
Abstract
Stingray envenomation is common in coastal regions around the world and may result in intense pain that can be challenging to manage. Described therapies involve hot water immersion and potentially other options such as opioid and nonopioid analgesics, removal of the foreign body, wound debridement, antibiotics for secondary infection, and tetanus toxoid. However, for some patients, this may not be enough. Peripheral nerve blockade is a frequently used perioperative analgesic technique, but it has rarely been described in the management of stingray envenomation. Here, we report a case of stingray envenomation in an otherwise healthy 36-y-old male with pain refractory to traditional therapies. After admission for pain control, the patient received an ultrasound-guided sciatic popliteal nerve block. Upon completion of the peripheral nerve block, the patient reported rapid and complete resolution of the intense pain, which did not return thereafter.
Introduction
Stingray envenomation is common along coastal regions of the United States, with approximately 2000 cases reported annually.1,2 The barb from the stingray punctures the patient’s skin, releasing a venom containing serotonin, 5’-nucleotidase, and phosphodiesterase, which can ultimately lead to intense pain and peripheral vasoconstriction. 3 Untreated, the envenomation and barb migration can lead to infection, soft tissue necrosis, organ perforation, gangrene, cardiac dysrhythmias, and even death. 3 -5 Significant long-term complications from envenomation have also been reported, including chronic pain and complex regional pain syndrome. 6 -8 Initial treatment involves hot water immersion (HWI) at approximately 40 to 45°C, although a more recent study suggests 43 to 45°C is optimal, 9 for up to 90 min to denature the heat-labile venom proteins.1,4,10 Other options include pharmacologic pain management, antibiotics for secondary infection, tetanus toxoid, and foreign body removal/debridement.1,4,10 The pain associated with the sting can be debilitating, challenging to manage, and potentially resistant to common analgesic medications. Here, we report a case of refractory pain due to envenomation by a southern stingray (Hypanus americanus), a species native to the east coast of the United States. The patient was treated with a popliteal sciatic nerve block. After the ultrasound-guided popliteal sciatic nerve block was performed, the patient achieved immediate and long-lasting pain relief.
Case
An otherwise healthy, opioid naïve, 36-y-old male presented to the emergency department with severe pain in his left ankle after being stung by a stingray while surfing in the Atlantic Ocean off the coast of Virginia Beach, Virginia. The patient reported immediately feeling a sharp and shooting pain over his left lateral malleolus. Shortly thereafter he was brought to the emergency department and over the next 3 to 4 h, his lower leg became erythematous, edematous, and exquisitely tender to palpation. He was initially examined for signs of retained foreign body and received HWI (>40°C, exact temperature unclear) therapy for a little over 80 min without improvement. Because the patient continued to report little improvement in his pain after 80 min of HWI, he was given 4 mg of intravenous morphine, 1000 mg of intravenous acetaminophen, and 15 mg of intravenous ketorolac. X-rays performed in the emergency department did not reveal any signs of fracture, dislocation, or foreign body (possibly not visible given the small size and cartilaginous nature of the spine).
At approximately 8 h after initial injury, the patient reported persistent intense pain despite prior interventions. At this point, he was admitted for pain control and the acute pain service was consulted for assistance with management. After the orthopedics services reported the injury as being low risk for the development or masking of compartment syndrome, the acute pain service team elected to perform a peripheral nerve block. Ultrasound-guided sciatic nerve block was performed via the popliteal fossa approach. The sciatic nerve was easily identified sonographically in the popliteal fossa and followed to the bifurcation into the common peroneal nerve and tibial nerves (Figure 1A). Under ultrasound guidance, 20 mL of 0.5% ropivacaine was injected in 5 mL aliquots around the nerve directly proximal to the sciatic nerve bifurcation. Immediate relief was achieved after the procedure and continued for the duration of the hospital stay. The patient was started on intravenous cefazolin and doxycycline for secondary infection prophylaxis and was monitored on the internal medicine ward overnight. After 24 h, the patient met discharge criteria with adequate pain control and without signs or symptoms of infection. He was able to ambulate without assistance after resolution of the peripheral nerve block approximately 20 h into admission.
