
Abstract
Owing to multiple factors, human-wildlife interactions are increasing, and conflict can result in fatal injuries. A 21-y-old man was brought to the emergency department in critical condition with 2 puncture wounds over the thoracoabdominal region after a nilgai, or blue bull (Boselaphus tragocamelus), had gored him. The patient sustained double gastric perforation, which was managed laparoscopically and complicated by an abscess formation in the lesser sac 1 wk later, which required further surgical exploration. The operative culture showed growth of Klebsiella pneumoniae. Intravenous antibiotics were given as per the culture sensitivity report, and the patient improved. Many horn injuries are described as puncture lacerated wounds owing to the rugged nature of animal horns. However, in this case, the margins of the wound were regular and incision-like owing to the smooth and straight structure of blue bull horns. Early surgical exploration and monitoring of treatment progress are crucial in reducing morbidity in penetrating horn injuries.
Introduction
The blue bull, or nilgai (Boselaphus tragocamelus), is the largest Asian antelope and is classified in the same bovid family as domestic cattle, antelope, and buffalo. The nilgai is endemic to the Indian subcontinent and was introduced to Texas in the 1920s for trophy hunting. The average weight of an adult nilgai is 200 kg, with a shoulder height of about 130 cm. 1 They have a stable population and are considered as least concern in the International Union for Conservation of Nature red list of threatened species. 2 The adult male is blue-gray (Figure 1), and the adult female and juveniles are light brown. Only males have horns, and the usual length of an adult nilgai’s horn is 15 to 20 cm. 1 Nilgai mainly inhabit scrublands, low hills, grassy plains, and near agricultural fields; hence, close encounters usually occur in agricultural settings. 3

Nilgai in a farm field taken at Jodhpur, India (representational image). Photo credit: Mohanraj Kolathapilly.
Although nilgai attacks have been occasionally reported in the press, none have been documented in the medical literature. 4 We present a case of an individual who sustained unexpected penetrating injuries from this wild bovine. The unusual pattern of nilgai horn injury and related medical implications are discussed.
Case Report
A 21-y-old male was brought to the emergency department unresponsive and in critical condition owing to puncture wounds in his abdomen and right axilla. Initial vital signs were as follows: blood pressure 96/60 mm Hg, heart rate 112 beats‧min-1, temperature 36.5°C, and oxygen saturation 100% on room air. After fluid resuscitation, the patient regained consciousness and reported that he had been attacked by a nilgai while working on his farm. The man was a farmer who had attempted to scare a nilgai away from his land, causing the animal to attack.
Physical examination revealed an elliptical-shaped puncture wound measuring 4 cm × 1 cm over the upper epigastrium. The omentum was visible in the wound gap. The margins of the wounds were clean and regular without associated contusions (Figure 2A). The epigastric wound was temporarily closed with silk suture in the emergency department. Another puncture wound measuring 2 cm × 0.5 cm, muscle deep, was present in the right axilla, with clean and regular margins (Figure 2B). The right axillary puncture wound was superficial, so simple primary closure was completed. There were grazed abrasions on the back of the right elbow (7 cm × 5 cm) and the back of the left elbow (4 cm × 3 cm). Intramuscular injections of tetanus toxoid and diclofenac were given. Intravenous ceftriaxone and metronidazole were started for empiric coverage. A computed tomography scan of the thorax and abdomen revealed mild to moderate pneumoperitoneum (Figure 3A) with mild free fluid in the abdomen (along the lesser sac and gastrohepatic ligament as well as in the perihepatic and perisplenic regions). A defect of 3.4 cm × 1.1 cm with omental herniation was seen in the epigastrium 3 cm distal to the tip of the xiphoid process (Figure 3B). A suspicious rent was seen in the gastric body, with adjacent air and fluid pockets. No other visceral injuries were seen in the scan. Initial laboratory blood test results were as follows: hemoglobin 15.9 g‧dL-1, white blood cell count 13,560/uL, and hematocrit 47%. After examination and investigations, the diagnosis of gastric perforation with peritonitis was made.
