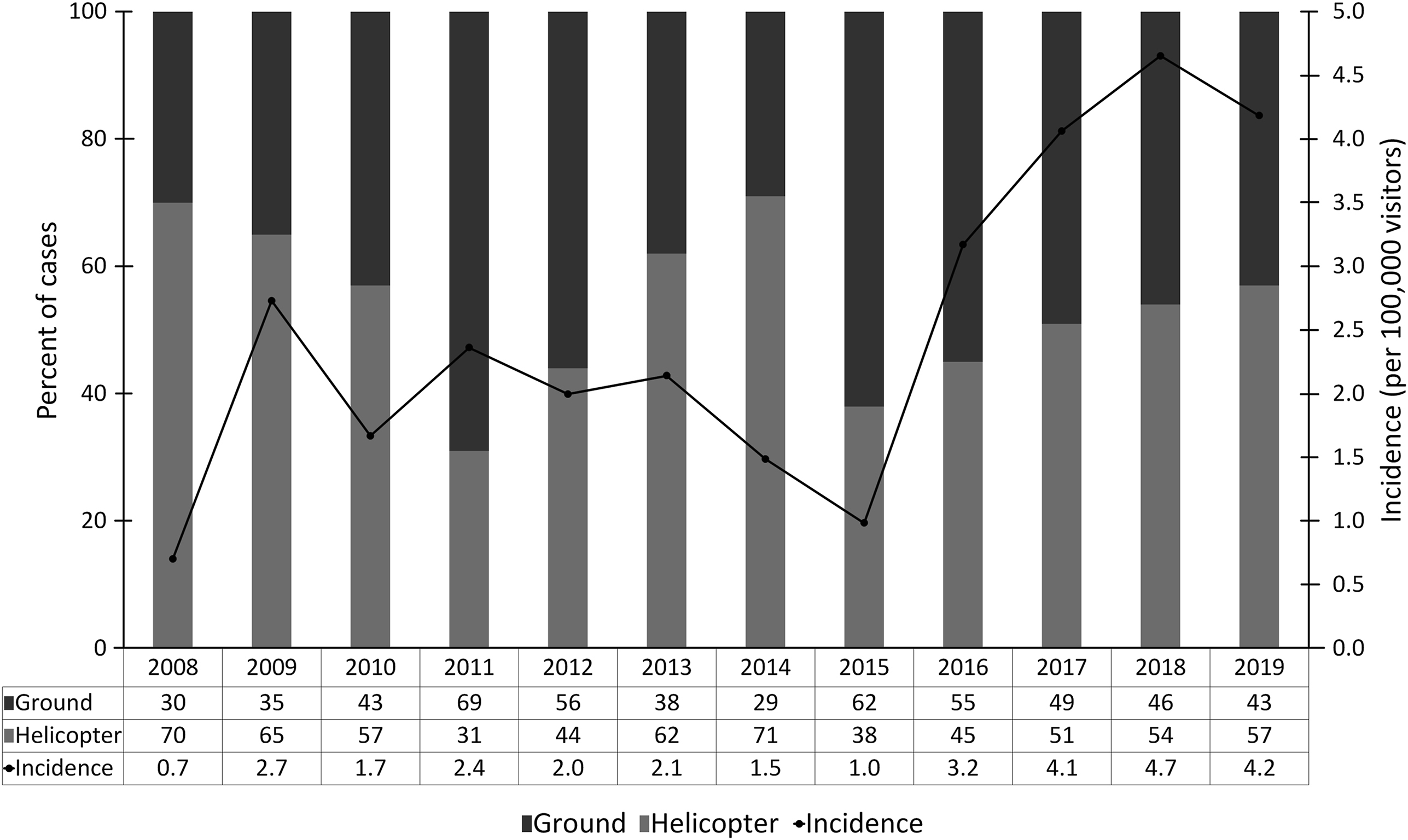
Incidence of rescue operations and proportions of helicopter-based rescue operations by year. The incidence of rescue operations began to increase in 2015.