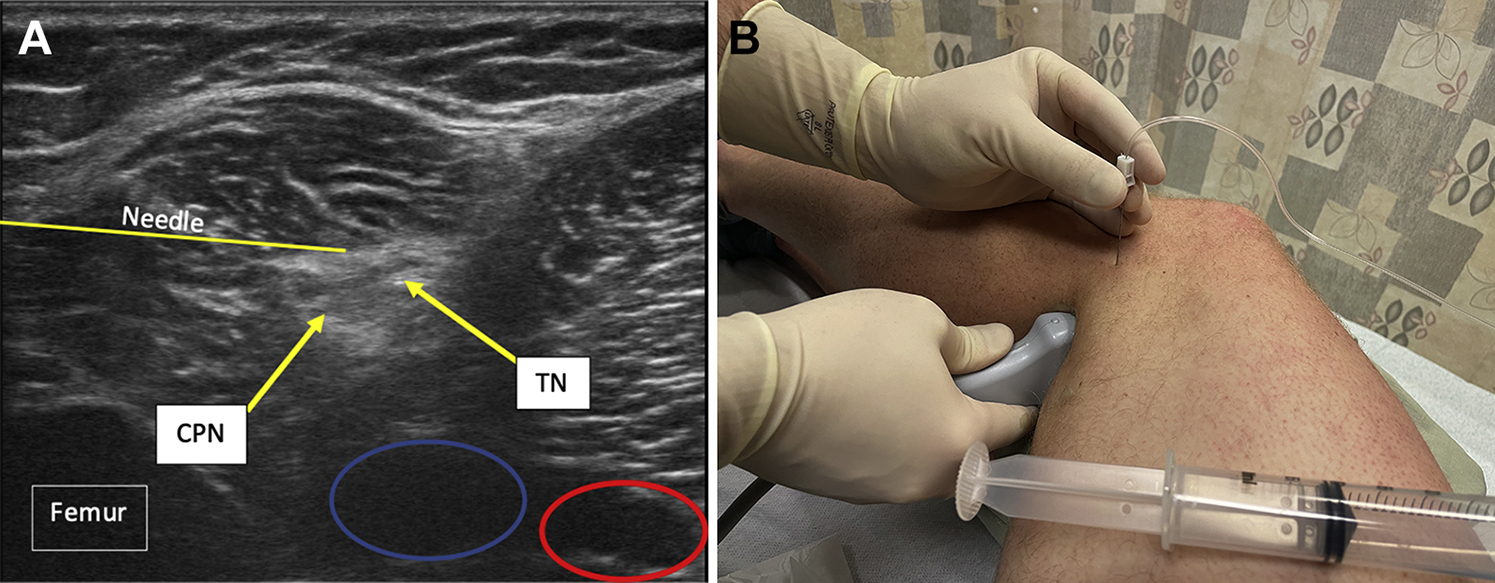
(A) The image on the left shows the ultrasound anatomy of the left sciatic nerve just above the popliteal fossa at the beginning of the sciatic nerve bifurcation into the tibial nerve and common peroneal nerve. Just deep and medial to the tibial nerve and common peroneal nerve are the popliteal vein and artery, circled in blue and red, respectively. (B) The patient is shown in the right lateral decubitus position. An ultrasound-guided sideline popliteal sciatic nerve block is performed with the needle entering from a lateral approach in plane with the ultrasound probe, with local anesthetic deposited around the nerve.
Discussion
The pain from stingray envenomation is potentially debilitating. Although first-line strategies are usually effective, 1 regional anesthesia offers an additional tool for pain control. In our case, the use of HWI in addition to pharmacologic adjuncts was not sufficient to achieve adequate pain control. Although the HWI temperature may have been inadequate to neutralize the venom in this case, peripheral nerve blockade might still be considered in other patients for whom HWI at temperatures of 43 to 45°C is ineffective. 9 That said, regional anesthesia techniques are rarely described for stingray envenomation. Local anesthetic infiltration into the wound site has been described, and 1 other case involving the use of a peripheral nerve blockade was reported, although an upper extremity peripheral nerve block was used.11,12 Regional anesthesia has significantly changed since the initial description in the 1880s, with improvement in technique and performance due to ultrasound and modern local anesthetics.13,14 In patients with challenging pain control, such as the combat wounded during the recent wars in Iraq and Afghanistan, regional anesthesia was critically important and effective.15,16 Regional anesthesia has been described in austere environments outside of the operating room, 17 as well as in the emergency department. For qualified providers in the emergency department, regional anesthesia has been used for patients with hip/femur fracture, shoulder reduction, extremity trauma, and rib fractures.1,18,19 Furthermore, the ongoing opioid crisis has demonstrated the need for increased utilization of regional techniques for opioid minimization.20,21
After stingray envenomation, pain typically reaches its peak within 30 to 90 min of injury and can last 48 h if untreated. 22 Long-acting local anesthetics such as bupivacaine or ropivacaine could offer analgesic benefit during this time period. Because of the ease of performance of peripheral nerve blocks and the low side effect profile, regional anesthesia should be considered for stingray envenomation refractory to traditional first-line treatment. In addition, peripheral nerve blockade often leads to increased blood flow due to disruption of sympathetic innervation to the local vasculature. 23 -25 Theoretically, increased regional perfusion could lead to decreased clinical duration of pain through redistribution of stingray toxins away from the local envenomation site.
Conclusions
We report the use of a popliteal fossa sciatic nerve block for symptomatic treatment of stingray envenomation in a patient with severe refractory pain. The literature supports the use of regional anesthesia for this purpose, however, there is scant evidence for its use. The relative ease of placement and safety of peripheral nerve blocks make their use a potentially valuable tool for such patients.
Footnotes
Acknowledgements
Author Contributions: HRD, SBH, JHC, and SBH all contributed equally to the patient identification and manuscript preparation. All authors approved the final form of the manuscript.
Financial/Material Support: None.
Disclosures: The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government. LT DeYoung is a military service member. This work was prepared as part of his official duties. Title 17 U.S.C. 105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. 101 defines a United States Government work as a work prepared by a military service member or employee of the United States Government as part of that person’s official duties.