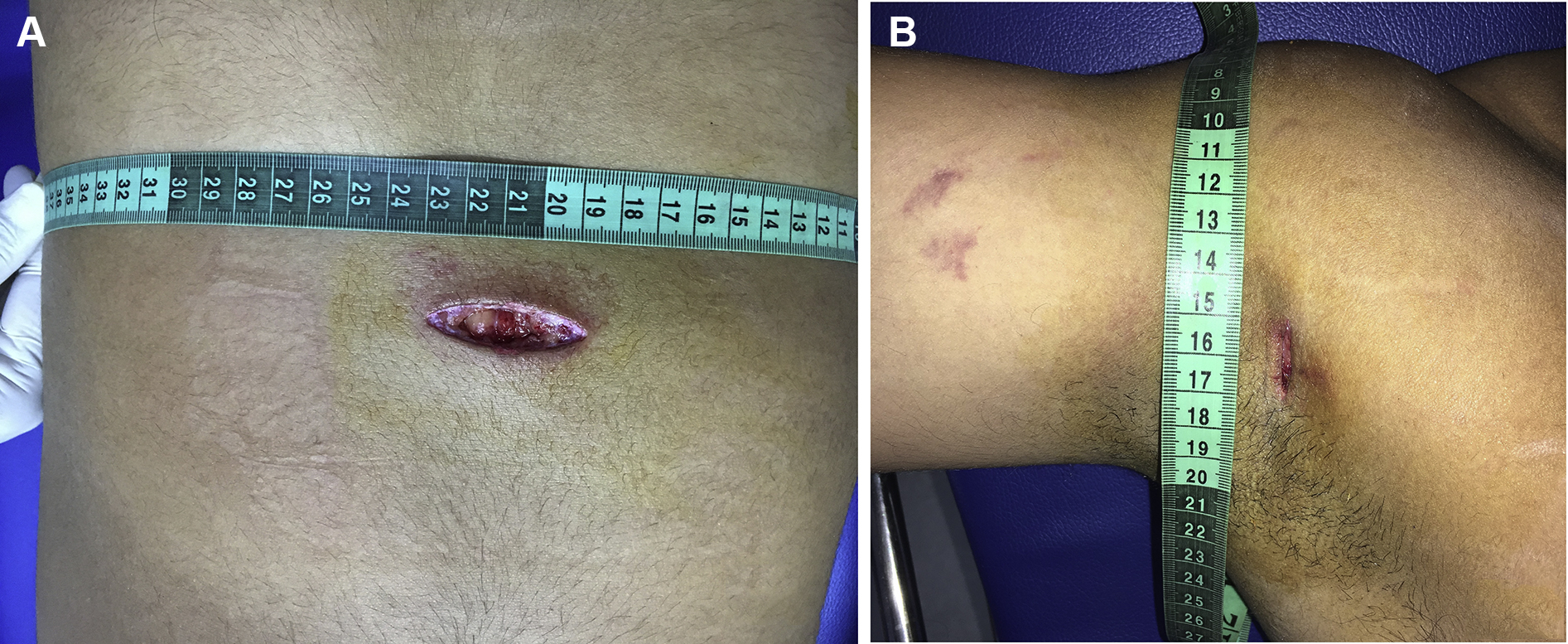
Two puncture wounds sustained on a single impact by the nilgai head. An elliptical shaped over the upper abdomen (A) and another slit-like in the right axilla (B).
