
Abstract
Introduction
Despite near gender parity for women entering medical careers, women remain underrepresented in medical societies. This study evaluated the gender distribution associated with Wilderness Medical Society (WMS) activities.
Methods
A retrospective review was performed on the gender breakdown of the following WMS members: a single-day 2020 snapshot, conference attendees 2012 through 2020, conference presenters from winter 2017 through winter 2021, and leadership and awards data from 1984 through 2021. Genderize.io was used to generate probability-based gender categorizations (male/female) based on first names or pronoun associations.
Results
Gender was assigned in 91% (4043/4461) of 2020 WMS members, 92% (6179/6720) of 2012-2020 conference attendees, and 100% of remaining categories. Women represented 28% (1143/4043) of members, 27% (1679/6179) of conference attendees, 31% (143/465) of all conference presenters, 20% (62/303) of mainstage presenters, 23% (17/75) of all board members, 38% (14/37) of committee chairs, and 10% (2/20) of board presidents. Women received 18% (42/228) of recognition awards and 31% (15/48) of research grants issued.
Conclusions
Although women comprise a minority of WMS participants, gender distribution was similar across categories for membership, conference presenters, total board positions, and research grant awards. Relative underrepresentation was seen in the highest leadership levels, in recognition awards, and in mainstage presenters. Ongoing auditing may help to identify and address sources of bias and/or barriers to participation. Although it is only one of many components of equity, identifying successes and future opportunities for gender balance can strengthen the base of the WMS, promote growth, and ensure a strong leadership pipeline.
Introduction
Women make up approximately half of all medical students in the United States. However, female physicians constitute only 38% of full-time medical school faculty, 21% of full professors, 15% of department chairs, and 16% of deans. 1 A review of the 43 largest and most influential medical societies from 2008-2017 found that the medical society presidential leadership position was held predominantly by men, with only 17% of the president positions filled by women. 2 The same study found that women were particularly underrepresented among society presidents compared with active female physicians, and that 10 specialty societies had no female presidents over a 10-y time period. 2 Despite a growing number of female biomedical faculty, women continue to be less likely than men to advance in academic careers, to serve in leadership positions, or to receive awards in academic medical institutions and across biomedical professional societies.1,3 A closer look at prize winners in the biomedical sciences suggests that women are underrepresented in the most prestigious and higher monetary awards in the top US biomedical societies, and that when women do receive prizes, they are over-represented in less prestigious awards such as service, advocacy, and education. 4
Gender inequities in medical societies have individual and societal consequences. Participation and recognition in medical societies can impact career trajectory and influence promotion, mentorship, and leadership opportunities.2,5 The benefits in innovation and productivity from having more women involved in leadership, research, and decision-making have been well documented.5,6 Within the field of wilderness medicine, trips with gender-balanced leadership were associated with fewer participant injuries. 7
Identifying imbalances in gender representation is one of the first steps to addressing inequities. Many societies are starting to promote awareness of explicit and implicit bias with “gender report cards” to track gender representation at multiple levels. 8 By assessing, reporting, and responding to gender inequities, academic societies provide transparency and can progress toward gender equity. 9 In the Wilderness Medical Society (WMS) values statement, the society states that it recognizes the importance and benefits of a diverse and inclusive society and makes a commitment to fostering an environment of acceptance that is equitable to all. With these values in mind, our goal was to evaluate the gender distribution of WMS membership, leadership, and award issuance.
Methods
We conducted a retrospective review to categorize the gender of WMS members, conference attendees, conference presenters, board members, and award winners. We primarily used publicly available information, and the WMS administrative staff provided the first names of members and meeting attendees with no other personally identifying information or additional data. This effort was not subject to research ethics oversight.
The WMS database did not allow us to capture the names of members by year. We captured a snapshot of the members’ first names on a single day and used the gender distribution of conference attendees for conferences in 2012-2020 as a proxy for membership to document gender distribution over time. According to a communication from WMS staff (February 2022), only a small minority of conference attendees are non-members. Conference attendee data was not available before 2012.
Members and conference attendees were classified by first name using Genderize.io software (
We obtained the following names directly from the WMS: all WMS board members since the inception of the society in 1983, all recognition award recipients and grant recipients from award inception, conference speakers for 10 conferences from winter 2017 through winter 2021, the most current committee chairs as of April 2021, and conference chairs from 2018 through 2021. Personal knowledge of individuals by the authors was used in concert with verification of pronoun usage on professional or institutional websites. All individuals were classified as male, female, or unknown. Each speaker was given presentation credit for every presentation, whether presenting alone or in a group. We also evaluated separately the number and percent of female and male panelists. Panels were defined as discussion sessions with ≥3 advertised speakers, distinct from workshops with multiple instructors. Terms of service were captured for individuals holding the office of president.
