
Abstract
Mountaineering is a dangerous recreational activity with falls causing severe injuries and deaths. Survival from falls longer than 100 m is uncommon. We present a case of a high-altitude porter on Mount Everest who fell 400 m and survived. He slipped from a ridge at 7000 m (22,900 ft). A rescue party found him above Camp 2 (6600 m, 21,600 ft) and arranged a helicopter rescue. The Everest ER medical team at Everest Base Camp (5400 m, 17,700 ft) received the climber. They identified a head injury without signs of other serious trauma. A doctor provided manual inline stabilization of the cervical spine, airway support, and ventilation for the patient during the helicopter and ground transport to a tertiary hospital in Kathmandu. The time from the fall to definitive hospital care was 2.5 h. The hospital emergency team diagnosed an epidural hematoma and subarachnoid hemorrhage without midline shift and right parietal, orbital, and maxillary fractures. The neurosurgical team evacuated the intracranial bleed. The patient spent 6 d in the hospital. He had a positive neurological outcome. He had mild cognitive impairment and vision loss in his left eye but could perform activities of daily living. He returned to physical work, but not to climbing. This case report provides evidence that survival is possible after falls from extreme heights and sheds light on the challenges of an evacuation from austere environments.
Introduction
Mountaineering is one of the most dangerous recreational activities, with a high number of injuries and deaths from trauma. 1 Falls cause most nonfatal injuries in mountain climbers.2,3 Worldwide, falling is the most common cause of death in mountain climbing accidents, outnumbering avalanches, exposure, high altitude illness, and other causes. 4 Mountain climbers often traverse steep and icy terrain in remote areas. This puts them at risk of slipping and falling in regions far from definitive medical care. 4
Falls are a leading cause of climbing deaths in the Himalayas. Based on the Himalayan database, a computerized registry of climbing expeditions in the Nepali Himalayas, in the period from 2010 to 2019, 42 of 222 attributable deaths (19%) were caused by falls. 5 On Mount Everest, falls are the most common cause of death among climbers.5,6 There were 32 fatal falls from 2010 to 2019. 5 The site of the accident usually determined whether the event was fatal. If an accident occurred on steep terrain, it was more likely to have serious consequences.5,7,8 Victims who have uncontrolled hemorrhaging or multiple critical injuries after falling can have poor outcomes.9,10
Backpack weight distribution affects a climber’s balance and can contribute to a fall. 11 Heavy loads in the upper part of the backpack and unsecured equipment hanging outside the backpack increase the risk of a fall.
We present a case of a climber who survived a 400 m fall on Mount Everest. We discuss the challenges of evacuating patients from Mount Everest and the role of a rapid medical response.
The Himalayan Rescue Association (HRA) can provide rapid medical responses on Mount Everest. The HRA is a voluntary nonprofit organization established in 1973 with the objective of decreasing morbidity and mortality in the Nepali Himalayas. The HRA runs Everest ER, the only medical clinic on the Nepali side of Mount Everest not associated with a commercial climbing company. 12 Everest ER delivers primary care and emergency services to a population of >1600 climbers, guides, porters, and support staff stationed at the Everest Base Camp during spring climbing season.
Case Report
One day in early May at about 1430 (0 min), Everest ER received a radio call that a climber had fallen on Mount Everest. The details were limited, but the initial report indicated that the victim was a Nepali high altitude porter who was descending after carrying oxygen to Camp 4 (8000 m, 26,200 ft) for a commercial expedition.
Subsequent reports indicated that the victim was a 36-y-old climber who seemed confused prior to the accident and had unclipped from the fixed rope. He wandered off despite multiple attempts from the rest of his party to call him back to the fixed line. The party lost sight of him. Observers from other points on the mountain witnessed the victim fall from a ridge on Lhotse face below Camp 3 (7300 m, 24,000 ft). Observers had clear lines of sight. The climber fell a vertical distance of approximately 400 m (1300 ft), from 7000 m (22,900 ft) to 6600 m (21,600 ft). A rescue team of climbers from various commercial expeditions found him alive near the bottom of Lhotse Face between Camps 2 and 3.
