
Abstract
Stingrays are found in open waters and are also kept in exhibits in many aquariums throughout the world. They are generally nonaggressive creatures by nature, but they can inflict injuries with their spines if provoked. We present a case of a 62-y-old diver who was pierced in the chest by the barb of a stingray while transferring the animal to another tank as part of his work in a public aquarium. He was rescued immediately from the tank but was found to be in cardiac arrest. Bystander cardiopulmonary resuscitation was promptly initiated by his colleagues. He was rapidly evacuated to the nearest emergency department, where he was noted to be in pulseless electrical activity. A single puncture wound was noted over the right second intercostal space, with the spine of the stingray still impaled in the chest. Trauma surgeons were activated promptly, and resuscitation was continued based on advanced cardiac and trauma life support guidelines, which included ongoing cardiopulmonary resuscitation, securing the airway, and emergency blood transfusion. An emergency department thoracotomy was performed, but despite aggressive resuscitation the thoracic injury was fatal. An autopsy revealed transection of the aorta by an impaled barb. We present a review of stingray injuries and suggest a general approach to management.
Introduction
Stingrays are marine creatures that belong to the Chondrichthyes class, along with sharks. They are found in both shallow and deep waters and are kept in exhibits in many aquariums worldwide. They are broad and flat, with a whip-like tail containing 1 or more barbed stingers. They are generally noted to be nonaggressive, but they can inflict injuries with their stingers as a mechanism of self-defense if provoked. 1 In addition to the trauma from a puncture wound, the stinger contains secretory venom cells and glands that may cause toxic effects to its victim. There are about 1500 to 2000 emergency department (ED) visits related to stingray injuries annually in the United States. 2 We report a fatal case of a penetrating thoracic injury caused by a stingray. A review of stingray injuries and an approach to their management will be discussed.
Case Report
A 62-y-old veteran diver, expert marine animal handler, and aquarium employee was part of a team transferring stingrays when he was pierced in the chest by a stingray. The animal was a leopard whiptail ray, Himantura leoparda, measuring 1.0 m in width and 1.8 m in length. He was rescued immediately from the aquarium by his colleagues, who noted that he was pulseless. They started bystander cardiopulmonary resuscitation (CPR) promptly and contacted the emergency ambulance service.
When paramedics arrived, the patient was noted to be in traumatic cardiac arrest with an initial rhythm of pulseless electrical activity (PEA). He was rapidly evacuated to the nearest ED with CPR continued en route. On arrival in the ED, he continued to be in PEA with a total downtime of 18 min. Resuscitation was continued as per advanced cardiac life support and advanced trauma life support protocols while the trauma team was activated. During the resuscitation, a total of 8 doses of intravenous adrenaline (1 mg each), 1 L of normal saline, and 1 unit of emergency packed red cell transfusion were given, but there was no return of spontaneous circulation.
A single puncture wound was found over the right second intercostal space (Figure 1). An ED thoracotomy was promptly performed by a senior trauma surgeon to attempt direct intrathoracic hemorrhage control, evacuate any cardiac tamponade, and perform open cardiac massage. A long barb was seen in the intrathoracic space (Figure 2). However, because there was no cardiac contractility nor any massive hemothorax or pericardial effusion to treat, the decision was made to terminate resuscitation.
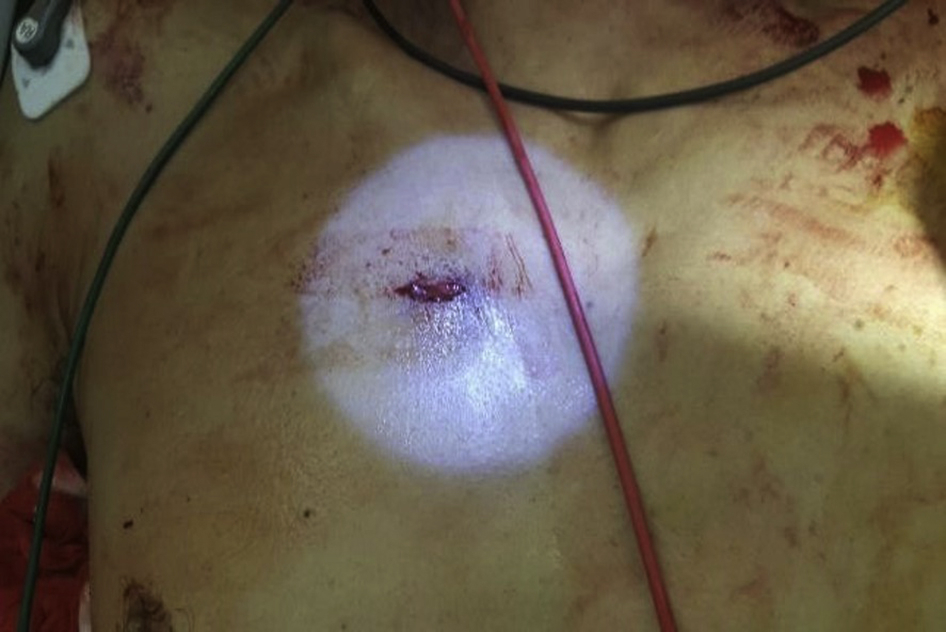
A puncture wound on the right second anterior intercostal space.