Descriptive statistics were calculated in Excel. Chi square goodness of fit tests were used to compare gender distribution of awards and grants from 2012 through 2020, (the subgroups with enough people to make statistically valid comparisons) compared with the expected benchmark distribution of the average distribution of conference attendees over the same time period.
Results
Our membership snapshot captured a total of 4461 individual WMS member first names on August 17, 2020. Manual review of the Genderize.io output led to name reclassification in <3% of cases (n=118); 418 (9%) unknowns were excluded. Unknown names were reclassified to both female and male. Outcomes of member name classifications are shown in Figure 1.
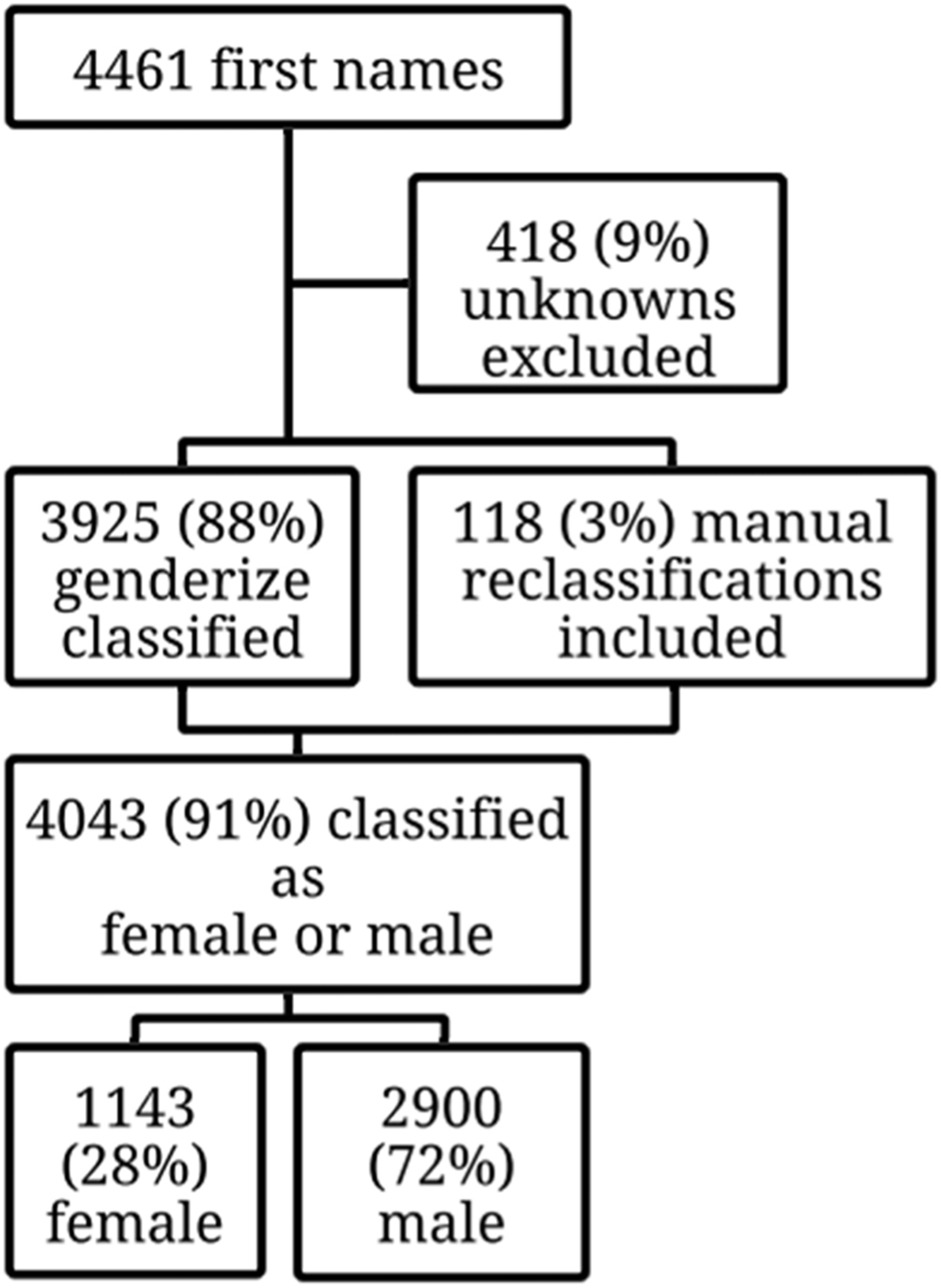
Gender distribution of WMS membership, August 17, 2020.