The rescuers placed outwear over the victim and secured him in a sled. They pulled the sled about 200 m to an improvised helicopter landing zone near Camp 2 (6600 m, 21,600 ft). At +15 min, the rescuers requested a helicopter rescue. The victim was picked up and flown to the Everest ER helipad (5400 m, 17,700 ft) for assessment before their transfer to definitive care at a tertiary hospital in Kathmandu. The helicopter arrived at the Everest ER helipad at +45 min. The victim was unloaded from the helicopter to the helipad with spinal precautions. The patient was assessed by 2 doctors from the Everest ER team with assistance from an emergency medical technician. The medical team performed a rapid trauma assessment. The primary survey revealed no significant external hemorrhage. The airway was patent. The patient had blood-stained teeth, but no blood pooling in his mouth. He was breathing at 18 breaths·min-1. His heart rate was 90 beats·min-1 with strong carotid and femoral pulses. He had a capillary refill time of 1 to 2 s at the index fingers. The Glasgow Coma Scale (GCS) score was 5 (E1 V1 M3). The pupils were equal, round, and reactive to light (3–2 mm). The team did not have a thermometer, but the patient’s skin felt warm. There was no evidence of spinal injury. There was ecchymosis of the right frontoparietal and maxillary areas. Clear fluid, possibly cerebrospinal fluid, was running from the nose. There were contusions of the anterior chest. There was no obvious injury of the pelvis or long bones.
One of the doctors cleared the airway with a manual suction device and inserted an oropharyngeal airway. The team was preparing for endotracheal intubation when the patient started making purposeful movements. The GCS score was 9 (E2 V2 M5). The team decided to keep the airway open using a chin-lift and jaw thrust rather than by intubation. Before evacuation, the team administered dexamethasone 8 mg intramuscularly to treat possible high altitude cerebral edema (HACE). They applied a pelvic binder. They also covered the patient with warm blankets. The team transferred the patient into the helicopter using a spine board. They removed the board once they had loaded the patient. An Everest ER doctor accompanied the patient in the helicopter.
During the flight, the doctor stabilized the cervical spine with both knees and used a jaw-thrust to help maintain an open airway. The patient required assisted ventilation intermittently during the flight. The doctor ventilated the patient with a bag-valve mask at a rate of 10 to 12 breaths·min-1 targeting a lung-protective tidal volume of 500 mL.