Table 1 lists the distribution of each type of casualty and rescue, as well as the location of the each rescue. Among the 329 victims, 105 (32%) did not require medical treatment, 102 (31%) were injured, 82 (25%) were ill, and 40 (12%) were deceased. The most common nonfatal injuries were lacerations or contusions, multiple trauma due to falling, and sprains or strains. Of the 82 victims in the illness group, 69 (84%) had acute altitude illness. Of these, 60 had acute mountain sickness, 2 had high altitude cerebral edema, and 7 had high altitude pulmonary edema. Other common illness cause were gastrointestinal, genitourinary, and cardiorespiratory distress. The most common cause of mortality was trauma. Of the total 40 deaths, 27 victims died from trauma, 21 fell off cliffs and 6 were involved in air crashes. Most of the rescue operations (74%) were conducted on the ACRs.
The incidence of medical events and types of rescue associated with rescue operations on different routes in Yushan National Park from 2008 to 2019
MCR, main climbing route; ACR, accessory climbing route; OR, odds ratio; AMS, acute mountain sickness; HACE, high altitude cerebral edema; HAPE, high altitude pulmonary edema.
Over the study period, 13,341,262 people visited YSNP. Among them, 423,560 and 102,441 trekkers used the MCR and ACRs, respectively. The MCR was used by 81% of the trekkers in YSNP during the study period. The accident and mortality rates of the ACRs were significantly higher than those of the MCR (odds ratio [OR]=11.71, 95% CI: 9.15–14.97, P<0.001 and OR=19.50, 95% CI: 8.63-44.08, P<0.001, respectively).
Table 2 lists the details of the rescue operations on the MCR and ACRs involving specific casualty types and rescue means. The rescues conducted on ACRs exhibited a significantly higher probability of involving victims in the NMP group (OR=3.36, 95% CI: 1.67–6.74, P<0.001) and victims who had gotten lost or trapped by weather conditions. Moreover, the rescue operations conducted on the ACRs used a helicopter-based means of rescue significantly more often than did those conducted on the MCR (OR=3.18, 95% CI: 1.78–5.66, P<0.001). In addition, they were significantly less likely to involve victims who required medical treatment (OR=0.21, 95% CI: 0.10–0.42, P<0.001) and used a ground-based means of rescue significantly less often than the rescues conducted on the MCR (OR=0.29, 95% CI: 0.17–0.48, P<0.001).
Probabilities of types of casualties and rescues associated with rescue operations on different routes
MCR, main climbing route; ACR, accessory climbing route; OR, odds ratio; AMS, acute mountain sickness; HACE, high altitude cerebral edema; HAPE, high altitude pulmonary edema.
Discussion
During the study period, numerous rescue operations were conducted in YSNP. The incidence was higher than it was in the 2 decades preceding the study period (2.47 vs 1.18 victims/100,000 visitors), possibly because of the number of recreational hikers visiting the park increased. 6 The incidence of rescues was low in 2008 and 2015, which may be attributable to the closure of some of the ACRs because of natural disasters (specifically, typhoons Jangmi in 2008 and Soudelor in 2015). The average mortality rate during the study period was similar to that reported in the previous study (0.30 vs 0.24 deaths/100,000 visitors), and trauma remained the most common cause of death. 6 Most fatalities on the mountain occurred on the ACRs, probably because poor trail maintenance and frequent landslides increased the probability that visitors would fall off the cliffs.
Examination of the incident reports revealed that the 2 most common rescue categories were unrelated to the victims’ physical condition (ie, spatial disorientation and weather conditions) and injury, which is similar to other results reported in epidemiological studies of recreational areas.5,7,11 Acute altitude illness was the most common cause of illness rescue and was strongly associated with the MCR. The two key factors reported to favor the development of acute altitude illness were the hikers’ altitude and the duration of their exposure to high altitudes.12,13 The MCR spans 2610 to 3952 m above sea level. Because of convenient roads, the drive from sea level to the 2610 m entrance is only 70 km (approximately 3 h of driving), and some trekkers choose to drive to the trailhead and start hiking without an additional day of acclimatization. This rapid ascent may increase their susceptibility to acute altitude illness.
The rescue operations conducted on the ACRs involved victims who did not require medical treatment more often than did those conducted on the MCR. Callouts in response to spatial disorientation (ie, getting lost) were significantly more common on the ACRs than on the MCR, possibly because the ACRs are characterized by high forest density and because some areas are affected by landslides. The other common cause of rescues on the ACRs was an inability to continue along a route because of weather conditions. It’s possible that some of the hikers were unprepared for weather or altitude changes, which may have increased their risk of requiring rescue.