Gender classification of all conference attendees over the 9-y period included 6720 names. Manual review of the Genderize.io output led to name reclassification in <2% of cases (n=121); 553 (8%) were excluded as unknowns. The outcomes of conference attendee classifications are shown in Figure 2 and are illustrated by year in Figure 3. The higher number of conference attendees in 2020 corresponded with a virtual conference format employed that year.
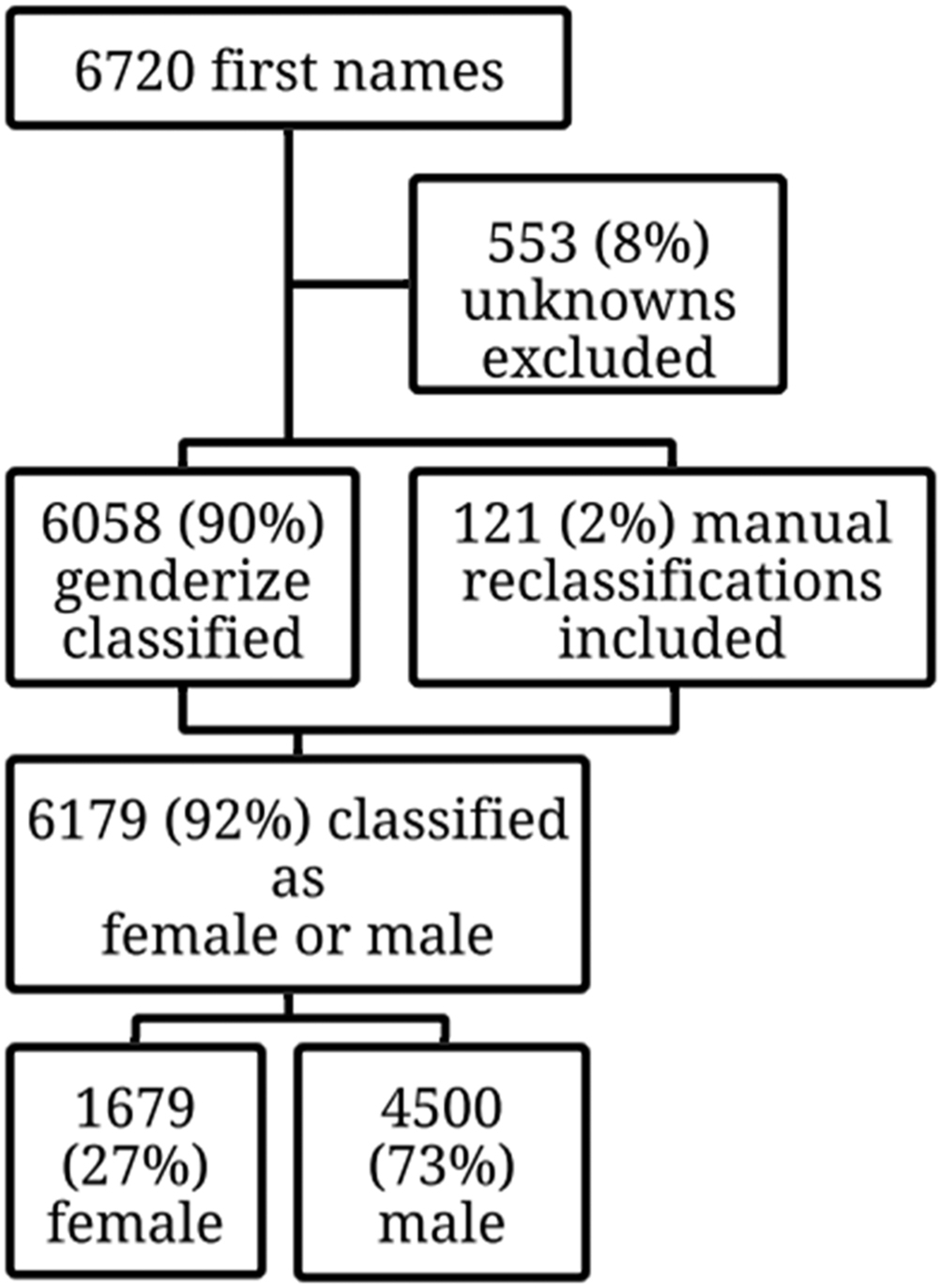
Gender distribution of WMS conference attendees, 2012-2020.