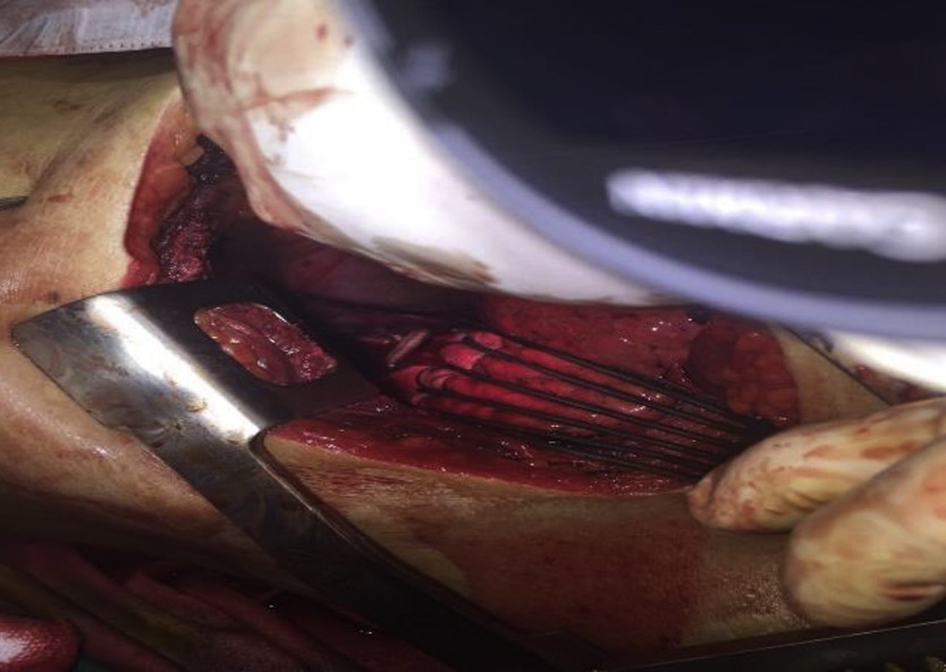
Emergency department thoracotomy revealing a stingray barb at the intrathoracic space.
An autopsy revealed a stinger penetrating the right second intercostal space, transecting the ascending aorta, pericardium, left atrium, descending aorta, and diaphragm and exiting from the posterior left seventh intercostal space (Figure 3). The stinger measured 22.5 cm.

A stingray barb exiting from left seventh posterior intercostal space.
Discussion
Most stingray injuries involve the extremities, more commonly the lower limbs than the upper limbs, 2 and rarely involve the thorax and abdomen. 1 Victims are usually stung on their lower limbs when they accidentally step on stingrays while walking in shallow waters. Some may be stung on the torso while swimming or diving in deep waters near stingrays.