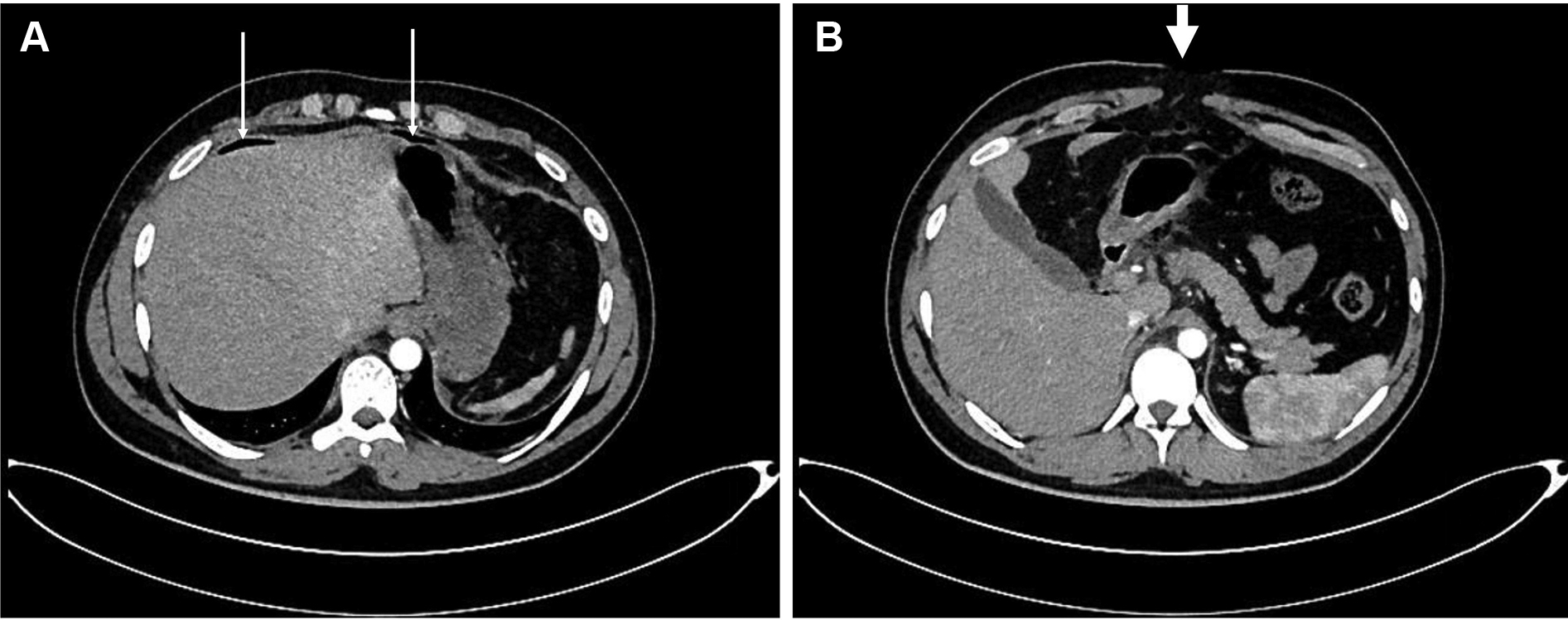
Computed tomography images of the abdomen. (A) Pneumoperitoneum (thin arrows). (B) The site and direction of the penetrating injury (thick arrow).
The patient underwent surgery on the second day and was managed with laparoscopic primary repair of gastric perforations and peritoneal wash. The gastric perforations in the anterior wall (1.5 cm × 1 cm) and posterior wall (1 cm × 1 cm) were near the lesser curvature corresponding to the anterior abdominal wall defect.
Eight days postoperatively, the patient developed abdominal pain, distension, and tenderness. His hemoglobin level fell to 10.9 g‧dL-1, white blood cell count increased to 22,900/uL, and a computed tomography scan revealed a 300 mL abscess in the lesser sac. He underwent exploratory laparotomy, and a loculated pus collection in the lesser sac was removed and sent for bacterial culture and sensitivity. The culture showed growth of Klebsiella pneumoniae. Intravenous antibiotics piperacillin/tazobactam, amikacin, and metronidazole were given for the next 7 d. The patient was recovering well and was advised discharge on hospital day 18. The patient remained in the hospital for an additional 5 d for continued wound care and monitoring and was ultimately discharged on day 23 with no further complications.