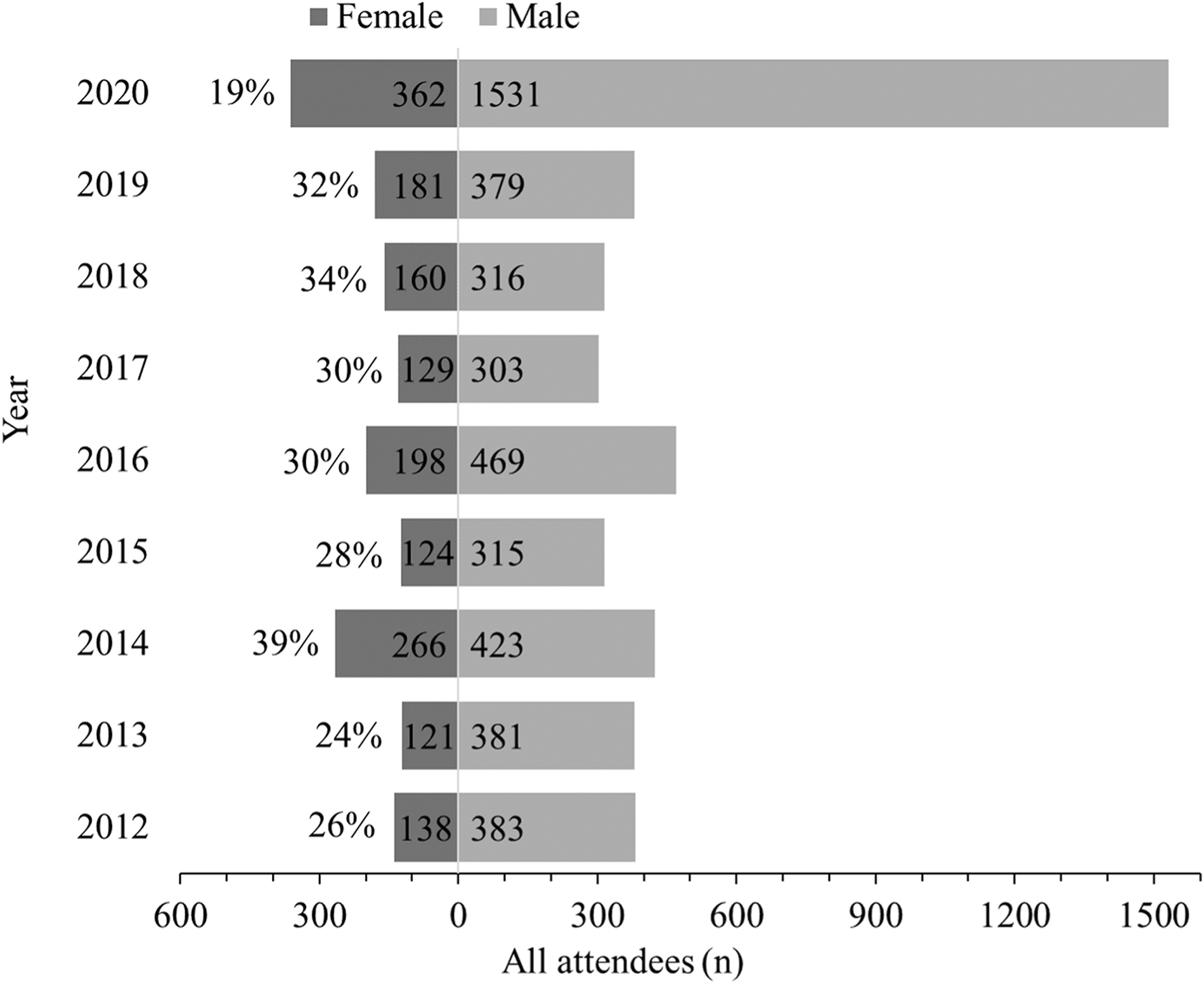
Gender distribution of WMS conference attendees, 2012-2020. Absolute counts are within bars, with the percentage of women represented to the left of the female bars. The unknown gender cases are not shown.
Women provided 31% (143/465) of all conference presentations, including small group sessions and workshops that were part of the main conference, but excluding separate pre-conference sessions and Diploma in Mountain Medicine classes and workshops (range 18-45% per event, Figure 4). Women accounted for 20% (62/303) of mainstage presentations (range 13-33% per event) (Figure 5) in the 10 WMS conferences held from winter 2017 through winter 2021. Out of all female presenters, 14% (20/143) were speakers on panels and 11% (16/143) were accounted for by 5 panels, of which 4 were women-only panels on the topic of women in wilderness medicine. Among the 5 conferences with panels, 26% (20/77) of female presenters at those conferences were accounted for by panel presentations.