In Taiwan, 80% of the hikers who climb Jade Mountain via the MCR were reported having participated in high altitude (>3000 m) mountaineering <5 times. 14 However, the inexperienced hikers who used the MCR were not involved in more mountain rescues. This may be owing to the fact that the MCR trail is maintained combined with the fact that the hikers using the ACRs were not sufficiently prepared for the conditions they encountered. YSNP is home to 19 mountain lodges. Paiyun Lodge, located on the MCR, is the only lodge with medical facilities (as well as a doctor on weekends). The other 18 lodges are scattered throughout the ACRs and do not contain medical resources. Although hazardous physical environments can endanger mountain climbers and other visitors to the ACRs, other factors, such as inexperience or lack of preparation, which are in turn exacerbated by lower body temperatures, fatigue, and other medical conditions, can also pose problems. 15
Rescue operations occur more commonly on the ACRs than on the MCR, and the rescue operations conducted on the ACRs require more resources than do those conducted on the MCR. Our study showed that rescue operations on the ACR exhibited a significantly higher probably of requiring a helicopter-based means of rescue. According to previous studies, the risk of accidents is greater for helicopter-based rescues than for ground-based rescues, and this enhanced risk must be taken into consideration whenever a rescue operation is requested.16,17 The frequent use of helicopters to transport patients with minor injuries using the ACRs may increase risks for the rescue crews. 4
The results of this study may serve as a reference for professionals seeking to reduce the number of casualties and overuse of helicopters by educating tourists on the appropriate use of maps and on how to evaluate the trails in relation to weather conditions. Moreover, to reduce accident rates, tourists wishing to enter the park should undergo more rigorous qualification procedures, especially those tourists planning to explore the ACRs. In addition, different trails in the same area were associated with different types of causalities. This finding should provide additional insight when evaluating and managing risk. Knowledge of the main risks of exploring an area may help improve the information available for visiting tourists. In addition, training programs for rescuers can also be targeted to the main problem areas of the route where they operate.
LIMITATIONS
Our study had several limitations. The greatest limitation of this study was its retrospective nature. The data were collected from reports generated for each incident, and the possibility of recall bias therefore could not be eliminated. Furthermore, the incident data were recorded by rescuers with varied medical and first aid training. Therefore, considerable variation was present in the details contained in the incident reports. Moreover, our study did not include victims who treated themselves or who sought medical services at mountain lodges as opposed to calling the mountain rescue teams. Thus, the overall accident rates were likely higher than reported in this study. Furthermore, additional studies are warranted to further refine triage and transport protocols to ensure that helicopter transport is offered only to patients for whom the potential benefits outweigh the risks. In addition, information that we did not have—including follow-up medical records and outcomes of the victims who were injured or ill, detailed records about the medical treatment provided at the scene, and information regarding the experience of the rescuers involved in each rescue—could be used to bolster our findings. Finally, we focused solely on YSNP and our sample size was, which limits the generalizability of our results. Additional large-scale studies that use data from various outdoor recreation sites are warranted.
Conclusions
Our study found that the overall accident and mortality rates were significantly higher on the ACRs than on the MCR. The percentages of the operations involving helicopter-based rescues and victims not requiring medical treatment were significantly higher on the ACRs than on the MCR. In other words, most of the rescues on the ACRs involved uninjured individuals requesting helicopter-based rescue after getting lost or trapped by weather conditions. The results of this study may serve as a reference in reducing the number of casualties and the overuse of helicopters by educating tourists who intend to use the ACRs about the appropriate use of maps and on how to evaluate the trails in relation to weather conditions. Our results also suggest the need to select rescue team members not only on the basis of their medical knowledge and familiarity with medical equipment, but also with consideration given to the most common medical diagnoses seen in individuals who engage in outdoor recreational activities. Overall, our analysis provides additional insight regarding the main risks associated with hiking and climbing on both MCR and ACRs in YSNP.
Footnotes
Acknowledgements
Acknowledgments: We acknowledge the Yushan National Park for sharing data and experiences.
Author contributions: All authors contributed to the writing, editing, and revising of this article, and approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.