Discussion
Human casualties from human-wildlife conflicts in India occur mainly in agricultural settings. 5 Recent data from India’s national crime records bureau show that 1425 people were killed by animal attacks in 2019, excluding deaths caused by poisonous and venomous animals. 6 Elephants and tigers are responsible for most wildlife conflicts in rural India. Other wild animals such as jackals, leopards, and wild boars cause a small percentage of attacks.5,7 Most reported attacks by Bovidae are caused by domestic bulls and cattle and are sustained by dairy workers, farmers, and people involved in the practice of bullfighting. 8 These animals usually inflict blunt trauma and penetrating injuries to the abdomen, perineum, and lower limbs. 9 -11 Blunt trauma occurs when a person is butted by the animal’s head or sustains a subsequent fall to the ground. Other mechanisms of blunt force trauma are kicking or trampling by the animal. 8 Penetrating injuries are due to direct goring by the animal’s horns. 11
Penetrating injuries caused by animal horns are of various sizes and shapes. These wounds are usually associated with adjacent bruising and lacerations of soft tissue.10,11 In this case, the epigastric wound was elliptical with clean regular margins and no associated bruising. This was due to the smooth, pointed, and near-straight structure of nilgai horns. 1 Because the horns of other wild animals and domestic cattle are usually ragged or curved, they are associated with bruising and lacerations of wound margins.
In this case, the stomach’s entry and exit wound were near the lesser curvature, fortunately sparing the liver and vasculature. However, the patient developed an abscess in the lesser sac 1 wk after the first surgery. He underwent exploratory laparotomy, and bacterial culture showed growth of K pneumoniae. K pneumoniae is ubiquitous in the environment and also resides in the oropharynx and gastrointestinal tract. 12 In the present case, there was a persistent gastric leak for 1 d after traumatic perforations because the patient underwent laparoscopic repair on the second day. The initial contamination from the gastric leak led to peritonitis and is the most likely cause for the subsequent abscess formation.
An overall wound infection rate of 13% was found in a study of 101 patients with bull horn injuries in south India. 9 In horn injuries, the introduction of organic contaminants such as grass and dirt into the puncture wound may contribute to the infection, although wound culture data from goring injuries are sparse. Surgical exploration with removal of foreign bodies and debris and wound irrigation is the standard of care. 11 Despite the internal organ injuries and infection risk, the prognosis is favorable in most cases. 13 In the present case, significant morbidity developed during a hospital stay, managed with surgery and appropriate medical care.
This case report highlights isolated goring injuries caused by a nilgai attack. Nilgai attacks on humans are rare because they are timid animals and quickly run away when threatened. The population of nilgai has increased in some Indian states after the introduction of the wildlife protection act in 1972. 14 This act includes provisions that prohibit wildlife hunting. Because nilgai prefer grass and herbs, they frequently migrate into agricultural areas. Conflicts occur between farmers and nilgai due to habitat loss and, more importantly, unwelcome entry into farms, where they can cause significant damage. 3
Conclusions
Gore wounds are serious injuries owing to variable depth of penetration, risk of infection, and internal organ injuries. Computed tomography helps assess wound extension, but the standard of care if an object penetrates the peritoneum is surgical exploration of the wound. The prognosis is favorable in most cases when wounds are managed surgically. Gore wounds from nilgai may be particularly prone to cleaner margins but can result in deep penetrating injuries owing to the structure of their horns.
Footnotes
Acknowledgements
Author Contributions: Examination of patient and study concept (AG, DJ); literature review, data collection and editing of the manuscript (AG, RSS); approval of final manuscript (AG, DJ, RSS).
Financial/Material Support: None.
Disclosures: None.