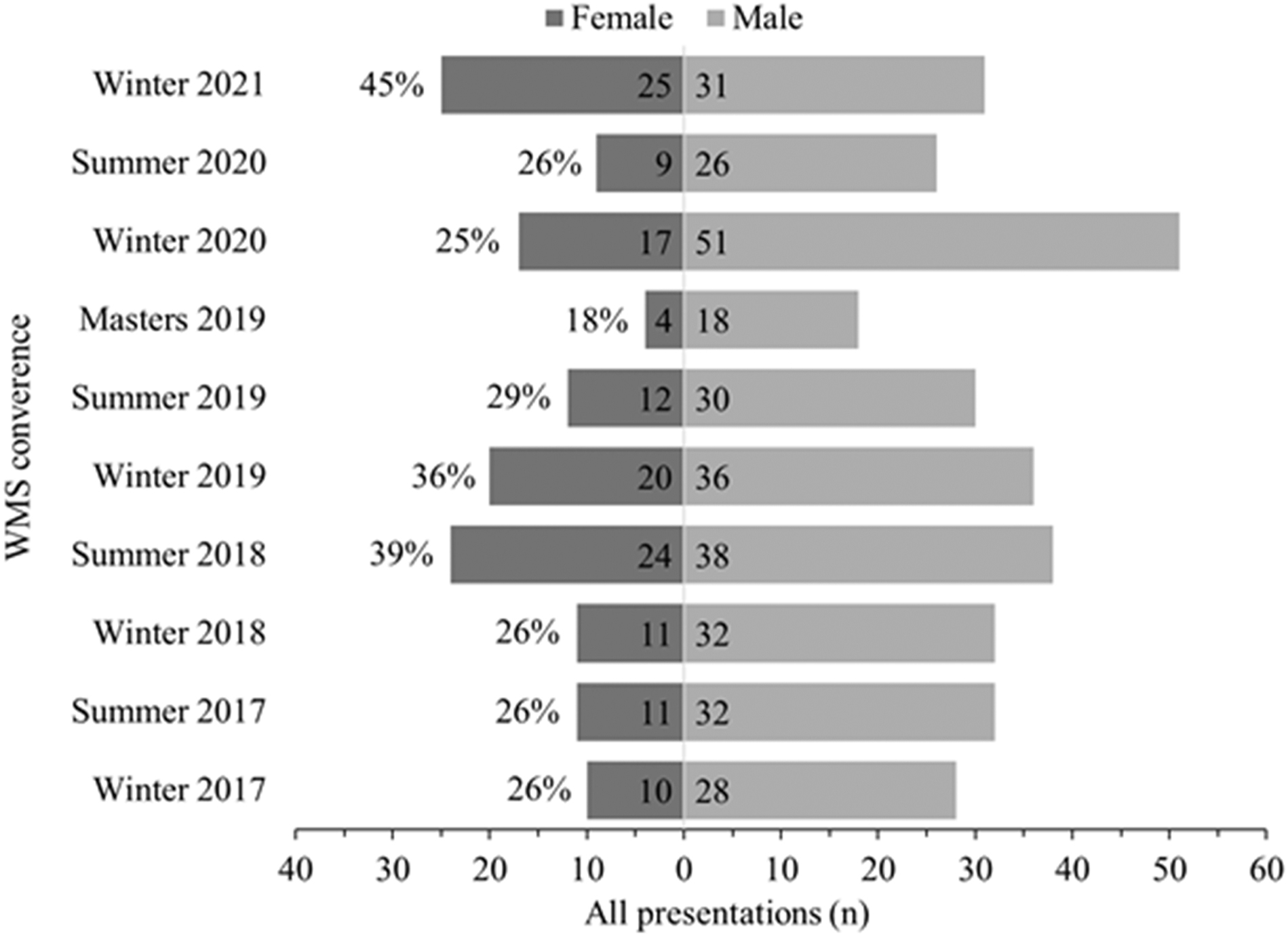
Gender distribution of all WMS conference presenters, 2017-2021. Absolute counts are within bars, with the percentage of presentations made by women represented to the left of the female bars. The unknown gender cases are not shown.