After the helicopter landed at Lukla Airport (+75 min), the doctor and 3 airport ground crew transferred the patient using spinal precautions into a fully fueled helicopter. The transfer took approximately 5 mins. The doctor re-evaluated the patient finding his condition unchanged and continued manual inline stabilization of the c-spine, airway support, and ventilation until the patient arrived at the hospital.
The patient arrived at Tribhuvan international airport in Kathmandu at +120 min. The doctor and the ambulance crew transferred the patient into the ground ambulance using spinal precautions. The emergency department received the patient at +150 min.
The trauma team met the patient in the emergency department. The vital signs were: respiratory rate 18 breaths·min-1, heart rate 97 beats·min-1, blood pressure 133/62 mm Hg, temperature 36.4°C, and oxygen saturation on room air 97%. The GCS score was 5 (E1 V3 M1). The team performed a rapid sequence intubation and administered intravenous ceftriaxone and normal saline (1 L).
Computed tomographic (CT) images of the head showed an epidural hematoma and subarachnoid hemorrhage without midline shift, a linear skull fracture from the right supraorbital region to the right parietal region overlying the hematoma, and a lateral wall fracture of the right maxillary sinus (Figures 1 and 2). The CT images of the spine, chest, abdomen, and pelvis did not reveal traumatic injuries.
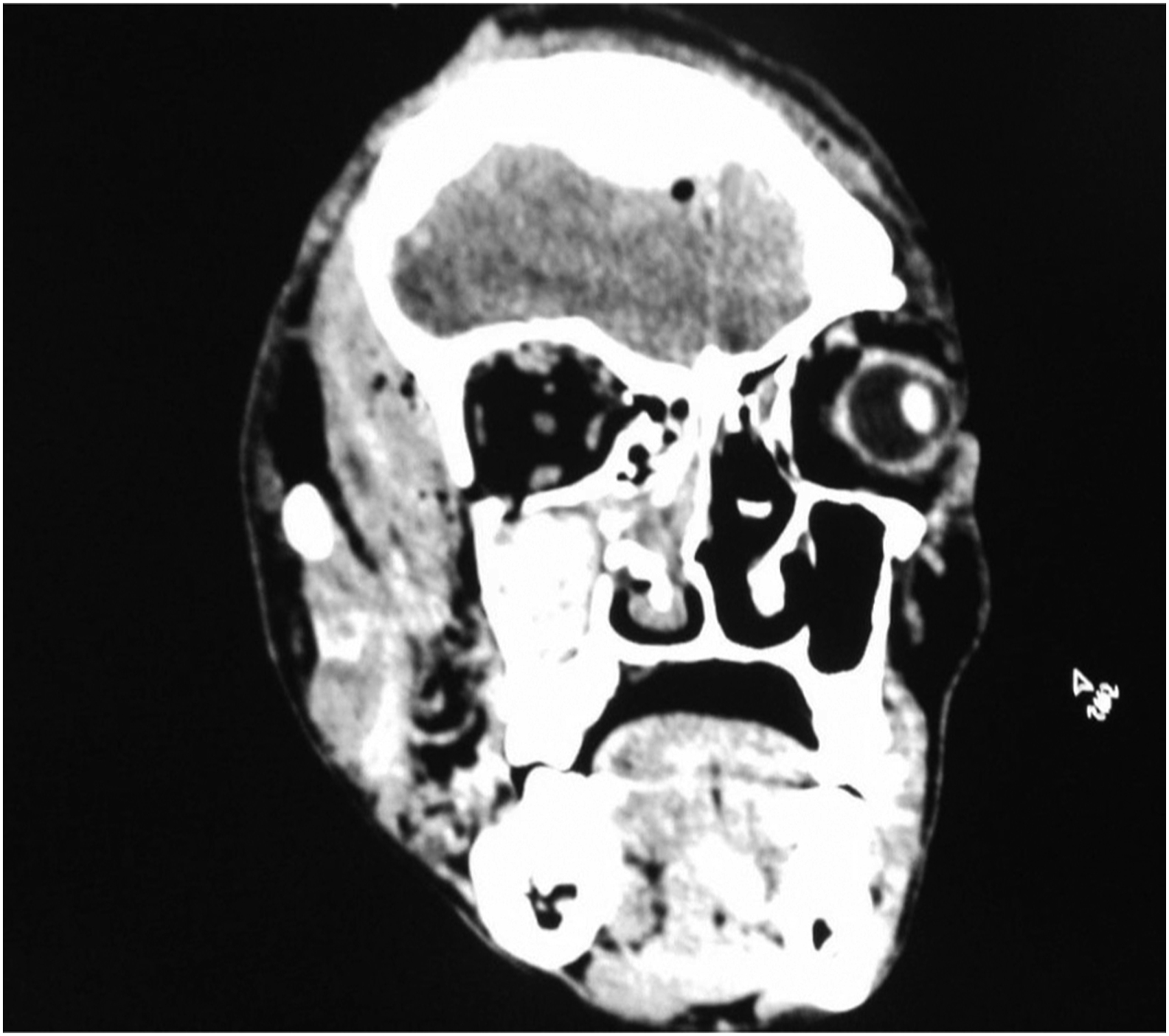
CT scan showing skull fracture in the right frontoparietal region, with lateral wall fracture of the right maxillary sinus with hemosinus involving right maxillary, sphenoid, and bilateral ethmoidal sinus.
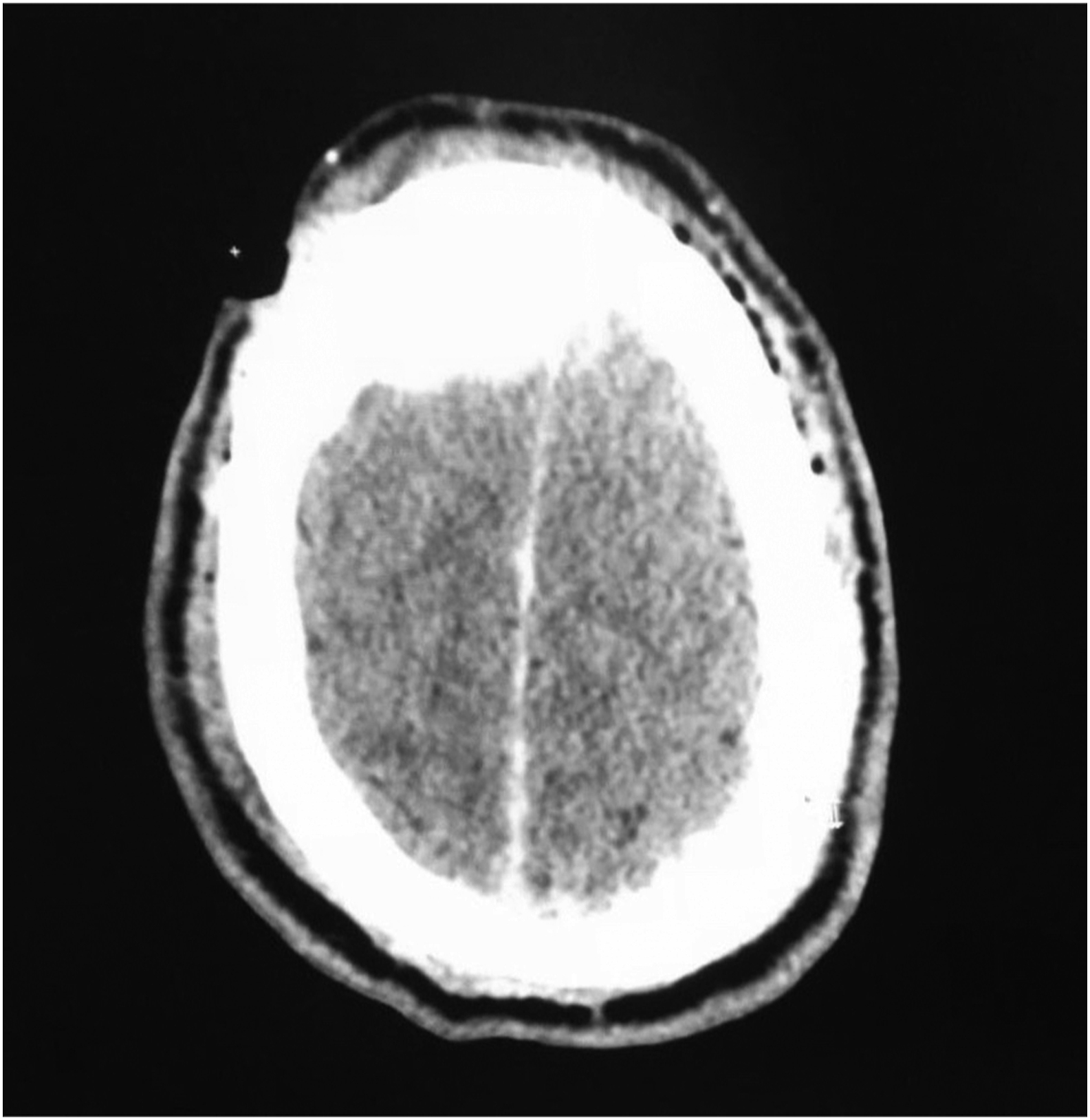
CT scan showing skull fracture in the right frontoparietal area, with subarachnoid hemorrhage and epidural hematoma formation.
The trauma team took the patient to the operating room for craniotomy, evacuation of the epidural hematoma, wound excision, scalp repair, and repair of the facial lacerations.
Postoperatively, the patient was admitted to the intensive care unit. He was extubated on Day 3 and transferred to the ward. He was discharged from the hospital on Day 6. The patient had minimal, persistent cognitive impairment, but could perform activities of daily living. He had complete loss of vision in his left eye. He returned to physical work, but not to climbing.
Discussion
Survival from mountaineering falls >100 m is uncommon. We were not aware of other cases in the published literature. This case highlighted the challenges associated with rescuing victims from remote regions, such as the Khumbu region.