Stingray injuries can be twofold: the mechanical effect of the stinger as it penetrates tissues and envenomation from toxins released from its venom glands. 3 The mechanical damage results from the cutting action of the serrated stinger, which lacerates and damages the underlying soft tissue. This may cause severe injuries and death if vital organs such as the heart, lungs, great vessels, liver, spleen, and bowels are involved. 3 In our case, the cause of death was likely exsanguination from the aorta and left atrium. Venom may also be released from the secreting glands on the barb, resulting in envenomation with serotonin, phosphodiesterase, 5’-nucleotidase, vasoconstrictor agents, and several other unidentified components. 4 This may cause local effects such as intense pain and necrosis of the wound, as well as systemic effects such as salivation, nausea, vomiting, diarrhea, dyspnea, cardiac arrhythmias, and seizure. 5 One study demonstrated that the cardiotoxic effects can result in myocardial inflammation, heart block, or even cardiac standstill. 6
Most extremity wounds can be managed with warm water immersion and basic wound care in the ED because most venom is heat labile and can be denatured by warm water (42–46°C) within 30 to 90 min.1,5 A retrospective review of clinical presentations and treatments of 119 stingray envenomations showed complete pain relief with warm water immersion alone within 30 min in 88% of patients presenting within 24 h of injury, with no thermal complications noted. 2 This is further supported by another study 7 that showed that 69% of patients had improvement in pain within 1 h of initiation of warm water immersion. However, the theory of denaturation has been questioned by many experts, who argue that such direct denaturation would require temperatures so high as to result in burns and tissue necrosis in the patient. 8 An alternative theory is that hot water immersion causes modulation of pain receptors in the nervous system, leading to a reduction in pain. 8
The wound may also be exposed to numerous pathogenic microbes, including Vibrio, Streptococcus, Staphylococcus, Aeromonas, and Clostridium species, via the barb and surrounding aquatic environment. 9 Two studies respectively reported that 17% and 5% patients who did not receive prophylactic antibiotics experienced complications of wound infection.2,9 In general, the majority of patients who sustain stingray injuries can be discharged from the ED with analgesia, prophylactic antibiotics, tetanus vaccination, and wound care advice without major complications. 2
There is no antidote for stingray venom, and its systemic effects can only be managed by supportive treatment such as wound management and systemic resuscitation. 1 The management, however, is more complicated if the penetrating injury involves the torso, including the thoracic and abdominal regions, because the mortality rate of penetrating torso injury is very high. 10 –12 A combination of prompt resuscitative efforts based on advanced trauma life support principles, ED thoracotomy when indicated, and early definitive surgical intervention has been shown to provide the best chance of survival in such situations.
There are 2 recent case reports of survivors of neck 13 and thoracic 14 injuries, respectively. The first case report 13 describes a patient with a small entrance wound on his neck from a stingray that caused a missed traumatic pneumothorax, which was subsequently discovered and treated with chest tube insertion and wound debridement. Another case report 14 describes a patient with a thoracic stingray injury that caused a hemopneumothorax and pneumomediastinum. The patient survived with prompt treatment, which included chest decompression by inserting a fillet knife into the fifth intercostal space on the midaxillary line at scene, chest tube insertion at a local hospital, and stinger removal and segmental lung resection at a thoracic surgery center.
To the best of our knowledge, this is the first reported stingray injury that involved aortic transection and ED thoracotomy. In our case, the patient had a penetrating thoracic injury with signs of life as evidenced by PEA on the electrocardiogram on arrival, thereby fulfilling the indication for an ED thoracotomy. A review of studies 15 showed that the overall survival rate for penetrating thoracic trauma with ED thoracotomies performed is 9 to 12%. In the literature review, there are only 3 survivors of penetrating cardiac injuries by stingrays. 16 –18 However, the barb did not transfix the cardiac chamber in the first 2 cases,16,17 involving the right ventricle muscle and right coronary artery, respectively.
The most recent reported case 18 involved transfixing cardiac injuries on both ventricles, compared to our case which involved left atrium and ascending and descending aorta. That patient reportedly survived as a result of the integrated trauma system, with rapid transport by the prehospital provider, initial stabilization by the surgical staff at the receiving facility, and expeditious referral to the trauma center for definitive care. 18
Conclusions
Most stingray injuries are minor and can be managed with supportive treatment in the ED. However, penetrating torso injury requires a combination of prehospital support and prompt evacuation to a tertiary trauma center due to the potential of a fatal penetrating injury. Sustained ED resuscitation effort and rapid definitive surgical intervention are important.
Footnotes
Acknowledgements
Author contribution: Major contributor in writing manuscript, literature searching, and case description and involved in the clinical management of this case (HKL); primary provider of this case who managed this patient and contributed to case description (IC); toxicologist who provided expert opinion and critical revision of article (RP); all authors read and approved final manuscript.
Financial/Material Support: None.
Disclosures: None.