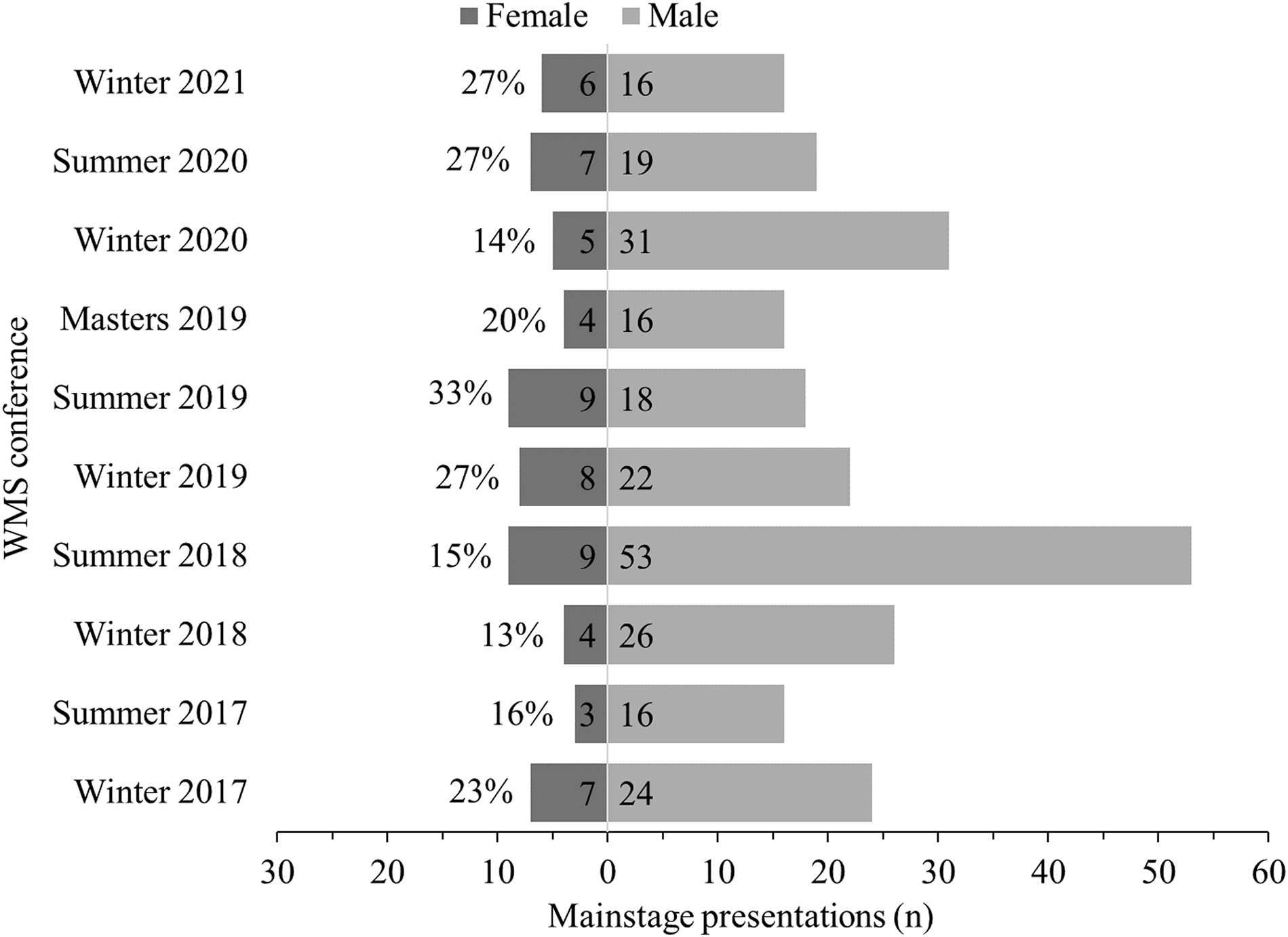
Gender distribution of WMS mainstage conference presentations, 2017-2021. Absolute counts are within bars, with the percentage of presentations made by women represented annually to the left of the female bars. The unknown gender cases are not shown.
Women constituted 23% (17/75) of all board members and 10% (2/20) of presidents over the 38-y history of WMS. Women comprised 27% (3/11) of WMS board members in 2019 and 2020 and 36% (4/11) in 2020 and 2021.
The WMS organizational structure includes committees that function under the board of directors (
The WMS began to issue recognition awards in 1994 (Table 1). Since then, the percentage of female recipients in each of the 10 award categories has ranged from 0-35% and overall, women received 18% (42/228) of all awards (Table 1). In the time period for which we have conference attendee data, women accounted for 24% (27/112) of awardees. These percentages did not differ statistically when compared with the gender distribution of conference attendees (X 2 [df=1, n=112]=0.34, P=0.55).
Gender distribution of WMS recognition award recipients, from award inception through 2020
WMS began to issue research funding awards in 2008 (Table 2). Women received 31% (15/48) of the total research grants awarded (Table 2). In the time period for which we have conference attendee data, women received 35% (13/ 37) of the research grants awarded, which was similar to the gender distribution of conference attendees (X 2 [df= 1, n=37]=86, P=0.35). To evaluate whether one or more individuals receiving multiple grants might influence percentages, we also counted the total number of individuals who won grants. The Hultgren grant has been awarded 12 times to 10 individuals (2 women, 8 men; with 1 woman and 1 man each receiving the award twice). No other grant has been awarded more than once to a single individual.