Despite the high-impact mechanism of injury, only the head injuries were severe enough to require surgical treatment. Airway management was the most immediate priority. Airway management was complicated by suspected traumatic brain injury and facial fractures. The team chose to defer intubation prior to transfer because of the high risk of a failed intubation with a technically difficult airway in an uncontrolled setting without signs of imminent airway collapse. The team also did not use a supraglottic airway, because the placement of a supraglottic airway might have triggered the gag reflex, causing vomiting and aspiration. 13 –15
The team managed the patient on the helipad because carrying him 100 m over rough terrain to the medical tent would have been time consuming and technically difficult.
The reported ataxia and confusion preceding the fall suggested a diagnosis of HACE. The suspected traumatic brain injury made it impossible to determine if the patient had HACE, so the team treated him for HACE with intramuscular dexamethasone. There was no evidence that poor distribution of backpack weight contributed to the fall.
The Aerospatiale B3 (Écureuil) helicopters and the ground ambulance were not equipped to provide critical care. This might have contributed to a worse outcome if the patient had more critical injuries.
Despite the challenges, the outcome was positive. The patient survived with a good neurological outcome. Luckily, he did not have an immediately life-threatening condition such as uncontrolled major hemorrhage. Prompt airway support likely contributed to a favorable outcome. The time from the accident to the arrival at the hospital was 2.5 h. This is faster than the average transport times for rescues and acute rural transfers in many developed countries. 16 –18
Conclusion
This report documented the survival of an individual after a long fall on Mount Everest. The patient survived because he did not sustain trauma requiring immediate intervention. Rapid rescue, prompt initial resuscitation, and timely evacuation to definitive care may also have contributed to the favorable outcome.
Footnotes
Acknowledgments
Thanks to those who provided eyewitness testimony. Special thanks to the rescuers and medical team, including Lakpa Sherpa and Deidre McCormack of Everest ER, Bruce Graham, Madison Mountaineering, Kailash Helicopter Services, and the receiving hospital (name omitted for confidentiality). Further thanks to Dr. Jonathan Reisman for reviewing the manuscript.
Author Contributions: Collating the case details (DD); literature selection (PK, DD); writing the manuscript (PK, DD); editing and reviewing the manuscript (DD). Both authors have read and approved the final version of the manuscript.
Financial/Material Support: None.
Disclosures: None.