Gender distribution of WMS research grant award recipients, from award inception through 2020
Discussion
We report the available historic and existing gender proportions in the WMS to identify gender disparities and opportunities for the next steps. Our key finding is that women are a minority across all WMS roles, although the gender distribution of speakers, board members, and award recipients generally reflects the gender distribution of the membership and conference attendees, with some notable exceptions (described herein).
In our 2020 membership snapshot, the proportion of female membership, approximately one-third, was similar to the proportion of female conference attendees. Women comprised a smaller minority in leadership, mainstage speakers, and multiple award categories. The proportion of women holding committee chair positions declined with ascending rank in the organization structural hierarchy. Similar to trends identified in other specialty societies, the situation is most imbalanced at the highest levels of leadership. 2
The total percentage of female conference speakers reflects the percentage of female conference attendees. However, the percentage of female main stage speakers was lower across multiple conferences. The lowest percentage of female main stage presenters occurred in the fairly recent conferences in the winters of 2018 and 2020, at 13% and 14%, respectively. Further analysis showed that all-female panels boosted female percentages. The proportion of female mainstage presenters changed little over the 5-y period evaluated, with half of the conferences featuring male presenters 4 or more times as often as female speakers.
The recognition awards with the greatest number of female recipients were for outstanding research presentations and service awards. This stands in contrast with the awards with the lowest number of female recipients, both of which are better described as leadership awards. This pattern supports prior work of others that found women more often won prizes awarded for reasons such as education, support, teaching, and public service compared to research or leadership awards.4,11 Of the 2 award categories with the lowest representation of women winners, the proportions were 0 and 7%. Other authors have noted that “low stakes” awards tend to be more equitable, but more prestigious awards tend to go to men across scientific and medical societies. 12 -14
We were not able to assess why so few women have been recognized in some categories. Without the ability to show the gender composition of society membership through the time period of award history, we cannot assess relative representation for awards whose inception date occurred before the time period for which we had membership or conference attendee data. The proportion of female recipients of research presentations and grants, which started more recently than the recognition awards, shows better gender balance and approximates the gender distribution of WMS members. Despite possible changes in the gender balance of membership compared with earlier years, the process by which recognition and research awards are granted is worth several considerations described below.
Unlike many of the recognition awards, the proportion of female WMS grant winners (31%) was similar to that of the membership at large. The percentage of female WMS grant awardees is less than the proportion of female US scientific grant winners, but greater than the proportion of Canadian female grant winners over a recent 5-y period. 15 The WMS research grants and the research presentation awards are intended to be determined by a merit-based process with published award scoring criteria. This is in contrast to self and/or peer nominations for recognition awards, which may be at higher risk of bias for several reasons. One potential contributing factor to a lower representation of women is that they have been found to be less likely to self-nominate or be nominated by male colleagues, owing to a multitude of reasons that range from differences in how men and women evaluate their own performance to perceived risk of backlash. 16 Another reason may be unintentional or implicit bias in nomination letters and in consideration of eponymous awards with male names. 17 An additional source of bias may be the perpetuation of a cycle in which underrepresented groups remain underrecognized, while those holding society leadership positions gain organizational exposure and increase the likelihood that they will achieve recognition. 9 One way to minimize unintentional bias in the nomination and decision processes could include using explicitly predefined evaluation criteria, as is currently done for research presentations and grant awards, or to ensure a gender-blind selection process.14,18
Our data show that gender distribution for award and grant winners and conference attendees is similar over a similar time period. An important question remains: By what standard should we evaluate gender ratios? The 2019 Association of American Medical Colleges workforce data indicates that female/male gender balance in medical schools in the United States is currently near parity, but gender distribution varies by medical specialty. 19 Gender imbalance in the WMS may reflect the gender distribution of the medical specialties that are likely to participate in wilderness medicine. Emergency medicine has the highest representation within the WMS, followed by family medicine and prehospital providers, but the available data on WMS members’ specialties are insufficient for statistical comparisons. The gender distribution of the WMS 2020 membership snapshot is roughly similar to that of emergency medicine, which comprises 36% female residents and 28% practicing female emergency physicians. It is also similar to the distribution for prehospital providers, where emergency medical technicians and paramedics in the United States are 35 and 23% women, respectively. 20 The Association of American Medical Colleges reports that women make up 41% of family medicine physicians, 19 substantially higher than the proportion of female WMS members.
Wilderness medicine is in the company of many specialties that struggle to achieve gender equity. A niche field like wilderness medicine has specific challenges. For example, we do not know when factors that influence interest in wilderness medicine have the greatest impact. It is possible that women and men develop their interest in wilderness activities before medical school. Although outdoor industry data show that women comprise 46% of outdoor recreation participants, and that the percent of women involved in outdoor recreation increased every year from 2017 through 2019, 21 women involved in the WMS, using conference attendance as a proxy, has remained stable at around 30% over a similar time frame. This discrepancy suggests that women’s interest in wilderness medicine is not due to an inherent difference in men and women’s interest in outdoor activities. Other, as yet unidentified, gender differences may exist that impact exposure to wilderness medicine and contribute to fewer women being involved in the field. Likewise, gender balance may be influenced by a confluence of factors, including implicit bias, lack of diversity in leadership, and the belief that disparities do not exist and therefore need not be prioritized by the organization. 22 For wilderness medicine, the existing gender imbalance itself may perpetuate a reluctance for female students to pursue the field, as has been seen in other specialties.23,24
Minority status for women can create continued problems. At the member end, the underrepresentation of female physician members in specialty societies, as compared with their numbers in their respective fields, may reduce engagement and opportunity. Underrepresentation at the highest levels makes it harder for women to identify role models, perpetuates the status quo, and may result in unintended bias across society activities. Areas with extremely low proportions of women participants are particularly concerning as they can indicate hidden attitudes that exclude women. 9
Striving for the goal of gender equity is beneficial to medical societies and their members. 25 Professional societies with women in visible leadership roles have been shown to have greater gender equity throughout the society.12,26 Improved gender balance in leadership can generate a positive feedback cycle for women early in their careers by means of role modeling and mentorship, which can have an important influence on career guidance, research productivity, and personal development. 27 Evidence suggests that early career providers will remain loyal to medical societies that strive to adapt to their needs. 28 Efforts to improve diversity and inclusion will have a positive impact not only for members who are women, but can strengthen the organization as a whole. 29
Gender equity in the WMS could be addressed multiple ways. Outreach efforts can ensure that an adequate pipeline for women in the WMS is developed or expanded to encourage broad participation in science, research, publication, and teaching. Creating opportunities to attract and engage junior members can build the membership pool, which is critical to promoting long-term parity. Websites can be reviewed and conference and course programs developed to avoid unintended bias and ensure optimal promotion and reach. We appreciate the complexity of addressing equity and the challenges that exist in making progress in diversity and inclusion. Previous work has recommended that such efforts include a transparent process focused on metrics and outcomes that operates under the assumption that there will always be room for improvement. 19 Society membership surveys that assess perceptions, collect suggestions, and evaluate the effectiveness of efforts to improve inclusiveness are warranted. These should be part of ongoing data collection and reporting to support self-appraisal and identification of areas for improvement in gender equity.
Limitations
There were several limitations to this work. We evaluated different time periods across several measures. We sampled a 1-d snapshot of membership data, conference speakers over 5 y, conference attendance over 9 y, and board and award counts over the life of the award and/or organization. We used conference attendees as a proxy for membership; gender distribution of conference attendees may differ from that of members. We did not evaluate the number of unique conference speakers in gender proportion calculations, such as instances when one woman gave multiple presentations. We did not assess the unique weight of individual contributions, with equal units of credit given for each presenter listed on the conference schedule. The review of final selected speakers and award recipients did not include data on speaker proposals, speaker invitations, or award nominees. The automated tool we used for gender classification only classifies names as “female” or “male” based on statistical likelihoods drawn from self-reporting, which did not address representation of other gender groups. In addition, the tool derives statistical likelihoods based on localized data from global sources, such that some names may be misclassified on the basis of localization (eg, “Jan” may be more likely to be male in Europe, but female in North America). Data on self-identification should be collected directly from community members to best represent individuals’ gender identities. Future studies would benefit from consistent data availability across similar time periods.
Conclusions
Our findings add to a larger collective effort to evaluate and advance gender balance in science and medicine. We hope that these data will help WMS efforts to enact its values statement in policy. Although it is only one of the many components of equity, identifying successes and future opportunities for gender balance can strengthen the WMS base, promote growth, and ensure a strong leadership pipeline.
Footnotes
Acknowledgements
Author Contributions: Study concept and design (SMS, LEK, NWP); data acquisition (SMS, NWP, NEP, ABB, AB, LK); data analysis (SMS, LEK, NWP, NEP, ABB); drafting and critical revision of the manuscript (SMS, LEK, NWP, NEP, ABB); approval of the final manuscript (all authors).
Disclosures: Linda E. Keyes is past president of the WMS, Neal W. Pollock was editor-in-chief of WEM at the time of writing, and Alicia Byrne is managing editor of WEM. No authors were involved in the process of peer review or the editorial process of this manuscript.
Financial/Material Support: None.